
Advancing Surgical Arrhythmia Ablation: Novel Insights on 3D Printing Applications and Two Biocompatible Materials


 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Selection of 3D Printing Material
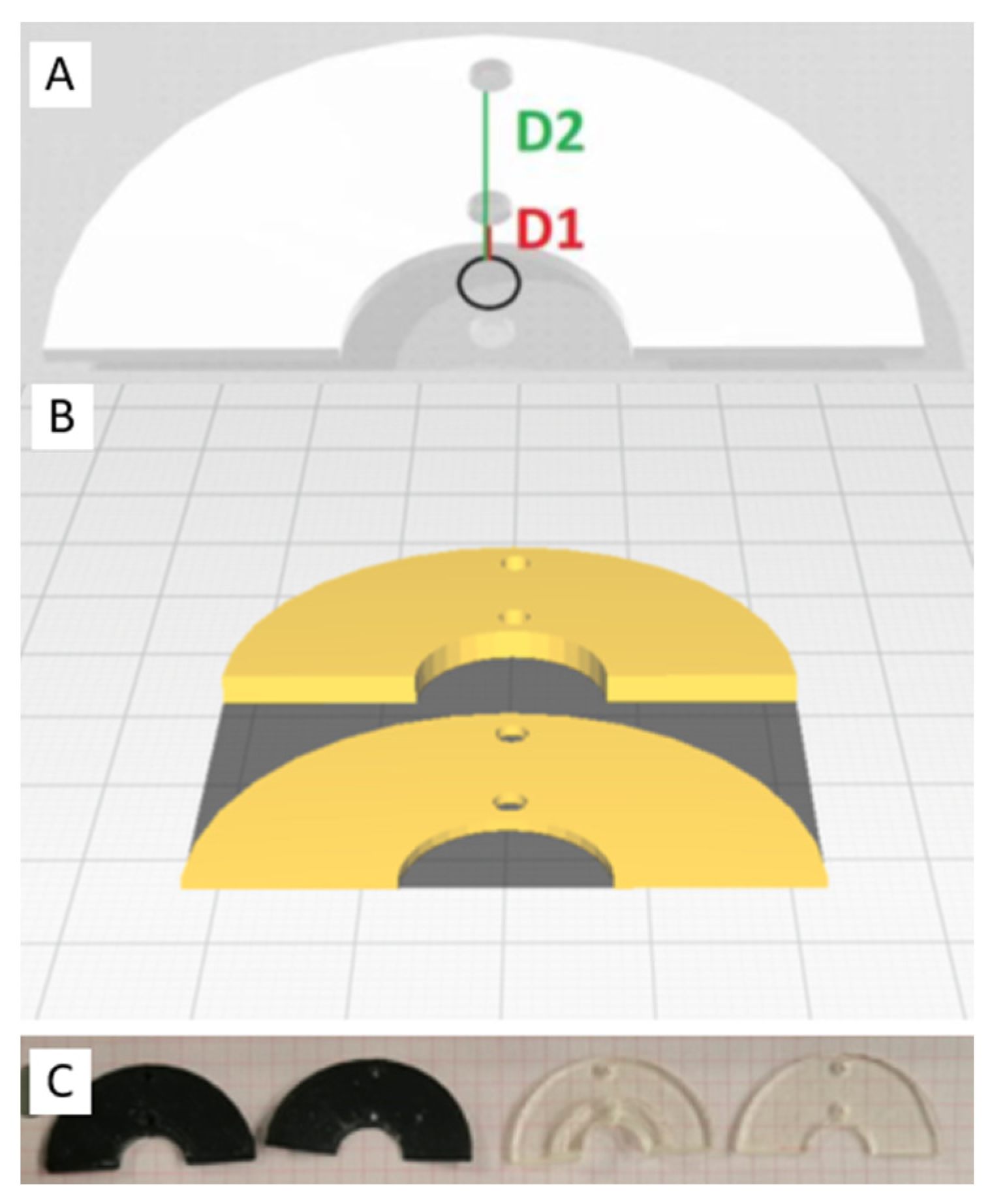
Material Sterilization and Geometry Testing
2.2. In Vitro Ablation Experiment
2.3. Type of Energy Delivery
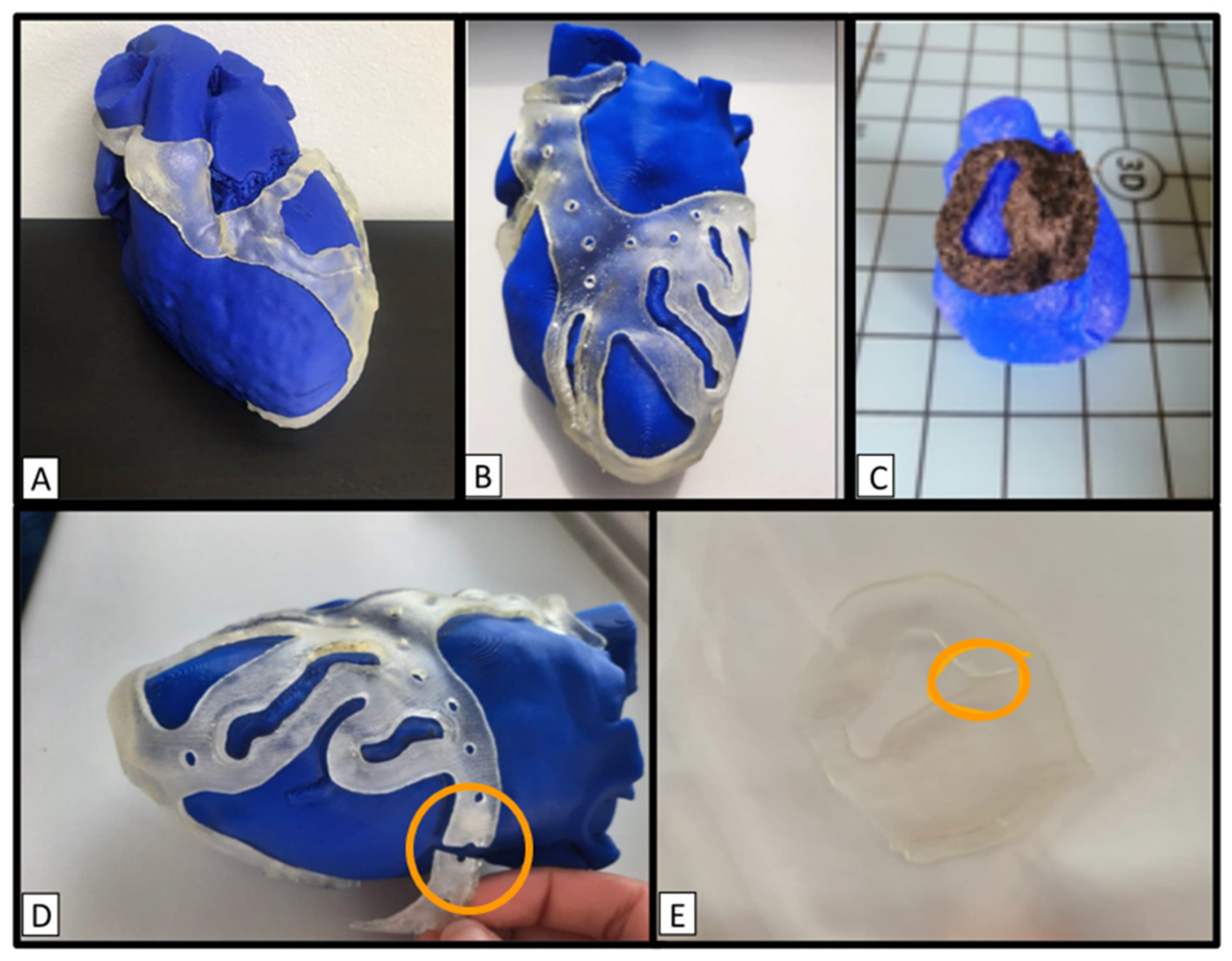
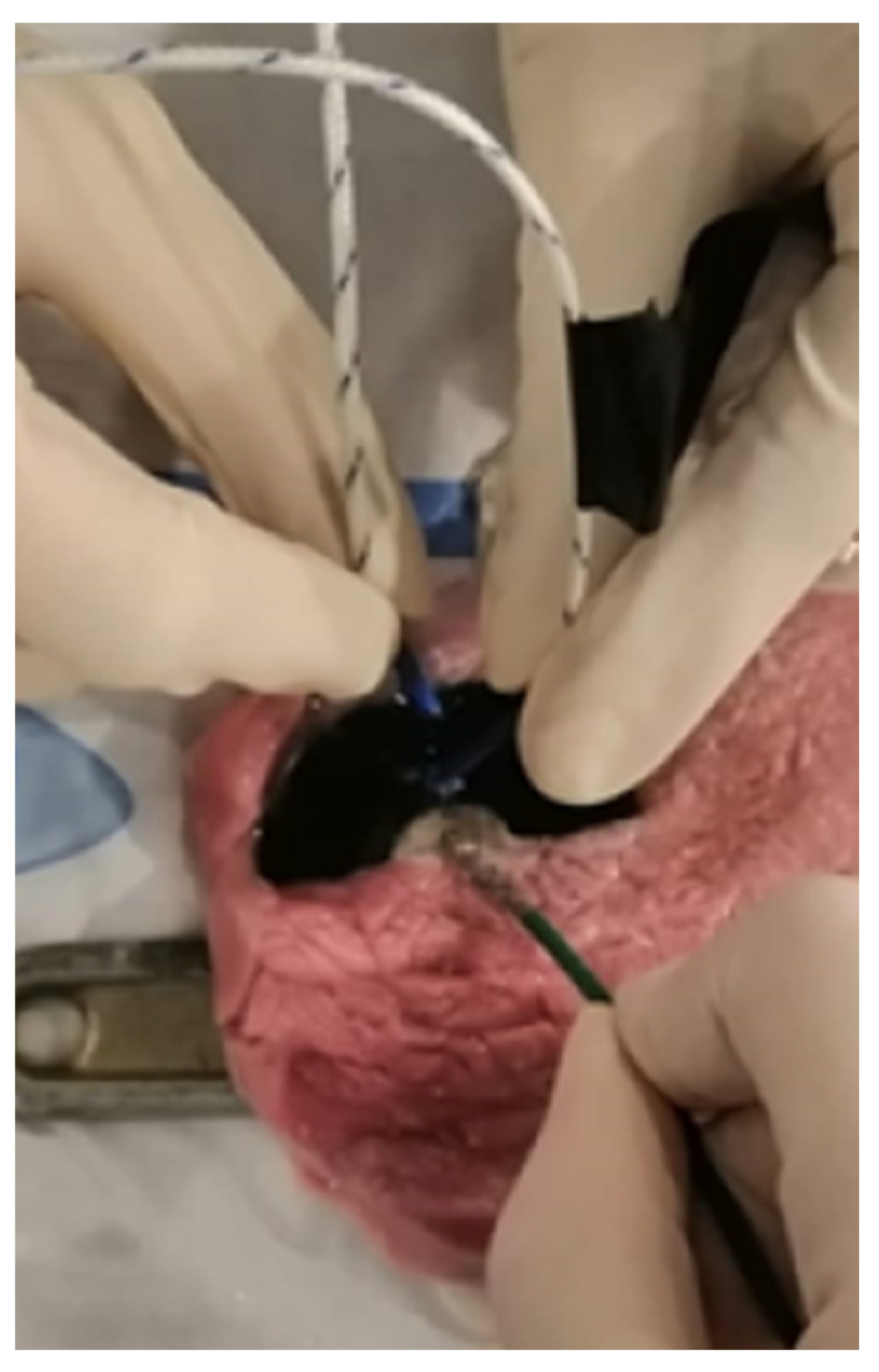
2.4. Experimental Setup
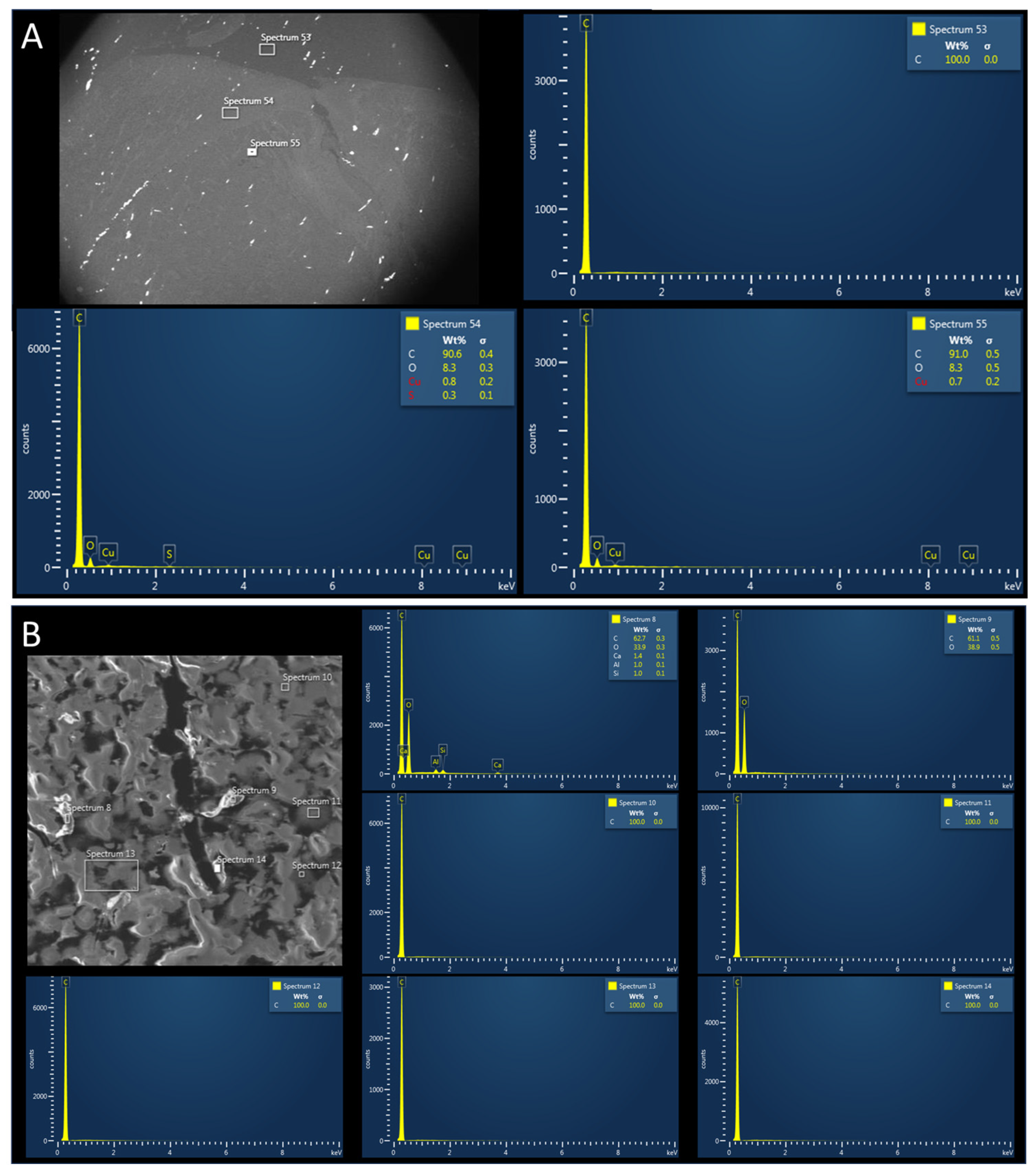
