Abstract
Diabetic neuropathy (DN) remains a major clinical burden, characterized by progressive sensory dysfunction, pain, and impaired quality of life. Despite the available symptomatic treatments, there is a pressing need for disease-modifying therapies. In recent years, preclinical research has highlighted the potential of repurposed pharmacological agents, originally developed for other indications, to target key mechanisms of DN. This narrative review examines the main pathophysiological pathways involved in DN, including metabolic imbalance, oxidative stress, neuroinflammation, ion channel dysfunction, and mitochondrial impairment. A wide array of repurposed drugs—including antidiabetics (metformin, empagliflozin, gliclazide, semaglutide, and pioglitazone), antihypertensives (amlodipine, telmisartan, aliskiren, and rilmenidine), lipid-lowering agents (atorvastatin and alirocumab), anticonvulsants (topiramate and retigabine), antioxidant and neuroprotective agents (melatonin), and muscarinic receptor antagonists (pirenzepine, oxybutynin, and atropine)—have shown promising results in rodent models, reducing neuropathic pain behaviors and modulating underlying disease mechanisms. By bridging basic mechanistic insights with pharmacological interventions, this review aims to support translational progress toward mechanism-based therapies for DN.
1. Introduction
Diabetic neuropathy (DN) is one of the most prevalent and debilitating complications of diabetes mellitus, affecting up to 50% of individuals with type 1 or type 2 diabetes. Among its various forms, diabetic peripheral neuropathy is the most common, characterized by progressive, asymmetrical, length-dependent nerve damage that typically begins distally in the lower limbs. Other subtypes include autonomic neuropathy, proximal neuropathy (diabetic amyotrophy), and focal or multifocal neuropathies, each presenting with distinct clinical features [1].
Characterized by progressive, symmetrical nerve damage, DN often presents with a combination of sensory loss and neuropathic pain, such as burning, tingling, or electric shock-like sensations, typically starting in the distal lower extremities [2]. Over time, these symptoms can severely impair the quality of life, increase the risk of foot ulcers, and lead to lower limb amputations [3]. The likelihood of developing DN rises with longer disease duration, inadequate glycemic control, and additional cardiovascular risk factors [4].
Despite advances in understanding DN pathogenesis, current treatment options remain largely symptomatic and insufficient. Pain relief is the primary treatment goal, as it can improve physical function, sleep, mood, and overall well-being, enhancing the quality of life and promoting physical activity [5]. First-line pharmacological therapies—including tricyclic antidepressants, serotonin–norepinephrine reuptake inhibitors, and gabapentinoids [6]—are often limited by modest efficacy and undesirable side effects [7,8,9,10,11,12,13,14]. Moreover, only a minority of patients achieve significant pain relief, underscoring the urgent need for more effective disease-modifying interventions [15].
Growing preclinical evidence highlights the potential of drug repurposing—using existing pharmacological agents developed for other indications—to target the underlying mechanisms of DN. Compounds originally approved for metabolic disorders, neurodegenerative diseases, or cardiovascular conditions have demonstrated promising effects in animal models of DN, modulating key pathogenic processes, such as oxidative stress, neuroinflammation, ion channel dysfunction, and mitochondrial impairment [16,17,18].
However, despite this emerging body of research, there remains a lack of comprehensive, mechanism-focused reviews that integrate these preclinical findings with the broader pathophysiological context of DN.
This narrative review addresses this gap by providing a structured overview of repurposed pharmacological agents with demonstrated efficacy in preclinical models of DN. We categorize these agents based on their primary mechanisms of action, link them to specific pathophysiological targets, and critically evaluate their potential for clinical application. By bridging fundamental research with therapeutic development, this review aims to support the translation of basic science into effective, mechanism-based treatments for diabetic neuropathy.
2. Materials and Methods
A focused literature review was conducted using PubMed to identify relevant in vivo preclinical studies investigating potential therapeutic agents for DN. The search was limited to English-language publications, prioritizing recent studies from 2020 to 2025 and considering key older research. The following keywords and MeSH terms were used: “preclinical”, “rat”, “mice”, OR “rodents” AND “diabetic neuropathic pain”, “diabetic neuropathy”, OR “peripheral neuropathy”. Inclusion criteria were designed to ensure study quality and relevance. Eligible studies had to (1) be original research articles published in peer-reviewed journals; (2) involve rodent models of DN; and (3) report significant findings on therapeutic agents, whether used alone or in combination. Additionally, studies needed to provide details on drug names, dosages, mechanisms of action, and the species used. Studies not including this information were excluded.
