

Friend or Foe? Exploring the Role of Cytomegalovirus (HCMV) Infection in Head and Neck Tumors

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zuhair, M.; Smit, G.S.A.; Wallis, G.; Jabbar, F.; Smith, C.; Devleesschauwer, B.; Griffiths, P. Estimation of the worldwide seroprevalence of cytomegalovirus: A systematic review and meta-analysis. Rev. Med. Virol. 2019, 29, e2034. [Google Scholar] [CrossRef] [PubMed]
- Stangherlin, L.M.; Castro, F.L.; Medeiros, R.S.; Guerra, J.M.; Kimura, L.M.; Shirata, N.K.; Nonogaki, S.; Dos Santos, C.J.; Carlan Silva, M.C. Human Cytomegalovirus DNA Quantification and Gene Expression in Gliomas of Different Grades. PLoS ONE 2016, 11, e0159604. [Google Scholar] [CrossRef] [PubMed]
- Geisler, J.; Touma, J.; Rahbar, A.; Söderberg-Nauclér, C.; Vetvik, K. A Review of the Potential Role of Human Cytomegalovirus (HCMV) Infections in Breast Cancer Carcinogenesis and Abnormal Immunity. Cancers 2019, 11, 1842. [Google Scholar] [CrossRef] [PubMed]
- Francis, S.S.; Wallace, A.D.; Wendt, G.A.; Li, L.; Liu, F.; Riley, L.W.; Kogan, S.; Walsh, K.M.; de Smith, A.J.; Dahl, G.V.; et al. In utero cytomegalovirus infection and development of childhood acute lymphoblastic leukemia. Blood 2017, 129, 1680–1684. [Google Scholar] [CrossRef] [PubMed]
- Wiemels, J.L.; Talbäck, M.; Francis, S.; Feychting, M. Early Infection with Cytomegalovirus and Risk of Childhood Hematologic Malignancies. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1024–1027. [Google Scholar] [CrossRef] [PubMed]
- Herbein, G. The Human Cytomegalovirus, from Oncomodulation to Oncogenesis. Viruses 2018, 10, 408. [Google Scholar] [CrossRef]
- Hochhalter, C.B.; Carr, C.; O’Neill, B.E.; Ware, M.L.; Strong, M.J. The association between human cytomegalovirus and glioblastomas: A review. Neuroimmunol. Neuroinflamm. 2017, 4, 96–108. [Google Scholar] [CrossRef]
- Kumar, A.; Coquard, L.; Pasquereau, S.; Russo, L.; Valmary-Degano, S.; Borg, C.; Pothier, P.; Herbein, G. Tumor control by human cytomegalovirus in a murine model of hepatocellular carcinoma. Mol. Ther. Oncolytics 2016, 3, 16012. [Google Scholar] [CrossRef] [PubMed]
- Jurak, I.; Brune, W. Induction of apoptosis limits cytomegalovirus cross-species infection. EMBO J. 2006, 25, 2634–2642. [Google Scholar] [CrossRef] [PubMed]
- Erkes, D.A.; Wilski, N.A.; Snyder, C.M. Intratumoral infection by CMV may change the tumor environment by directly interacting with tumor-associated macrophages to promote cancer immunity. Hum. Vaccin. Immunother. 2017, 13, 1778–1785. [Google Scholar] [CrossRef] [PubMed]
- Nagel, B.; Frankel, L.; Ardeljan, A.; Cardeiro, M.; Rashid, S.; Takabe, K.; Rashid, O.M. The Association of Human Cytomegalovirus Infection and Colorectal Cancer: A Clinical Analysis. World J. Oncol. 2023, 14, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Rashid, S.; Ardeljan, A.; Frankel, L.R.; Cardeiro, M.; Kim, E.; Nagel, B.M.; Takabe, K.; Rashid, O. Human Cytomegalovirus (CMV) Infection Associated with Decreased Risk of Bronchogenic Carcinoma: Understanding How a Previous CMV Infection Leads to an Enhanced Immune Response Against Malignancy. Cureus 2023, 15, e37265. [Google Scholar] [CrossRef] [PubMed]
- Janković, M.; Knežević, A.; Todorović, M.; Đunić, I.; Mihaljević, B.; Soldatović, I.; Protić, J.; Miković, N.; Stoiljković, V.; Jovanović, T. Cytomegalovirus infection may be oncoprotective against neoplasms of B-lymphocyte lineage: Single-institution experience and survey of global evidence. Virol. J. 2022, 19, 155. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, M.; Knezevic, T.; Tomic, A.; Milicevic, O.; Jovanovic, T.; Djunic, I.; Mihaljevic, B.; Knezevic, A.; Todorovic-Balint, M. Human Cytomegalovirus Oncoprotection across Diverse Populations, Tumor Histologies, and Age Groups: The Relevance for Prospective Vaccinal Therapy. Int. J. Mol. Sci. 2024, 25, 3741. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Classification of Tumours Online. Available online: https://tumourclassification.iarc.who.int/welcome/ (accessed on 2 November 2023).
- Global Cancer Observatory. Available online: https://gco.iarc.fr/ (accessed on 8 December 2020).