2.5. Post-Procedural Tissue Analysis
2.6. Statistical Analysis
3. Results
3.1. Geometry Test after Sterilization
3.2. In Vitro Ablation
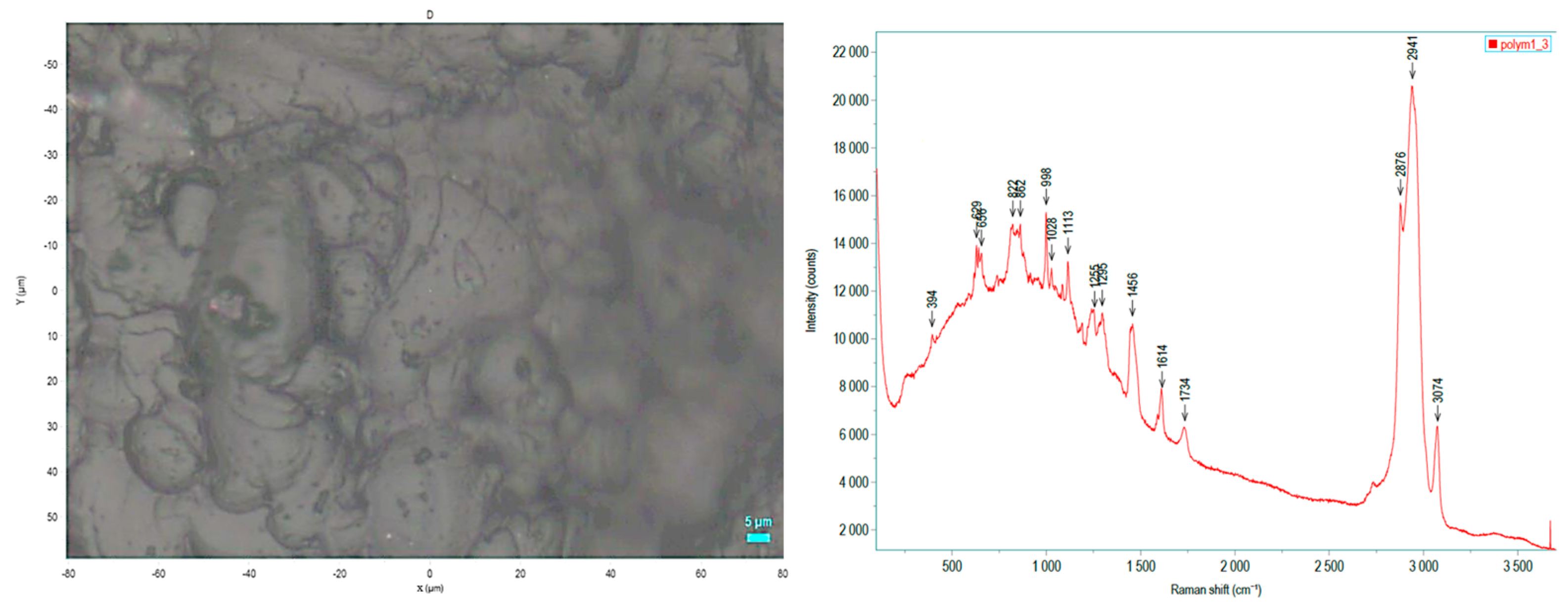
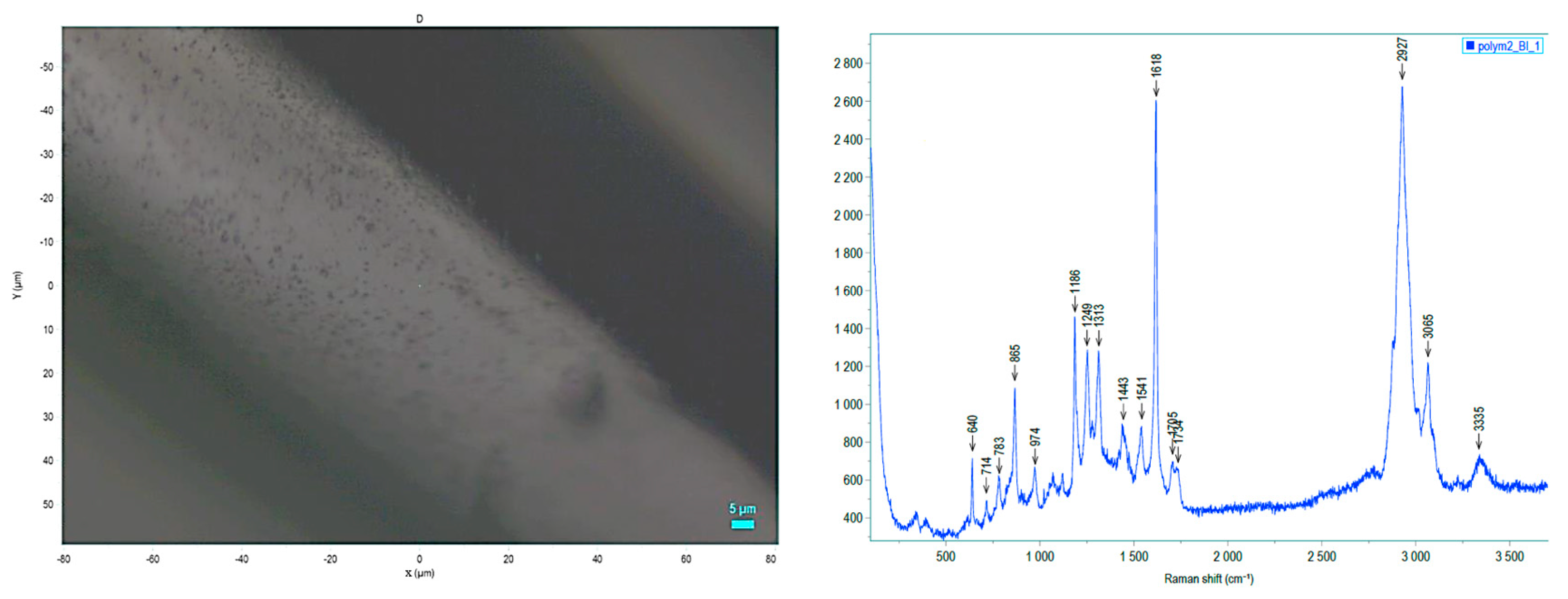
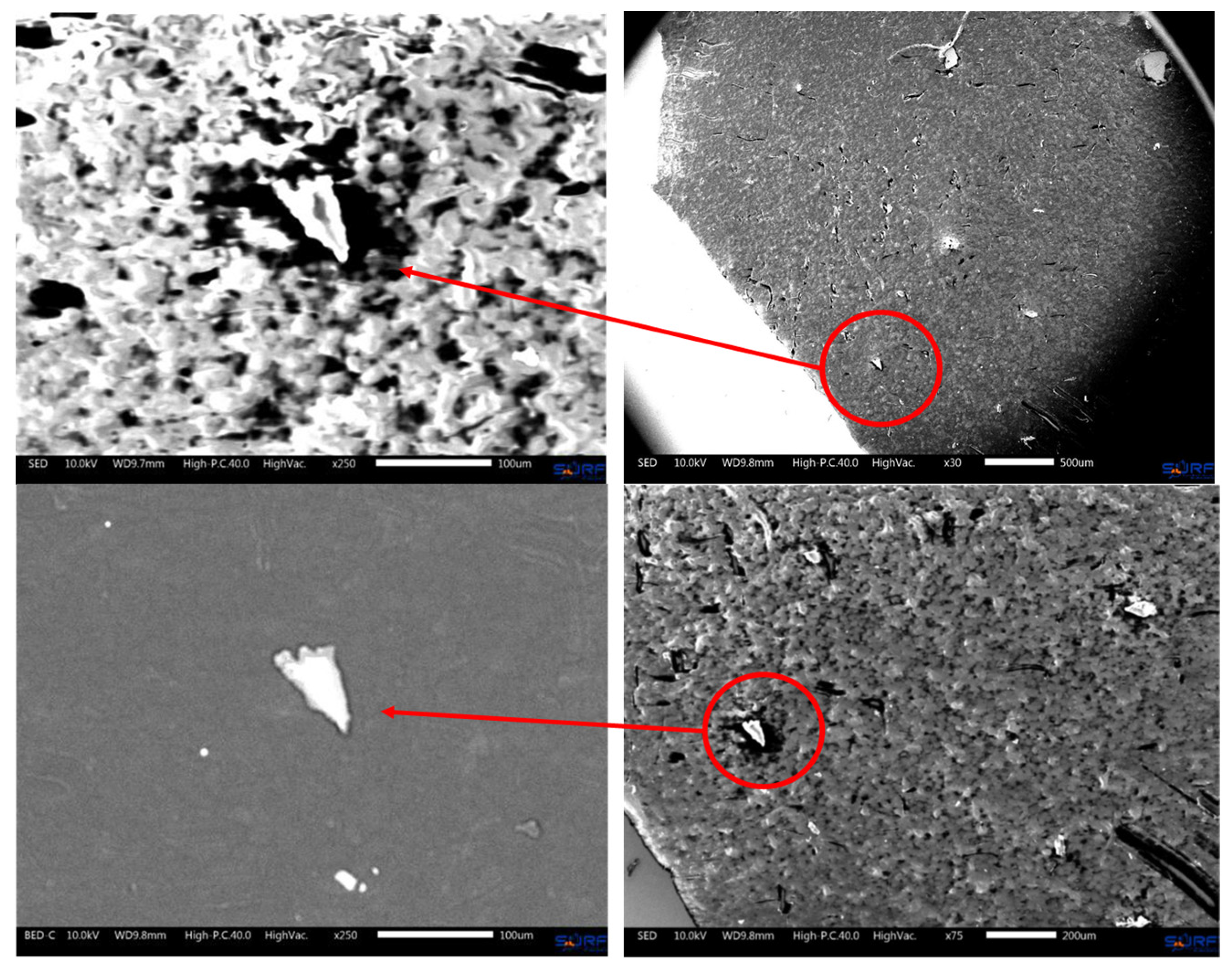
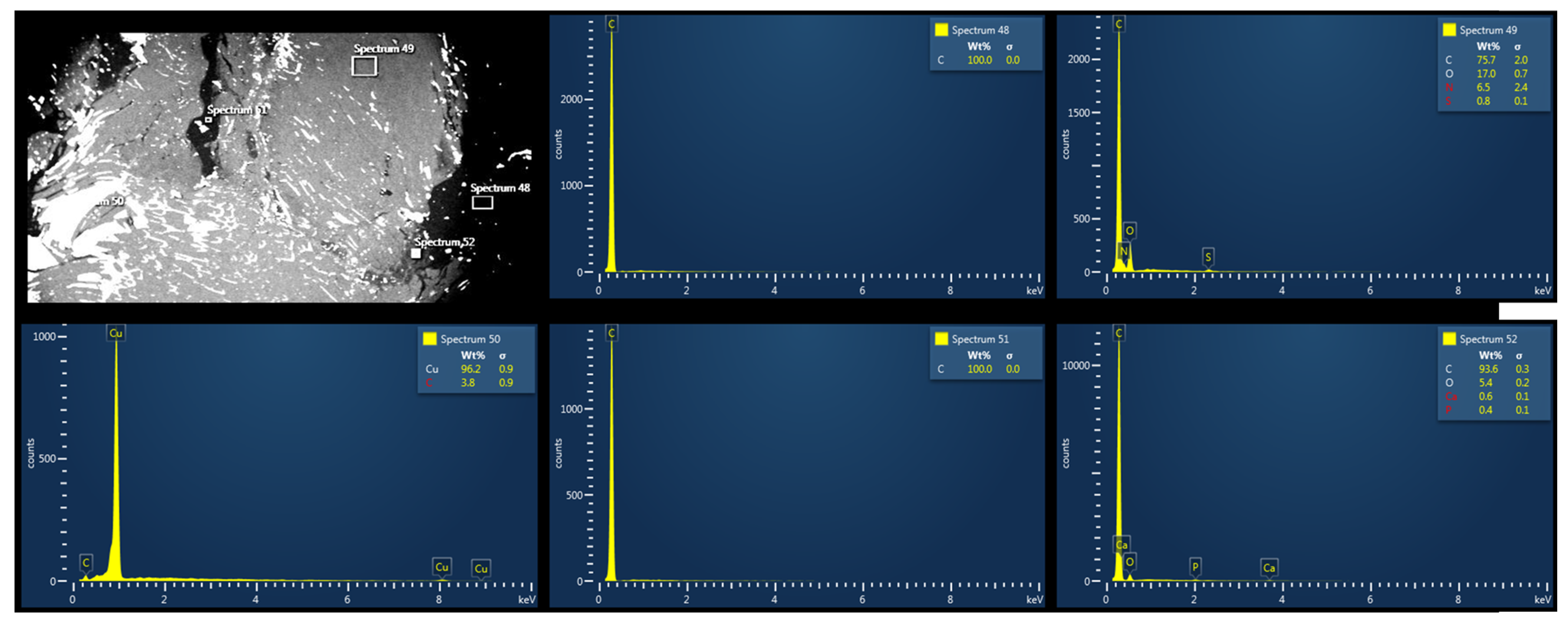
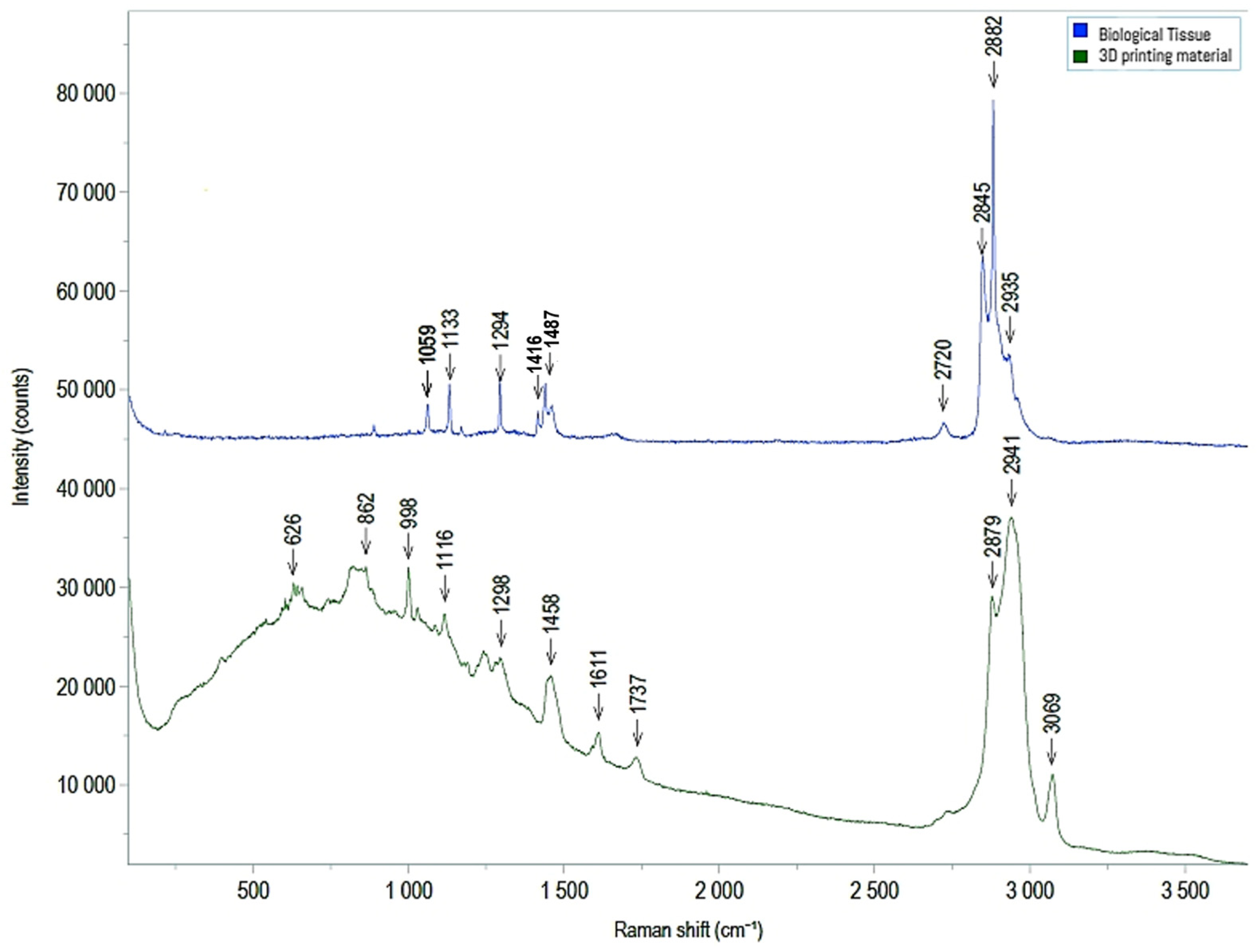
3.3. Electron Microscopy and Raman Spectroscopy
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Olivieri, L.J.; Su, L.; Hynes, C.F.; Krieger, A.; Alfares, F.A.; Ramakrishnan, K.; Zurakowski, D.; Marshall, M.B.; Kim, P.C.W.; Jonas, R.A.; et al. “Just-In-Time” Simulation Training Using 3-D Printed Cardiac Models after Congenital Cardiac Surgery. World J. Pediatr. Congenit. Heart Surg. 2016, 7, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Giannopoulos, A.A.; Steigner, M.L.; George, E.; Barile, M.; Hunsaker, A.R.; Rybicki, F.J.; Mitsouras, D. Cardiothoracic Applications of 3-Dimensional Printing. J. Thorac. Imaging 2016, 31, 253–272. [Google Scholar] [CrossRef] [PubMed]
- Meier, L.M.; Meineri, M.; Qua Hiansen, J.; Horlick, E.M. Structural and Congenital Heart Disease Interventions: The Role of Three-Dimensional Printing. Neth. Heart J. 2017, 25, 65–75. [Google Scholar] [CrossRef]
- Candelari, M.; Cappello, I.A.; Pannone, L.; Monaco, C.; Talevi, G.; Bori, E.; Ramak, R.; La Meir, M.; Gharaviri, A.; Chierchia, G.B.; et al. A 3D-Printed Surgical Guide for Ischemic Scar Targeting and Ablation. Front. Cardiovasc. Med. 2022, 9, 1029816. [Google Scholar] [CrossRef] [PubMed]
- Talevi, G.; Pannone, L.; Monaco, C.; Bori, E.; Cappello, I.A.; Candelari, M.; Ramak, R.; La Meir, M.; Gharaviri, A.; Chierchia, G.B.; et al. Development of a 3D Printed Surgical Guide for Brugada Syndrome Substrate Ablation. Front. Cardiovasc. Med. 2022, 9, 1029685. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A. Additive Manufacturing Applications in Medical Cases: A Literature Based Review. Alex. J. Med. 2018, 54, 411–422. [Google Scholar] [CrossRef]
- ISO 10993-1:2018; Biological Evaluation of Medical Devices—Part 1: Evaluation and Testing within a Risk Management Process. International Organization for Standardization: Geneva, Switzerland, 2018.
- Biocompatibility Requirements Printing Biocompatible Parts on PolyJetTM 3D Printers with MED625FLX TM, CL: Flexible Clear Biocompatible Material; 2022. Available online: https://support.stratasys.com/download/FD81A519-5973-4309-BE97-0B01F3CCD0A5 (accessed on 11 April 2024).