3. Pathogenesis of DN
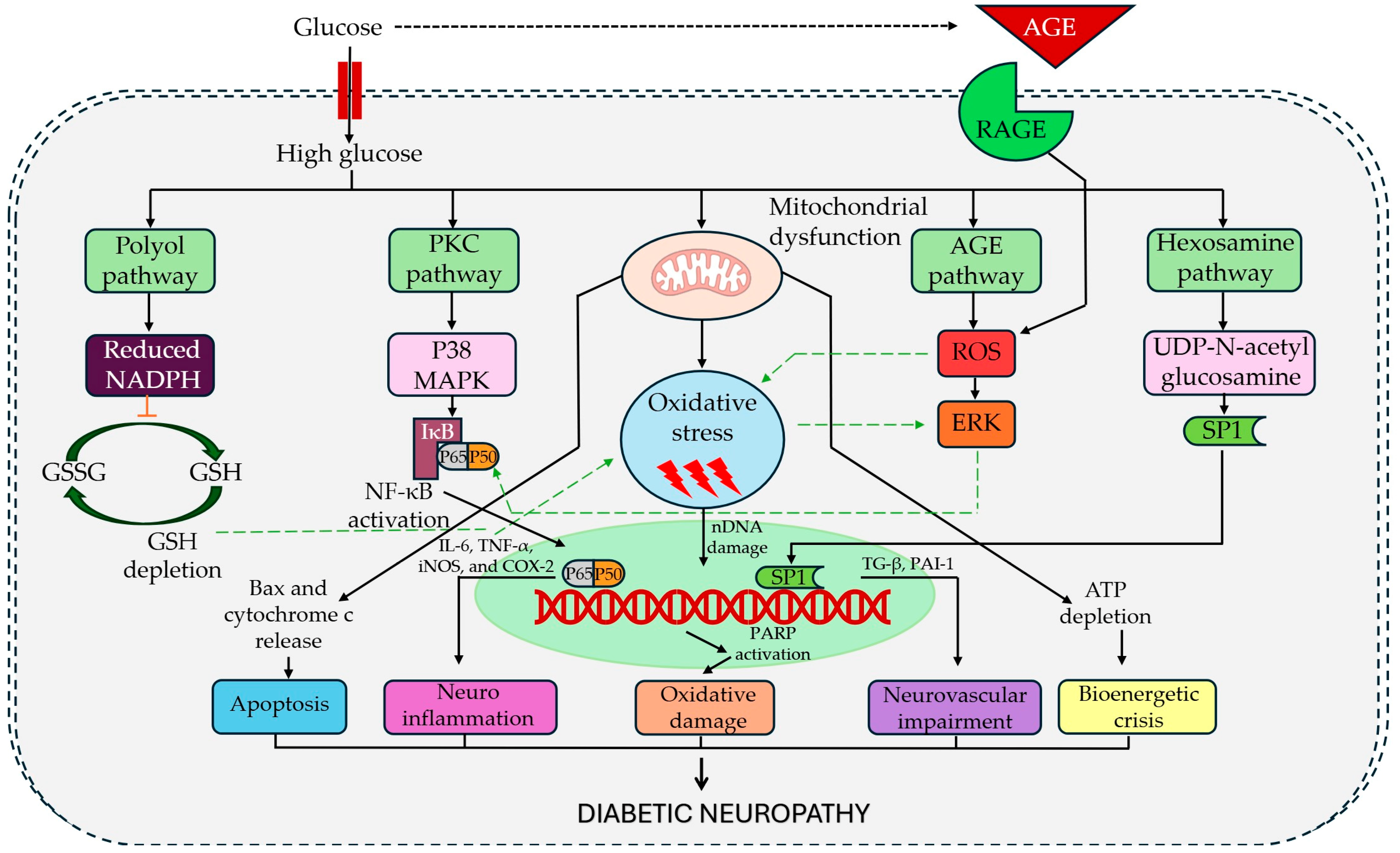
DN is a complex, multifactorial disorder driven by a convergence of metabolic abnormalities and neuroimmune dysfunction. Chronic hyperglycemia, often accompanied by dyslipidemia and insulin resistance, triggers a cascade of injurious pathways that ultimately damage peripheral nerves [19]. These include the hyperactivity of glucose metabolic routes (polyol, protein kinase C, hexosamine, and advanced glycation end-product pathways) that generate toxic intermediates and oxidative stress, impairing the microvasculature that nourishes the nerves. The result is metabolic dysfunction and microvascular damage leading to nerve fiber degeneration, Schwann cell injury, and demyelination [19,20]. In parallel, diabetes induces oxidative stress and neuroinflammation, contributing to neural injury and pain sensitization [19,20]. Importantly, these molecular insults also disrupt neuronal ion channel function, promoting ion channel modulation and neuronal hyperexcitability in primary afferents and setting the stage for central sensitization within the spinal cord [20]. Together, these mechanisms form the pathophysiological basis of DN and highlight numerous potential targets for therapeutic intervention (Figure 1).