- Lachmann, R.; Loenenbach, A.; Waterboer, T.; Brenner, N.; Pawlita, M.; Michel, A.; Thamm, M.; Poethko-Muller, C.; Wichmann, O.; Wiese-Posselt, M. Cytomegalovirus (CMV) seroprevalence in the adult population of Germany. PLoS ONE 2018, 13, e0200267. [Google Scholar] [CrossRef] [PubMed]
- Cannon, M.J.; Schmid, D.S.; Hyde, T.B. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev. Med. Virol. 2010, 20, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Marshall, G.S.; Rabalais, G.P.; Stewart, J.A.; Dobbins, J.G. Cytomegalovirus seroprevalence in women bearing children in Jefferson County, Kentucky. Am. J. Med. Sci. 1993, 305, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Hecker, M.; Qiu, D.; Marquardt, K.; Bein, G.; Hackstein, H. Continuous cytomegalovirus seroconversion in a large group of healthy blood donors. Vox Sang. 2004, 86, 41–44. [Google Scholar] [CrossRef]
- Staras, S.A.S.; Dollard, S.C.; Radford, K.W.; Flanders, W.D.; Pass, R.F.; Cannon, M.J. Seroprevalence of cytomegalovirus infection in the United States, 1988–1994. Clin. Infect. Dis. 2006, 43, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Ahlfors, K. IgG antibodies to cytomegalovirus in a normal urban Swedish population. Scand. J. Infect. Dis. 1984, 16, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Human Development Index. Available online: https://hdr.undp.org/data-center/human-development-index#/indicies/HDI (accessed on 2 November 2023).
- Our World in Data. Age Structure. Available online: https://ourworldindata.org/age-structure#how-does-median-age-vary-across-the-world (accessed on 2 November 2023).
- World Population Review. Average Number of Sexual Partners by Country 2024. Available online: https://worldpopulationreview.com/country-rankings/average-number-of-sexual-partners-by-country (accessed on 2 November 2023).
- The Tobacco Atlas. Prevalence. 2023. Available online: https://tobaccoatlas.org/challenges/prevalence/ (accessed on 2 November 2023).
- UNICEF. Breastfeeding Practices Worldwide. Available online: https://data.unicef.org/resources/world-breastfeeding-week-2020/ (accessed on 2 November 2023).
- The World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 2 November 2023).
- Polz-Gruszka, D.; Stec, A.; Dworzański, J.; Polz-Dacewicz, M. EBV, HSV, CMV and HPV in laryngeal and oropharyngeal carcinoma in Polish patients. Anticancer Res. 2015, 35, 1657–1661. [Google Scholar] [PubMed]
- Strauss, M. Cytomegalovirus and the otolaryngologist. Laryngoscope 1981, 91, 1995–2006. [Google Scholar] [CrossRef] [PubMed]
- Schindele, A.; Holm, A.; Nylander, K.; Allard, A.; Olofsson, K. Mapping human papillomavirus, Epstein-Barr virus, cytomegalovirus, adenovirus, and p16 in laryngeal cancer. Discov. Oncol. 2022, 13, 18. [Google Scholar] [CrossRef] [PubMed]
- Munjal, T.; Vukkadala, N.; Hazard, F.K.; Meister, K.D. Next-Generation Sequencing as an Auxiliary Tool in Pediatric Laryngeal Lymphoma Diagnosis. Pediatrics 2015, 8, e21838. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.J.; Browning, D.; Schwartz, D.A.; Hudgins, P.A. Cytomegaloviral laryngitis and probable malignant lymphoma of the larynx in a patient with acquired immunodeficiency syndrome. Arch. Pathol. Lab. Med. 1992, 116, 539–541. [Google Scholar]
- Riederer, A.; Zietz, C.; Held, M. Das HIV-assoziierte Kaposi-Sarkom im Kopf-Hals-Bereich: Eine klinische, morphologische und therapeutische Ubersicht [HIV-associated Kaposi sarcoma in the head and neck area: A clinical, morphologic and therapeutic review]. Laryngorhinootologie 1993, 72, 478–484. (In German) [Google Scholar] [CrossRef]