- Vogels, R.R.M.; Lambertz, A.; Schuster, P.; Jockenhoevel, S.; Bouvy, N.D.; Disselhorst-Klug, C.; Neumann, U.P.; Klinge, U.; Klink, C.D. Biocompatibility and Biomechanical Analysis of Elastic TPU Threads as New Suture Material. J. Biomed. Mater. Res. B Appl. Biomater. 2015, 105, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Guttridge, C.; Shannon, A.; O’Sullivan, A.; O’Sullivan, K.J.; O’Sullivan, L.W. Biocompatible 3D Printing Resins for Medical Applications: A Review of Marketed Intended Use, Biocompatibility Certification, and Post-Processing Guidance. Ann. 3D Print. Med. 2021, 5, 100044. [Google Scholar] [CrossRef]
- Cappello, I.A.; Candelari, M.; Pannone, L.; Monaco, C.; Bori, E.; Talevi, G.; Ramak, R.; La Meir, M.; Gharaviri, A.; Chierchia, G.B.; et al. 3D Printed Surgical Guide for Coronary Artery Bypass Graft: Workflow from Computed Tomography to Prototype. Bioengineering 2022, 9, 179. [Google Scholar] [CrossRef]
- Burkhardt, F.; Handermann, L.; Rothlauf, S.; Gintaute, A.; Vach, K.; Spies, B.C.; Lüchtenborg, J. Accuracy of Additively Manufactured and Steam Sterilized Surgical Guides by Means of Continuous Liquid Interface Production, Stereolithography, Digital Light Processing, and Fused Filament Fabrication. J. Mech. Behav. Biomed. Mater. 2024, 152, 106418. [Google Scholar] [CrossRef] [PubMed]
- Eveland, R.; Antloga, K.; Meyer, A.; Tuscano, L. Low Temperature Vaporized Hydrogen Peroxide Sterilization of 3D Printed Devices. 3D Print. Med. 2024, 10, 6. [Google Scholar] [CrossRef]
- Cappello, I.A.; Candelari, M.; Pannone, L.; Monaco, C.; Bori, E.; Talevi, G.; Ramak, R.; La Meir, M.; Gharaviri, A.; Chierchia, G.B.; et al. Temperature Analysis of 3D-Printed Biomaterials during Unipolar and Bipolar Radiofrequency Ablation Procedure. Front. Cardiovasc. Med. 2022, 9, 978333. [Google Scholar] [CrossRef]
- Candelari, M.; Cappello, I.A.; Pannone, L.; Monaco, C.; Bori, E.; Talevi, G.; Ramak, R.; La Meir, M.; Gharaviri, A.; Chierchia, G.B.; et al. 3D-Printed Biomaterial Testing in Response to Cryoablation: Implications for Surgical Ventricular Tachycardia Ablation. J. Clin. Med. 2023, 12, 1036. [Google Scholar] [CrossRef] [PubMed]
- Calzolari, V.; De Mattia, L.; Indiani, S.; Crosato, M.; Furlanetto, A.; Licciardello, C.; Squasi, P.A.M.; Olivari, Z. In Vitro Validation of the Lesion Size Index to Predict Lesion Width and Depth After Irrigated Radiofrequency Ablation in a Porcine Model. JACC Clin. Electrophysiol. 2017, 3, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- Kawel, N.; Turkbey, E.B.; Carr, J.J.; Eng, J.; Gomes, A.S.; Hundley, W.G.; Johnson, C.; Masri, S.C.; Prince, M.R.; Van Der Geest, R.J.; et al. Middle-Aged and Older Subjects with Steady-State Free Precession Cardiac Magnetic Resonance the Multi-Ethnic Study of Atherosclerosis. Circ. Cardiovasc. Imaging 2012, 5, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Nagy, B.; Farkas, A.; Borbás, E.; Vass, P.; Nagy, Z.K.; Marosi, G. Raman Spectroscopy for Process Analytical Technologies of Pharmaceutical Secondary Manufacturing. AAPS PharmSciTech 2018, 20, 1. [Google Scholar] [CrossRef] [PubMed]
- Butler, H.J.; Ashton, L.; Bird, B.; Cinque, G.; Curtis, K.; Dorney, J.; Esmonde-White, K.; Fullwood, N.J.; Gardner, B.; Martin-Hirsch, P.L.; et al. Using Raman Spectroscopy to Characterize Biological Materials. Nat. Protoc. 2016, 11, 664–687. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 3D Printing Material | Thickness (mm) | Geometry Damage Index |
|---|---|---|
| MED625FLX | 0.8 | 2 |
| 1 | 0 | |
| 2.5 | 0 | |
| 3 | 0 | |
| TPU95A | 0.8 | 2 |
| 1 | 0 | |
| 2.5 | 0 | |
| 3 | 1 |
| Thickness of 3DP Model (mm) | Cryo N. Applications Delivered | Uni-RF N. Applications Delivered | Bi-RF N. Applications Delivered | N. Applications/ Material | |||
|---|---|---|---|---|---|---|---|
| Ablation catheter | Ablation catheter | Electro-cautery | Ablation catheter | Electro-cautery | |||
| Control | N/A | 4 | 4 | 4 | 4 | 4 | 20 |
| MED625FLX | 1 | 4 | 4 | 4 | 4 | 4 | 20 |
| 2.5 | 4 | 4 | 4 | 4 | 4 | 20 | |
| TPU | 1 | 4 | 4 | 4 | 4 | 4 | 20 |
| 2.5 | 4 | 4 | 4 | 4 | 4 | 20 | |
| N. Applications/energy type 20 | 40 | 40 | 100 | ||||
| Mixed ANCOVA—Temperature | |||||