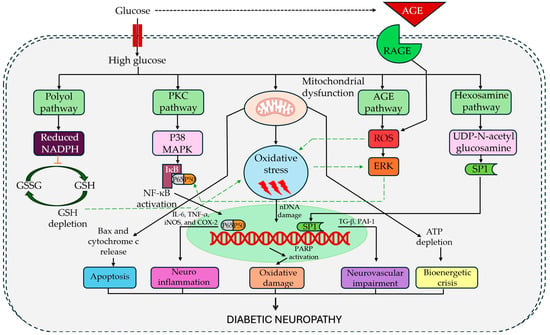
Figure 1.
Pathophysiological basis of diabetic neuropathy. Legend: AGE, advanced glycation end-products; RAGE, receptor for advanced glycation end-products; ROS, reactive oxygen species; ERK, extracellular signal-regulated kinase; PKC, protein kinase C; P38 MAPK, p38 mitogen-activated protein kinase; NF-κB, nuclear factor kappa-light-chain-enhancer of activated B cells; IκB, inhibitor of NF-κB; IL-6, interleukin-6; TNF-α, tumor necrosis factor-alpha; iNOS, inducible nitric oxide synthase; COX-2, cyclooxygenase-2; GSH, reduced glutathione; GSSG, oxidized glutathione; NADPH, nicotinamide adenine dinucleotide phosphate (reduced form); Bax, Bcl-2-associated X protein; SPI, specificity protein 1; nDNA, nuclear DNA; PARP, poly (ADP-ribose) polymerase; TGF-β, transforming growth factor-beta; PAI-1, plasminogen activator inhibitor-1; SPT1, serine palmitoyltransferase long chain base subunit 1; UDP-N-acetylglucosamine, uridine diphosphate N-acetylglucosamine; ATP, adenosine triphosphate.
3.1. Metabolic Dysfunction and Microvascular Damage
Persistent hyperglycemia disrupts normal metabolism, leading to toxic metabolite buildup that damages peripheral nerves. Excess glucose is channeled into the polyol, hexosamine, and protein kinase C (PKC) pathways that contribute to the generation of advanced glycation end-products (AGEs). Each pathway contributes to neuronal injury. Sorbitol depletes myoinositol and impairs Na+/K+-ATPase, affecting axonal conduction [21]. AGEs alter proteins and activate specific receptors, inducing oxidative stress and inflammation [21].
At the same time, insulin resistance or deficiency reduces neurotrophic support, promoting axonal atrophy and impairing repair [22]. Diabetes-induced dyslipidemia causes lipid buildup in nerves, increasing oxidative damage and inflammation [22].
Beyond metabolic toxicity, diabetes disrupts the microvascular supply to peripheral nerves. Chronic hyperglycemia impairs the vasa nervorum, leading to basement membrane thickening and endothelial dysfunction [23,24,25,26]. This process is exacerbated by PKC activation, which alters the expression of the vascular endothelial growth factor and promotes vasoconstriction [27,28]. The resulting reduction in perfusion causes endoneurial hypoxia and energy failure, contributing to axonal degeneration and demyelination [29,30]. In painful DN, these microvascular abnormalities are even more pronounced, with altered skin microvascular regulation [31]. These findings underscore how metabolic and vascular dysfunction converge to drive nerve injury in DN.