- Ahmed, H.G.; Suliman, R.S.A.; Ashankyty, I.M.; Albieh, Z.A.; Warille, A.A. Role of human Cytomegalovirus in the etiology of nasopharyngeal carcinoma. J. Cancer Res. Ther. 2018, 14, 583–586. [Google Scholar] [CrossRef] [PubMed]
- Chan, B.W.; Woo, J.K.; Liew, C.T. Cytomegalovirus infection of the nasopharynx. J. Clin. Pathol. 2002, 55, 970–972. [Google Scholar] [CrossRef] [PubMed]
- Desgranges, C.; Seigneurin, J.M.; Baccard, M.; Nejmi, S. Cytomegalovirus isolations from cell cultures derived from Epstein-Barr virus-associated nasopharyngeal carcinoma. J. Natl. Cancer Inst. 1983, 71, 39–43. [Google Scholar]
- Lin, C.T.; Dee, A.N.; Chen, W.; Chan, W.Y. Association of Epstein-Barr virus, human papilloma virus, and cytomegalovirus with nine nasopharyngeal carcinoma cell lines. Lab. Investig. 1994, 71, 731–736. [Google Scholar] [PubMed]
- Kalavari, F.; Tanzifi, P.; Yousefi, T.; Lotfi, M.; Nazar, E. Investigation of Parvovirus B19, Cytomegalovirus, Herpes Simplex Virus Types 1 and 2, Human Papillomavirus Types 16 and 18 in Papillary Thyroid Carcinoma. Iran. J. Pathol. 2023, 18, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.S.; Lee, J.J.; Cheng, S.P. No evidence of association between human cytomegalovirus infection and papillary thyroid cancer. World J. Surg. Oncol. 2014, 12, 41. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; el-Sahrigy, D.; Elhosseiny, A.; Melamed, M.R. Simultaneous cytomegalovirus infection and Kaposi’s sarcoma of the thyroid diagnosed by fine needle aspiration in an AIDS patient. A case report and first cytologic description of the two entities occurring together. Acta Cytol. 2003, 47, 645–648. [Google Scholar] [CrossRef] [PubMed]
- Frank, T.S.; LiVolsi, V.A.; Connor, A.M. Cytomegalovirus infection of the thyroid in immunocompromised adults. Yale J. Biol. Med. 1987, 60, 1–8. [Google Scholar] [PubMed]
- Carroll, V.A.; Lundgren, A.; Wei, H.; Sainz, S.; Tung, K.S.; Brown, M.G. Natural killer cells regulate murine cytomegalovirus-induced sialadenitis and salivary gland disease. J. Virol. 2012, 86, 2132–2142. [Google Scholar] [CrossRef] [PubMed]
- Melnick, M.; Deluca, K.A.; Sedghizadeh, P.P.; Jaskoll, T. Cytomegalovirus-induced salivary gland pathology: AREG, FGF8, TNF-α, and IL-6 signal dysregulation and neoplasia. Exp. Mol. Pathol. 2013, 94, 386–397. [Google Scholar] [CrossRef] [PubMed]
- Melnick, M.; Sedghizadeh, P.P.; Allen, C.M.; Jaskoll, T. Human cytomegalovirus and mucoepidermoid carcinoma of salivary glands: Cell-specific localization of active viral and oncogenic signaling proteins is confirmatory of a causal relationship. Exp. Mol. Pathol. 2012, 92, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Atula, T.; Grénman, R.; Klemi, P.; Syrjänen, S. Human papillomavirus, Epstein-Barr virus, human herpesvirus 8 and human cytomegalovirus involvement in salivary gland tumours. Oral Oncol. 1998, 34, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Kärjä, V.; Syrjänen, K.; Syrjänen, S. No Epstein Barr and cytomegalovirus DNA found in salivary gland tumours. ORL J. Otorhinolaryngol. Relat. Spec. 1997, 59, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Radunovic, M.; Tomanovic, N.; Novakovic, I.; Boricic, I.; Milenkovic, S.; Dimitrijevic, M.; Radojevic-Skodric, S.; Bogdanovic, L.; Basta-Jovanovic, G. Cytomegalovirus induces Interleukin-6 mediated inflammatory response in salivary gland cancer. J. BUON 2016, 21, 1530–1536. [Google Scholar] [PubMed]