|---|---|---|---|---|---|
| Cases | Sum of Squares | DF | Mean Square | F Statistic | p-Value |
| Thickness | 15.969 | 1 | 15.969 | 0.366 | 0.545 |
| Material | 378.539 | 1 | 378.539 | 8.681 | 0.003 |
| Distance | 2.260 | 1 | 2.260 | 0.052 | 0.820 |
| Energy | 55,706.124 | 2 | 27,853.062 | 638.751 | <0.001 |
| Time | 75.776 | 3 | 25.259 | 0.579 | 0.629 |
| Thickness ✻ Material | 8.724 | 1 | 8.724 | 0.200 | 0.655 |
| Thickness ✻ Distance | 140.150 | 1 | 140.150 | 3.214 | 0.074 |
| Thickness ✻ Energy | 67.475 | 2 | 33.737 | 0.774 | 0.462 |
| Thickness ✻ Time | 9.467 | 3 | 3.156 | 0.072 | 0.975 |
| Material ✻ Distance | 238.805 | 1 | 238.805 | 5.476 | 0.020 |
| Material ✻ Energy | 77.657 | 2 | 38.828 | 0.890 | 0.411 |
| Material ✻ Time | 20.792 | 3 | 6.931 | 0.159 | 0.924 |
| Distance ✻ Energy | 22,681.436 | 2 | 11,340.718 | 260.075 | <0.001 |
| Distance ✻ Time | 14.797 | 3 | 4.932 | 0.113 | 0.952 |
| Energy ✻ Time | 522.313 | 6 | 87.052 | 1.996 | 0.065 |
| Thickness ✻ Material ✻ Distance | 0.665 | 1 | 0.665 | 0.015 | 0.902 |
| Thickness ✻ Material ✻ Energy | 140.044 | 2 | 70.022 | 1.606 | 0.202 |
| Thickness ✻ Material ✻ Time | 3.036 | 3 | 1.012 | 0.023 | 0.995 |
| Thickness ✻ Distance ✻ Energy | 125.124 | 2 | 62.562 | 1.435 | 0.240 |
| Thickness ✻ Distance ✻ Time | 0.709 | 3 | 0.236 | 0.005 | 0.999 |
| Thickness ✻ Energy ✻ Time | 37.848 | 6 | 6.308 | 0.145 | 0.990 |
| Material ✻ Distance ✻ Energy | 33.523 | 2 | 16.762 | 0.384 | 0.681 |
| Material ✻ Distance ✻ Time | 37.493 | 3 | 12.498 | 0.287 | 0.835 |
| Material ✻ Energy ✻ Time | 7.003 | 6 | 1.167 | 0.027 | 1.000 |
| Distance ✻ Energy ✻ Time | 425.703 | 6 | 70.950 | 1.627 | 0.139 |
| Thickness ✻ Material ✻ Distance ✻ Energy | 33.727 | 2 | 16.864 | 0.387 | 0.680 |
| Thickness ✻ Material ✻ Distance ✻ Time | 12.126 | 3 | 4.042 | 0.093 | 0.964 |
| Thickness ✻ Material ✻ Energy ✻ Time | 2.013 | 6 | 0.335 | 0.008 | 1.000 |
| Thickness ✻ Distance ✻ Energy ✻ Time | 1.027 | 6 | 0.171 | 0.004 | 1.000 |
| Material ✻ Distance ✻ Energy ✻ Time | 10.228 | 6 | 1.705 | 0.039 | 1.000 |
| Thickness ✻ Material ✻ Distance ✻ Energy ✻ Time | 8.531 | 6 | 1.422 | 0.033 | 1.000 |
| Residuals | 15,567.165 | 357 | 43.606 | ||
| Temperature * | z-test | Wi | Wj | p-value | ||
| Distance (mm) | 1–11 | 3.764 | 250.000 | 203.799 | <0.001 | |
| Energy type | Cryo–bi-RF | −12.020 | 78.378 | 259.172 | <0.001 | |
| Cryo–uni-RF | −17.711 | 78.378 | 345.217 | <0.001 | ||
| Bi-RF–uni-RF | −5.702 | 259.172 | 345.217 | <0.001 | ||
| Material | MED625FLX-TPU | −0.645 | 222.828 | 230.769 | 0.260 | |
| Thickness (mm) | 1–2.5 | 1.369 | 235.858 | 218.998 | 0.086 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monaco, C.; Kronenberger, R.; Talevi, G.; Pannone, L.; Cappello, I.A.; Candelari, M.; Ramak, R.; Della Rocca, D.G.; Bori, E.; Terryn, H.; et al. Advancing Surgical Arrhythmia Ablation: Novel Insights on 3D Printing Applications and Two Biocompatible Materials. Biomedicines 2024, 12, 869. https://doi.org/10.3390/biomedicines12040869
Monaco C, Kronenberger R, Talevi G, Pannone L, Cappello IA, Candelari M, Ramak R, Della Rocca DG, Bori E, Terryn H, et al. Advancing Surgical Arrhythmia Ablation: Novel Insights on 3D Printing Applications and Two Biocompatible Materials. Biomedicines. 2024; 12(4):869. https://doi.org/10.3390/biomedicines12040869
Chicago/Turabian StyleMonaco, Cinzia, Rani Kronenberger, Giacomo Talevi, Luigi Pannone, Ida Anna Cappello, Mara Candelari, Robbert Ramak, Domenico Giovanni Della Rocca, Edoardo Bori, Herman Terryn, and et al. 2024. "Advancing Surgical Arrhythmia Ablation: Novel Insights on 3D Printing Applications and Two Biocompatible Materials" Biomedicines 12, no. 4: 869. https://doi.org/10.3390/biomedicines12040869
APA StyleMonaco, C., Kronenberger, R., Talevi, G., Pannone, L., Cappello, I. A., Candelari, M., Ramak, R., Della Rocca, D. G., Bori, E., Terryn, H., Baert, K., Laha, P., Krasniqi, A., Gharaviri, A., Bala, G., Chierchia, G. B., La Meir, M., Innocenti, B., & de Asmundis, C. (2024). Advancing Surgical Arrhythmia Ablation: Novel Insights on 3D Printing Applications and Two Biocompatible Materials. Biomedicines, 12(4), 869. https://doi.org/10.3390/biomedicines12040869