3.2. Oxidative Stress
Oxidative stress is a key driver of DN, fueled by an excessive production of reactive species of oxygen (ROS) and impaired antioxidant defenses [32]. Hyperglycemia promotes ROS generation through mitochondrial overload, NADPH oxidase 2/4 activation [33,34], and glucose or lipid auto-oxidation [35,36]. The reactive species damage neurons and Schwann cells by oxidizing DNA, lipids, and proteins [37,38]. Although Schwann cells initially mount antioxidant responses, prolonged ROS exposure causes mitochondrial dysfunction, NADPH oxidase 4-mediated stress, and apoptosis [34,39,40]. ROS also activate PKC and c-Jun N-terminal kinase, further amplifying nerve injury [41,42].
Lipids also contribute to nerve damage [1]. Diabetic nerves exhibit increased lipid peroxidation and DNA oxidation, correlating with neuropathy severity [43]. Cholesterol-derived oxysterols, along with oxidized LDL, activate inflammatory signaling via LOX-1, Toll-like receptor 4, and AGE receptors [37,44,45,46,47]. This cascade promotes caspase-3 activation, nuclear DNA degradation, and neuronal damage, promoting inflammation, oxidative stress, and nerve damage [37,44,45,46,47].
Importantly, oxidative stress is not only a consequence but also a driver of metabolic imbalance. ROS activate poly(ADP-ribose) polymerase, depleting NAD+, impairing glycolysis, and enhancing polyol and AGE pathway activity, creating a vicious cycle that accelerates nerve fiber loss.
3.3. Neuroinflammation
Once considered a purely metabolic complication, DN is now recognized as a disorder with a strong neuroinflammatory component. Chronic hyperglycemia induces low-grade systemic inflammation, reflected by elevated proinflammatory cytokines and acute-phase reactants, which correlate directly with the onset and progression of diabetic polyneuropathy [48]. In the peripheral nerves, hyperglycemia and dyslipidemia disrupt endothelial integrity, increasing blood–nerve barrier permeability and allowing monocyte and T-cell infiltration [49]. Activated macrophages and lymphocytes release cytokines and chemokines that damage neurons and Schwann cells while sensitizing nociceptors. Experimental models show that endoneurial macrophage buildup is associated with small fiber loss and NeP [43]. Additionally, hyperglycemia impairs Schwann cell function, reducing neurotrophic factor levels while increasing proinflammatory signaling, including CXCR3-mediated T-cell recruitment [50].
Neuroinflammation extends beyond peripheral nerves, with immune activation in the central nervous system playing a key role in NeP. Diabetes and nerve injury activate dorsal horn microglia that become hypertrophic and express ionized calcium-binding adaptor molecule 1 [51,52]. Hyperglycemia and ATP further stimulate P2X receptors, promoting cytokine release and amplifying nociceptive signaling [53]. Microglia-derived brain-derived neurotrophic factor disrupts chloride homeostasis, reducing inhibitory control in dorsal horn neurons [54], while astrocyte activation reinforces central sensitization through chemokines and glutamate release.
3.4. Ion Channel Modulation and Neuronal Hyperexcitability
A hallmark of diabetic NeP is sensory neuron hyperexcitability. Despite the axonal loss, surviving nociceptors develop spontaneous activity due to diabetes-induced changes in ion channel expression and function [22,55].
Several voltage-gated sodium channels, including Nav1.3, Nav1.6, Nav1.7, and Nav1.9, were upregulated in the dorsal root ganglia of streptozotocin-induced diabetic rodents. These changes contribute to the development of thermal and mechanical allodynia [56]. Furthermore, gain-of-function mutations in the SCN9A gene, which encodes Nav1.7, have been directly linked to painful DN in humans [57].
Hyperglycemia also elevates methylglyoxal, a glycolytic byproduct that modifies Nav1.8 and TRPA1 channels, further increasing nociceptor sensitivity [58,59,60,61]. Similarly, the heat-sensitive capsaicin receptors TRPV1 are also upregulated or sensitized in DN, possibly via PKC-mediated phosphorylation, contributing to burning pain [62].
Other excitatory channels, including T-type calcium channels such as Cav3.2, N-methyl-D-aspartate (NMDA), and P2X receptors, are frequently upregulated, amplifying nociceptive transmission [63,64,65]. Meanwhile, inhibitory mechanisms are diminished; potassium channels, such as Kv1, Kv7, and ATP-sensitive potassium channels, are down-regulated in diabetic rodents, disrupting neuronal repolarization, promoting ectopic firing, and facilitating central sensitization [66].