- Yang, G.R.; Huang, G.S.; Wang, J.H.; Wang, E.H.; Wang, Z.; Song, J.Y. Human cytomegalovirus inhibits proliferation of duct epithelial cells of human salivary gland. Zhonghua Kou Qiang Yi Xue Za Zhi 2004, 39, 298–301. (In Chinese) [Google Scholar] [PubMed]
- Saravani, S.; Kadeh, H.; Miri-Moghaddam, E.; Zekri, A.; Sanadgol, N.; Gholami, A. Human Cytomegalovirus in Oral Squamous Cell Carcinoma in Southeast of Iran. Jundishapur J. Microbiol. 2015, 8, e21838. [Google Scholar] [CrossRef] [PubMed]
- Naqvi, S.U.; Khan, S.; Ahmed, A.; Lail, A.; Gul, S.; Ahmed, S. Prevalence of EBV, CMV, and HPV in oral squamous cell carcinoma patients in the Pakistani population. J. Med. Virol. 2020, 92, 3880–3883. [Google Scholar] [CrossRef] [PubMed]
- Kelly, E.; Russell, S.J. History of oncolytic viruses: Genesis to genetic engineering. Mol. Ther. 2007, 15, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.J.; Peng, K.W.; Bell, J.C. Oncolytic virotherapy. Nat. Biotechnol. 2012, 30, 658–670. [Google Scholar] [CrossRef] [PubMed]
- Cao, G.D.; He, X.B.; Sun, Q.; Chen, S.; Wan, K.; Xu, X.; Feng, X.; Li, P.P.; Chen, B.; Xiong, M.M. The Oncolytic Virus in Cancer Diagnosis and Treatment. Front. Oncol. 2020, 10, 1786. [Google Scholar] [CrossRef] [PubMed]
- Laane, C.J.; Murr, A.H.; Mhatre, A.N.; Jones, K.D.; Lalwan, A.K. Role of Epstein-Barr virus and cytomegalovirus in the etiology of benign parotid tumors. Head Neck 2002, 24, 443–450. [Google Scholar] [CrossRef]
- Ingerslev, K.; Høgdall, E.; Skovrider-Ruminski, W.; Schnack, T.H.; Lidang, M.; Høgdall, C.; Blaakaer, J. The prevalence of EBV and CMV DNA in epithelial ovarian cancer. Infect. Agents Cancer 2019, 14, 7. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, J.F.; van Hecke, W.; Jansen, M.K.; Spliet, W.G.; Broekhuizen, R.; Bovenschen, N. No evidence for human cytomegalovirus infection in pediatric medulloblastomas. Neuro Oncol. 2016, 18, 1461–1462. [Google Scholar] [CrossRef] [PubMed]
- Geris, J.M.; Spector, L.G.; Pfeiffer, R.M.; Limaye, A.P.; Yu, K.J.; Engels, E.A. Cancer risk associated with cytomegalovirus infection among solid organ transplant recipients in the United States. Cancer 2022, 128, 3985–3994. [Google Scholar] [CrossRef] [PubMed]
- Erlach, K.C.; Podlech, J.; Rojan, A.; Reddehase, M.J. Tumor control in a model of bone marrow transplantation and acute liver-infiltrating B-cell lymphoma: An unpredicted novel function of cytomegalovirus. J. Virol. 2002, 76, 2857–2870. [Google Scholar] [CrossRef] [PubMed]
- Bigley, A.B.; Baker, F.L.; Simpson, R.J. Cytomegalovirus: An unlikely ally in the fight against blood cancers? Clin. Exp. Immunol. 2018, 193, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Koldehoff, M.; Ross, S.R.; Dührsen, U.; Beelen, D.W.; Elmaagacli, A.H. Early CMV-replication after allogeneic stem cell transplantation is associated with a reduced relapse risk in lymphoma. Leuk. Lymphoma 2017, 58, 822–833. [Google Scholar] [CrossRef] [PubMed]
- Elmaagacli, A.H.; Steckel, N.K.; Koldehoff, M.; Hegerfeldt, Y.; Trenschel, R.; Ditschkowski, M.; Christoph, S.; Gromke, T.; Kordelas, L.; Ottinger, H.D.; et al. Early human cytomegalovirus replication after transplantation is associated with a decreased relapse risk: Evidence for a putative virus-versus-leukemia effect in acute myeloid leukemia patients. Blood 2011, 118, 1402–1412. [Google Scholar] [CrossRef] [PubMed]
- Green, M.L.; Leisenring, W.M.; Xie, H.; Walter, R.B.; Mielcarek, M.; Sandmaier, B.M.; Riddell, S.R.; Boeckh, M. CMV reactivation after allogeneic HCT and relapse risk: Evidence for early protection in acute myeloid leukemia. Blood 2013, 122, 1316–1324. [Google Scholar] [CrossRef] [PubMed]
- Litjens, N.H.R.; van der Wagen, L.; Kuball, J.; Kwekkeboom, J. Potential Beneficial Effects of Cytomegalovirus Infection after Transplantation. Front. Immunol. 2018, 9, 389. [Google Scholar] [CrossRef]
- Inagaki, J.; Noguchi, M.; Kurauchi, K.; Tanioka, S.; Fukano, R.; Okamura, J. Effect of Cytomegalovirus Reactivation on Relapse after Allogeneic Hematopoietic Stem Cell Transplantation in Pediatric Acute Leukemia. Biol. Blood Marrow Transplant. 2016, 22, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Peric, Z.; Wilson, J.; Durakovic, N.; Ostojic, A.; Desnica, L.; Vranjes, V.R.; Marekovic, I.; Serventi-Seiwerth, R.; Vrhovac, R. Early human cytomegalovirus reactivation is associated with lower incidence of relapse of myeloproliferative disorders after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2018, 53, 1450–1456. [Google Scholar] [CrossRef]
- Mattila, P.S.; Aalto, S.M.; Heikkilä, L.; Mattila, S.; Nieminen, M.; Auvinen, E.; Hedman, K.; Tarkkanen, J. Malignancies after heart transplantation: Presence of Epstein-Barr virus and cytomegalovirus. Clin. Transplant. 2001, 15, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.Y.; Koh, L.W.; Tsai, J.H.; Tsai, C.H.; Wong, E.F.; Lin, S.J.; Yang, C.C. Involvement of viral and chemical factors with oral cancer in Taiwan. Jpn. J. Clin. Oncol. 2004, 34, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Jayaraj, G.; Sherlin, H.J.; Ramani, P.; Premkumar, P.; Anuja, N. Cytomegalovirus and Mucoepidermoid carcinoma: A possible causal relationship? A pilot study. J. Oral Maxillofac. Pathol. 2015, 19, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.A.; Gheit, T.; Stellin, M.; Lupato, V.; Spinato, G.; Fuson, R.; Menegaldo, A.; Mckay-Chopin, S.; Dal Cin, E.; Tirelli, G.; et al. Oncogenic DNA viruses found in salivary gland tumors. Oral Oncol. 2017, 75, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.F.M.; Campos, A.H.; Marcello, M.A.; Bufalo, N.E.; Rossi, C.L.; Amaral, L.H.P.; Marques, A.B.; Cunha, L.L.; Alvarenga, C.A.; Tincani, P.C.; et al. Investigation on the association between thyroid tumorigeneses and herpesviruses. J. Endocrinol. Investig. 2017, 40, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Saeed, N.A.A.A.H.; Wahab, W.A. Thyroid Carcinoma Patients Correlated With Cytomegalovirus by using Insitu Hybridization. Indian J. Forensic Med. Toxicol. 2021, 15, 2726–2732. [Google Scholar] [CrossRef]
- Geder, L.; Sanford, E.J.; Rohner, T.J.; Rapp, F. Cytomegalovirus and cancer of the prostate: In vitro transformation of human cells. Cancer Treat. Rep. 1977, 61, 139–146. [Google Scholar] [PubMed]
- Herbein, G. Tumors and Cytomegalovirus: An Intimate Interplay. Viruses 2022, 14, 812. [Google Scholar] [CrossRef] [PubMed]
- Nauclér, C.S.; Geisler, J.; Vetvik, K. The emerging role of human cytomegalovirus infection in human carcinogenesis: A review of current evidence and potential therapeutic implications. Oncotarget 2019, 10, 4333–4347. [Google Scholar] [CrossRef] [PubMed]
- Cobbs, C.S. Cytomegalovirus and brain tumor: Epidemiology, biology and therapeutic aspects. Curr. Opin. Oncol. 2013, 25, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Barami, K. Oncomodulatory mechanisms of human cytomegalovirus in gliomas. J. Clin. Neurosci. 2010, 17, 819–823. [Google Scholar] [CrossRef]