3.5. Mitochondrial Dysfunction
Mitochondrial dysfunction and impaired energy metabolism are key features of hyperglycemia-induced nerve damage [67,68]. Chronic hyperglycemia alters mitochondrial membrane potential, impairing respiration and ATP production [69,70,71].
This dysfunction contributes to axonal degeneration, particularly through toxic acylcarnitine accumulation in Schwann cells, dorsal root ganglion neurons, and axons [72]. Additionally, elevated free fatty acids, undergoing excessive β-oxidation due to hyperlipidemia, further damage peripheral nerves—especially Schwann cells [73]—by increasing ROS production and promoting inflammation. This inflammatory response is amplified by activated macrophages, which release cytokines and chemokines, perpetuating nerve injury [74].
3.6. Central Sensitization
In diabetes, persistent nociceptor activity and neuroinflammation drive central sensitization—an exaggerated pain response within the central nervous system. In DN, ongoing peripheral input increases excitatory neurotransmitters, such as glutamate and substance P, in the dorsal horn, amplifying pain signaling. NMDA receptor overactivation and reduced inhibitory control contribute to allodynia. Additionally, activated microglia and astrocytes release proinflammatory cytokines and brain-derived neurotrophic factor that reduce GABA-mediated inhibition. These cytokines further enhance NMDA receptor activity and activate intracellular kinases, perpetuating a sensitized state [75].
In animal models of diabetes, increased extracellular signal-regulated kinase (ERK) phosphorylation in spinal neurons and astrocytes correlates with mechanical hypersensitivity, while ERK inhibition reduces pain behavior. These central changes can become self-sustaining, allowing pain to persist even when glucose levels normalize [75].
Painful DN also involves supraspinal changes. Neuroimaging studies reveal cortical reorganization, with reduced gray matter in the somatosensory cortex and increased activity in pain-related regions such as the insula and anterior cingulate cortex [76]. Altered connectivity is also seen in ascending and descending pathways [77,78,79]. Although it remains unclear whether these changes are a cause or consequence of chronic pain, they reinforce the role of brain-level central sensitization in DN.
Oxidative stress, inflammation, and ion channel dysfunction are interrelated mechanisms that progressively amplify each other in painful DN. Hyperglycemia-driven oxidative stress activates redox-sensitive pathways like the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathway [80], leading to proinflammatory cytokine release, which amplifies oxidative injury and disrupts Schwann cell function [81,82]. These inflammatory mediators also alter ion channel expression and activity, enhancing nociceptor excitability [83,84]. Aberrant neuronal firing promotes glial and immune activation, creating a vicious cycle of inflammation, oxidative stress, and neurodegeneration that drives chronic pain and demyelination in DN [85].
4. Substances with Potential Effectiveness in Treating DN
Various pharmacological substances have been investigated in animal models of DN, targeting both symptom management and underlying disease mechanisms. These compounds exhibit diverse modes of action, including anti-inflammatory, antioxidant, neuroprotective, and ion channel-modulating effects. Some primarily attenuate NeP—symptoms such as mechanical allodynia and thermal hyperalgesia—while others show potential for slowing or reversing neurodegenerative processes.
Most preclinical studies rely on genetic or chemically induced models, using streptozotocin or alloxan, which cause selective destruction of pancreatic β-cells and persistent hyperglycemia. These models are widely accepted for replicating key features of type 1 diabetes and its complications, including sensory hypersensitivity, oxidative stress, nerve fiber loss, and neuroinflammation.
As discussed in Section 3, mitochondrial dysfunction, oxidative stress, and chronic low-grade inflammation are key contributors to peripheral nerve damage in DN. Consequently, pharmacological agents that restore metabolic balance, improve mitochondrial function, and exert antioxidant and anti-inflammatory effects are of growing interest as potential disease-modifying therapies. Table 1 summarizes preclinical studies investigating such compounds in experimental models of DN. These agents, which have already been approved for metabolic or cardiovascular indications, have shown the ability to reduce oxidative stress, modulate inflammatory pathways, and improve mitochondrial homeostasis, ultimately alleviating neuropathic symptoms.

Table 1.
Metabolic and mitochondrial modulators with antioxidant and anti-inflammatory effects in animal models of DN.
Mitochondrial dysfunction and oxidative stress are central drivers of neuronal injury in DN. However, experimental evidence increasingly shows that agents targeting these pathways rarely exert isolated effects. Instead, antioxidant and mitochondrial protective compounds often engage overlapping mechanisms that include anti-inflammatory actions and direct neuroprotection, collectively contributing to improved nerve function and pain relief.
Table 2 summarizes pharmacological agents evaluated in animal models of DN that demonstrate this multi-dimensional activity profile. These substances, originally developed for diverse clinical indications, show the ability to attenuate oxidative damage, preserve mitochondrial function, modulate inflammatory responses, and support structural and functional nerve integrity. This mechanistic overlap highlights the interconnected nature of oxidative stress, mitochondrial failure, inflammation, and neurodegeneration in DN pathogenesis.
Table 2.
Anti-oxidative and mitochondrial protective agents with overlapping anti-inflammatory and neuroprotective actions in animal models of DN.
Increased proinflammatory cytokine signaling, microglial activation, and dysfunction in pain modulatory circuits contribute to both peripheral nerve injury and central sensitization, sustaining chronic pain even when metabolic factors are addressed. A growing number of pharmacological agents have demonstrated the ability to modulate these pathways in experimental models of DN by attenuating cytokine production, suppressing glial activation, or restoring neuroprotective signaling. Many of these compounds act at the intersection of inflammation, immune activation, and pain processing, offering promising therapeutic potential. Table 3 summarizes these agents, detailing their effects on neuroinflammatory mediators, central sensitization markers, and pain-related outcomes in animal models of DN.
Table 3.
Agents targeting neuroinflammation, cytokine signaling, and central sensitization in animal models of DN.
Aberrant neuronal excitability is a key contributor to neuropathic pain and sensory deficits in diabetic neuropathy (DN). Targeting ion channels and pathways involved in neuronal hyperactivity has emerged as a promising strategy for symptom relief and potential disease modification. Table 4 summarizes preclinical studies evaluating repurposed pharmacological agents that modulate ion channels or regulate neuronal excitability in animal models of DN.
Table 4.
Ion channel modulators and regulators of neuronal hyperexcitability in animal models of DN.
5. Discussion
This review highlights emerging evidence for repurposed pharmacological agents in DN, focusing on their analgesic efficacy, disease-modifying effects, and underlying mechanisms based on preclinical studies. By integrating findings from animal models, we explore how these compounds influence pain signaling, neuroinflammation, oxidative stress, and neurodegeneration.
5.1. Modulating Neuronal Hyperexcitability
Retigabine [140], reboxetine [126], and ifenprodil [127] significantly reduced mechanical and thermal hypersensitivity in animal models by modulating abnormal neuronal firing and enhancing descending inhibitory pathways [126,127,140]. Cilostazol improved mechanical allodynia and preserved nociceptive fibers without affecting thermal pain, suggesting selective modulation of Aβ and Aδ fibers [142].
Additional agents such as drofenine [151] and N-acetylcysteine [144] further support the role of ion channel modulation in DN, improving sensory response and reducing pain [151] via TRPV1, NMDA, and P2X7 pathways [144]. Muscarinic M1 receptor antagonists (pirenzepine, atropine, oxybutynin) further demonstrated robust analgesic and neuroprotective effects [146,148].
5.2. Mitigating Inflammation and Oxidative Stress
Chronic inflammation and oxidative stress are central to both pain and neurodegeneration in DN. Agents such as telmisartan [123], clavulanic acid [124], metformin [88,135], melatonin [114,156], pentoxifylline [120,133], semaglutide [90], and atorvastatin [91] consistently reduced inflammatory cytokines (TNF-α, IL-1β, IL-6) and oxidative markers (MDA, ROS), correlating with improved behavioral and structural outcomes.
Etifoxine [129] and bupivacaine [131] also reduced inflammation and improved pain thresholds. Topiramate enhanced neuroprotection via glial modulation [18], while liraglutide targeted central inflammation through NLRP3 inhibition [102].
5.3. Promoting Neuroprotection, Remyelination, and Mitochondrial Function
Alirocumab [93], pramipexole [122], melatonin [156], and tropisetron [115] promoted nerve preservation by enhancing neurotrophic factors and mitochondrial biogenesis. Vincamine [112] and amlodipine [106] improved mitochondrial function via AMPK/SIRT1/PGC-1α signaling, which is crucial for maintaining neuronal energy homeostasis. Romidepsin, a histone deacetylase inhibitor, facilitated nerve regeneration through epigenetic modulation [118].