- Pandey, J.P. Immunoglobulin GM Genes, Cytomegalovirus Immunoevasion, and the Risk of Glioma, Neuroblastoma, and Breast Cancer. Front. Oncol. 2014, 4, 236. [Google Scholar] [CrossRef] [PubMed]
- Nehme, Z.; Pasquereau, S.; Haidar Ahmad, S.; El Baba, R.; Herbein, G. Polyploid giant cancer cells, EZH2 and Myc upregulation in mammary epithelial cells infected with high-risk human cytomegalovirus. eBioMedicine 2022, 80, 104056. [Google Scholar] [CrossRef] [PubMed]
- Wolmer-Solberg, N.; Baryawno, N.; Rahbar, A.; Fuchs, D.; Odeberg, J.; Taher, C.; Wilhelmi, V.; Milosevic, J.; Mohammad, A.A.; Martinsson, T.; et al. Frequent detection of human cytomegalovirus in neuroblastoma: A novel therapeutic target? Int. J. Cancer 2013, 133, 2351–2361. [Google Scholar] [CrossRef] [PubMed]
- Herbein, G.; Kumar, A. The oncogenic potential of human cytomegalovirus and breast cancer. Front. Oncol. 2014, 4, 230. [Google Scholar] [CrossRef] [PubMed]
- Taher, C.; de Boniface, J.; Mohammad, A.A.; Religa, P.; Hartman, J.; Yaiw, K.C.; Frisell, J.; Rahbar, A.; Söderberg-Naucler, C. High prevalence of human cytomegalovirus proteins and nucleic acids in primary breast cancer and metastatic sentinel lymph nodes. PLoS ONE 2013, 8, e56795. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Guo, G.; Xu, J.; Sun, X.; Chen, W.; Jin, J.; Hu, C.; Zhang, P.; Shen, X.; Xue, X. Human cytomegalovirus detection in gastric cancer and its possible association with lymphatic metastasis. Diagn. Microbiol. Infect. Dis. 2017, 88, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Nelson, H.H.; Contestabile, E.; Hunter-Schlichting, D.; Koestler, D.; Pawlita, M.; Waterboer, T.; Christensen, B.C.; Petersen, C.L.; Miller, J.S.; Kelsey, K.T. Human cytomegalovirus alters immune cell profile with potential implications for patient survival in head and neck cancer. Carcinogenesis 2022, 43, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Soroceanu, L.; Cobbs, C.S. Is HCMV a tumor promoter? Virus Res. 2011, 157, 193–203. [Google Scholar] [CrossRef]
- Michaelis, M.; Doerr, H.W.; Cinatl, J. The story of human cytomegalovirus and cancer: Increasing evidence and open questions. Neoplasia 2009, 11, 1–9. [Google Scholar] [CrossRef]
- Costa, H.; Xu, X.; Overbeek, G.; Vasaikar, S.; Patro, C.P.; Kostopoulou, O.N.; Jung, M.; Shafi, G.; Ananthaseshan, S.; Tsipras, G.; et al. Human cytomegalovirus may promote tumor progression by upregulating arginase-2. Oncotarget 2016, 7, 47221–47231. [Google Scholar] [CrossRef] [PubMed]
- Cobbs, C.S.; Harkins, L.; Samanta, M.; Gillespie, G.Y.; Bharara, S.; King, P.H.; Nabors, L.B.; Cobbs, C.G.; Britt, W.J. Human cytomegalovirus infection and expression in human malignant glioma. Cancer Res. 2002, 62, 3347–3350. [Google Scholar] [PubMed]
- Joseph, G.P.; McDermott, R.; Baryshnikova, M.A.; Cobbs, C.S.; Ulasov, I.V. Cytomegalovirus as an oncomodulatory agent in the progression of glioma. Cancer Lett. 2017, 384, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Farias, K.P.R.A.; Moreli, M.L.; Floriano, V.G.; da Costa, V.G. Evidence based on a meta-analysis of human cytomegalovirus infection in glioma. Arch. Virol. 2019, 164, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, B.; Renzette, N.; Kowalik, T.F. Genetic analysis of cytomegalovirus in malignant gliomas. J. Virol. 2012, 86, 6815–6824. [Google Scholar] [CrossRef] [PubMed]
- Maleki, F.; Sadigh, Z.A.; Sadeghi, F.; Muhammadnejad, A.; Farahmand, M.; Parvin, M.; Shirkoohi, R. Human cytomegalovirus infection in Iranian glioma patients correlates with aging and tumor aggressiveness. J. Med. Virol. 2020, 92, 1266–1276. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Liu, D.; Fang, S.; Ma, W.; Wang, Y. Cytomegalovirus and Glioblastoma: A Review of the Biological Associations and Therapeutic Strategies. J. Clin. Med. 2022, 11, 5221. [Google Scholar] [CrossRef] [PubMed]
- Libard, S.; Popova, S.N.; Amini, R.-M.; Kärjä, V.; Pietiläinen, T.; Hämäläinen, K.M.; Sundström, C.; Hesselager, G.; Bergqvist, M.; Ekman, S.; et al. Human Cytomegalovirus Tegument Protein pp65 Is Detected in All Intra- and Extra-Axial Brain Tumours Independent of the Tumour Type or Grade. PLoS ONE 2014, 9, e108861. [Google Scholar]
- Habibi, Z.; Hajizadeh, M.; Nozarian, Z.; Safavi, M.; Monajemzadeh, M.; Meybodi, K.T.; Nejat, F.; Vasei, M. Cytomegalovirus DNA in non-glioblastoma multiforme brain tumors of infants. Childs Nerv. Syst. 2021, 37, 1581–1586. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, P.; Clark, P.A.; Kuo, J.S.; Salamat, M.S.; Kalejta, R.F. Significant association of multiple human cytomegalovirus genomic Loci with glioblastoma multiforme samples. J. Virol. 2012, 86, 854–864. [Google Scholar] [CrossRef] [PubMed]
- Michaelis, M.; Doerr, H.W.; Cinatl, J., Jr. Oncomodulation by human cytomegalovirus: Evidence becomes stronger. Med. Microbiol. Immunol. 2009, 198, 79–81. [Google Scholar] [CrossRef] [PubMed]
- Herbein, G. High-Risk Oncogenic Human Cytomegalovirus. Viruses 2022, 14, 2462. [Google Scholar] [CrossRef] [PubMed]
- Cinatl, J., Jr.; Vogel, J.U.; Kotchetkov, R.; Wilhelm Doerr, H. Oncomodulatory signals by regulatory proteins encoded by human cytomegalovirus: A novel role for viral infection in tumor progression. FEMS Microbiol. Rev. 2004, 28, 59–77. [Google Scholar] [CrossRef]
- Goerig, N.L.; Frey, B.; Korn, K.; Fleckenstein, B.; Überla, K.; Schmidt, M.A.; Dörfler, A.; Engelhorn, T.; Eyüpoglu, I.; Rühle, P.F.; et al. Frequent occurrence of therapeutically reversible CMV-associated encephalopathy during radiotherapy of the brain. Neuro Oncol. 2016, 18, 1664–1672. [Google Scholar] [CrossRef] [PubMed]
- Cobbs, C.S. Cytomegalovirus is a tumor-associated virus: Armed and dangerous. Curr. Opin. Virol. 2019, 39, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Roche, J. The Epithelial-to-Mesenchymal Transition in Cancer. Cancers 2018, 10, 52, Erratum in Cancers 2018, 10, 79. [Google Scholar] [CrossRef] [PubMed]
- Marcucci, F.; Stassi, G.; De Maria, R. Epithelial-mesenchymal transition: A new target in anticancer drug discovery. Nat. Rev. Drug Discov. 2016, 15, 311–325. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Belcher, J.D.; Marker, P.H.; Wilcken, D.E.; Vercellotti, G.M.; Wang, X.L. Cytomegalovirus inhibits p53 nuclear localization signal function. J. Mol. Med. 2001, 78, 642–647. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Keywords | Filter | Result No. | Relevant Results [Reference No.] | Period (Years) |
|---|---|---|---|---|
| CMV, laryng* | Title | 2 | 1 [29] | 2005–2024 |
| cytomegalov*, laryng* | Title | 168 | 5 [29,30,31,32,33] | 1960–2024 |
| HHV5, laryng* | Title | 0 | 0 | N/A |
| HHV-5, laryng* | Title | 0 | 0 | N/A |
| CMV, laryn* | Title | 2 | 1 [29] | 2005–2024 |
| Laryn*, cytomegalov* | Title | 13 | 2 [31,33] | 1981–2024 |
| Laryn*, HHV5 | Title | 0 | 0 | N/A |