5.4. Modulating Glial Activation and Central Sensitization
Central sensitization and glial activation are major drivers of chronic pain. Clavulanic acid [124], ifenprodil [127], semaglutide [90], cilostazol [142], etifoxine [129], topiramate [18], and bupivacaine [131] reduced microglial reactivity and inflammatory cytokine release, indicating that glia-targeted therapies may stabilize pain processing circuits.
5.5. Mitigating Advanced Glycation and Metabolic Dysregulation
Gliclazide [98] lowered sorbitol buildup and oxidative stress, while alirocumab [93] and atorvastatin [91] improved lipid profiles and suppressed AGE signaling.
Topiroxostat, a xanthine oxidase inhibitor, preserved nerve function and structure by inhibiting macrophage polarization and reducing systemic oxidative stress, highlighting its dual antioxidant and anti-inflammatory capacity [104].
Metformin alone or associated with duloxetine, oxycodone, or vitamin B12 consistently showed enhanced efficacy in reducing pain and improving neural integrity, driven by metabolic regulation via AMPK activation and ROS reduction [95].
5.6. Multi-Targeted Approaches
Combination therapies offer synergistic effects across several pathogenic pathways. Melatonin + gabapentin [156], rolipram + pentoxifylline [133], and sildenafil + metformin [135,137] demonstrated enhanced antinociceptive and neuroprotective outcomes.
Similarly, the combination of agomelatine + morphine yielded longer-lasting analgesia while attenuating morphine tolerance, suggesting that melatonergic signaling could be harnessed to optimize opioid therapy [153].
Metformin co-administered with various agents or administered intrathecally displayed dose-sparing effects, broadening its translational value [95,135,137].
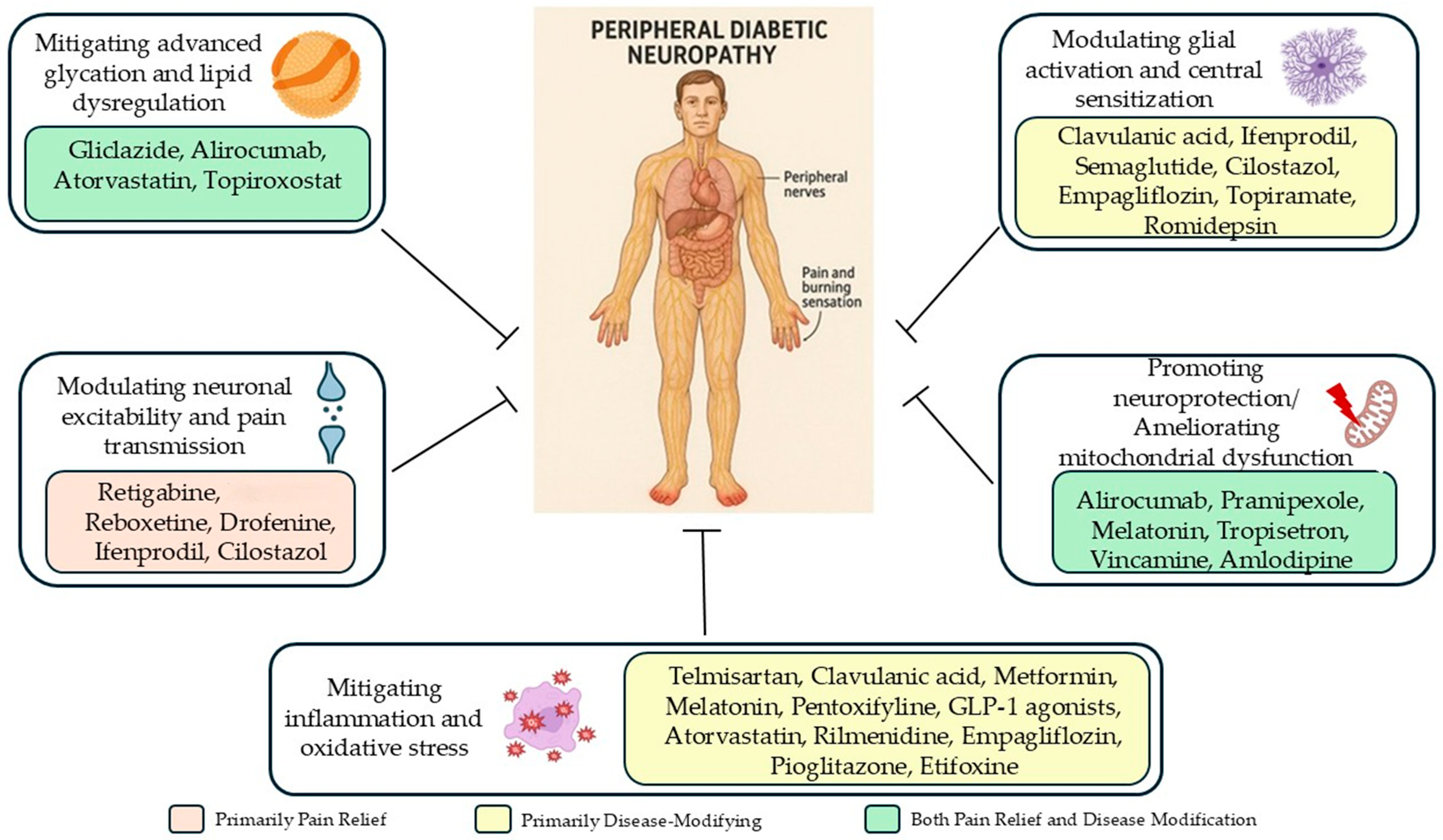
Figure 2 summarizes the mechanisms of action of these repurposed antineuropathic agents.