| Laryn*, HHV-5 | Title | 0 | 0 | N/A |
| Hypophary*, CMV | Title | 6 | 1 [34] | 1993–2024 |
| Hypophary*, cytomegalov* | Title | 8 | 0 | 1990–2024 |
| Hypophary*, HHV5 | Title | 0 | 0 | N/A |
| Hypophary*, HHV-5 | Title | 0 | 0 | 1990–2024 |
| Nasopharyn*, CMV | Title | 2 | 0 | 1999–2024 |
| Nasopharyn*, cytomegalov* | Title | 5 | 4 [35,36,37,38] | 1979–2024 |
| Nasopharyn*, HHV-5 | Title | 0 | 0 | N/A |
| Nasopharyn*, HHV5 | Title | 0 | 0 | N/A |
| Thyroi*, CMV | Title | 3 | 0 | 2005–2024 |
| Thyroi*, cytomegalov* | Title | 13 | 4 [39,40,41,42] | 1976–2024 |
| Thyroi*, HHV5 | Title | 0 | 0 | N/A |
| Thyroi*, HHV-5 | Title | 0 | 0 | N/A |
| CMV, saliva* | Title | 25 | 0 | 1994–2004 |
| Cytomegalov*, saliva* | Title | 131 | 8 [43,44,45,46,47,48,49] | 1963–2024 |
| HHV5, saliva* | Title | 0 | 0 | N/A |
| HHV-5, saliva* | Title | 0 | 0 | N/A |
| CMV, lip | Title | 0 | 0 | N/A |
| Cytomegalov*, lip | Title | 1 | 0 | 2017 |
| HHV5, lip | Title | 0 | 0 | N/A |
| HHV-5, lip | Title | 0 | 0 | N/A |
| Cytomegalov*, oral* | Title | 48 | 1 [50] | 2014–2024 |
| CMV, oral* | Title | 5 | 1 [51] | 2014–2024 |
| HHV5, oral* | Title | 0 | 0 | N/A |
| HHV-5, oral* | Title | 0 | 0 | N/A |
| Tumor/Localization | Correlation Analysis | Univariate Linear Regression Analysis | Multivariate Linear Regression Analysis a | ||||
|---|---|---|---|---|---|---|---|
| Spearman’s ρ | Stand. Coeff. β | 95% CI | p-Value | Stand. Coeff. β | 95% CI | p-Value * | |
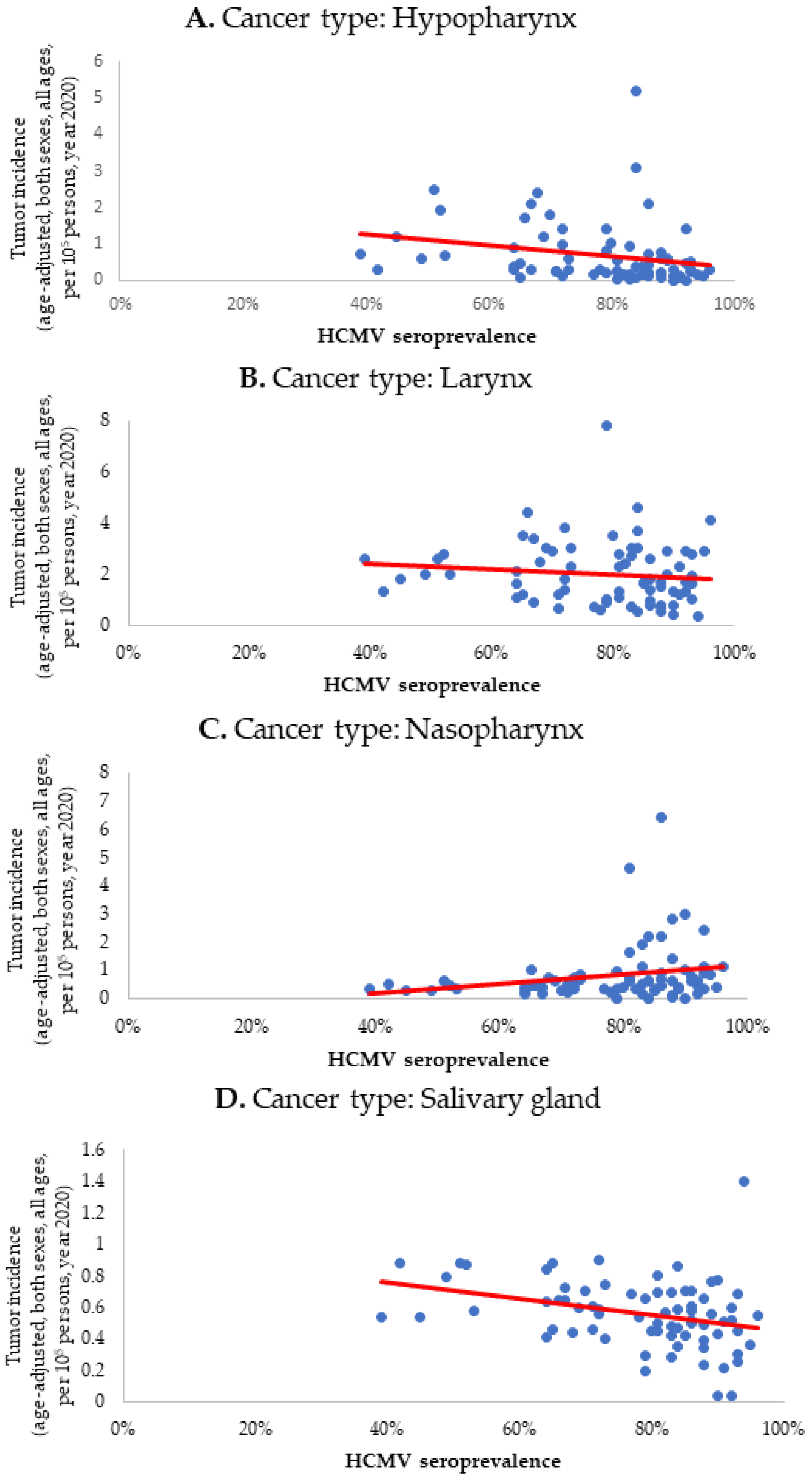
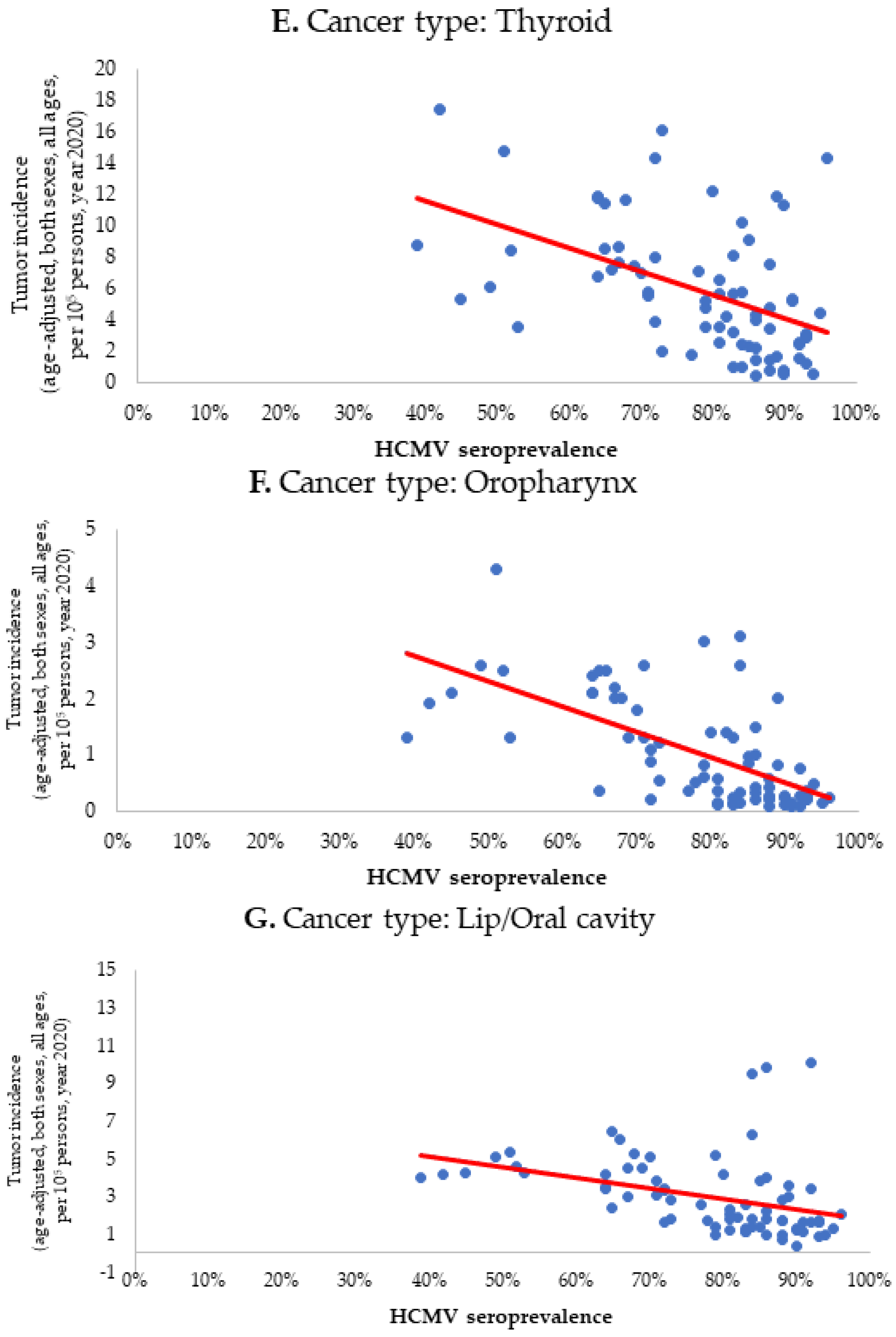
| Oropharynx | −0.651 * | −0.635 | −5.817–−3.217 | <0.001 * | −0.533 | −5.473–−2.137 | <0.001 * |
| Lip/Oral cavity | −0.551 * | −0.367 | −8.984–−2.243 | 0.001 * | −0.368 | −10.009–−1.273 | 0.012 * |
| Thyroid | −0.532 * | −0.485 | −21.293–−8.557 | <0.001 * | −0.138 | −11.466–2.901 | 0.238 |
| Hypopharynx | −0.377 * | −0.236 | −2.963–−0.039 | 0.044 * | −0.261 | −3.566–0.232 | 0.084 |
| Salivary glands | −0.350 * | −0.320 | −0.874–−0.154 | 0.006 * | −0.440 | −1.165–−0.248 | 0.003 * |
| Nasopharynx | 0.266 * | 0.227 | −0.023–3.451 | 0.053 | 0.338 | 0.337– 4.804 | 0.025 * |
| Larynx | −0.165 | −0.117 | −3.241–1.089 | 0.325 | 0.016 | 0.337– 4.804 | 0.913 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trivic, A.; Milovanovic, J.; Kablar, D.; Tomic, A.; Folic, M.; Jotic, A.; Tomanovic, N.; Tomic, A.M.; Djoric, I.; Jankovic, M. Friend or Foe? Exploring the Role of Cytomegalovirus (HCMV) Infection in Head and Neck Tumors. Biomedicines 2024, 12, 872. https://doi.org/10.3390/biomedicines12040872
Trivic A, Milovanovic J, Kablar D, Tomic A, Folic M, Jotic A, Tomanovic N, Tomic AM, Djoric I, Jankovic M. Friend or Foe? Exploring the Role of Cytomegalovirus (HCMV) Infection in Head and Neck Tumors. Biomedicines. 2024; 12(4):872. https://doi.org/10.3390/biomedicines12040872
Chicago/Turabian StyleTrivic, Aleksandar, Jovica Milovanovic, Djurdjina Kablar, Ana Tomic, Miljan Folic, Ana Jotic, Nada Tomanovic, Ana Marija Tomic, Igor Djoric, and Marko Jankovic. 2024. "Friend or Foe? Exploring the Role of Cytomegalovirus (HCMV) Infection in Head and Neck Tumors" Biomedicines 12, no. 4: 872. https://doi.org/10.3390/biomedicines12040872
APA StyleTrivic, A., Milovanovic, J., Kablar, D., Tomic, A., Folic, M., Jotic, A., Tomanovic, N., Tomic, A. M., Djoric, I., & Jankovic, M. (2024). Friend or Foe? Exploring the Role of Cytomegalovirus (HCMV) Infection in Head and Neck Tumors. Biomedicines, 12(4), 872. https://doi.org/10.3390/biomedicines12040872