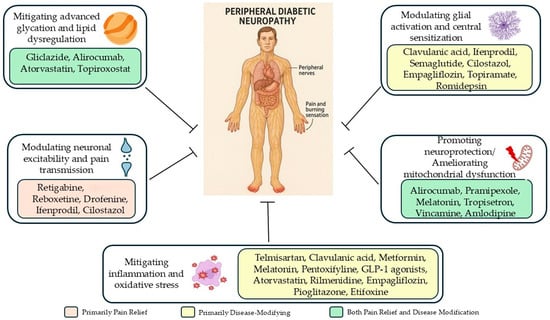
Figure 2.
Pathophysiological mechanisms targeted by repurposed drugs in diabetic neuropathy: from pain relief to disease modification.
Although current clinical guidelines for the management of DN primarily recommend agents such as duloxetine, pregabalin, and tricyclic antidepressants for symptomatic relief, these drugs are often limited by partial efficacy and side effects. The repurposed pharmacological agents discussed here, while not currently included in guideline-based treatment algorithms, may complement or enhance existing therapies through disease-modifying effects. Their ability to target multiple underlying mechanisms—such as neuroinflammation, oxidative stress, and mitochondrial dysfunction—offers a promising direction for expanding the therapeutic landscape.
However, clinical validation is necessary before these compounds can be integrated into evidence-based treatment strategies. Despite promising preclinical results, clinical translation remains inconsistent and challenging.
Several compounds that exhibited therapeutic efficacy in rodent models did not translate into clinical success. Liraglutide (1.2–1.8 mg/day subcutaneously for 26 weeks) reduced inflammation but failed to improve neuropathy outcomes in humans, possibly due to the advanced stage of neuropathic damage in the tested patients [158]. Similarly, pentoxifylline was unable to demonstrate clinical efficacy in a one-year randomized controlled trial [159], while the utility of topiramate has been limited by adverse effects, including sensory disturbances, fatigue, and cognitive dysfunction [160].
Other agents have produced varied outcomes. Telmisartan (40–80 mg) [161] and aliskiren [162] reduced symptoms and inflammation in small trials, while cilostazol (100–200 mg) improved walking speed but not neuropathic symptoms [163]. Clinical data on metformin remain conflicting, with some studies reporting nerve preservation [164] and others indicating increased DN risk at high doses, possibly linked to metformin-induced vitamin B12 deficiency [165].
Encouragingly, empagliflozin (25 mg/day) reduced pain scores, improved electrophysiology, and decreased serum levels of neuron-specific enolase and MDA [166]. Semaglutide, combined with cagrilintide, is under investigation in painful DN [167].
The variability in animal models, disease stage, dosing regimens, and outcome measures limits direct clinical applicability. Many repurposed agents show efficacy in early-stage DN under controlled laboratory conditions. Furthermore, species-specific differences in drug metabolism and pain processing can obscure clinical relevance. The lack of standardized biomarkers for early detection and treatment response in DN complicates trial design and therapeutic validation.
To advance these preclinical discoveries toward clinical application, future research should prioritize rigorous, standardized animal models that better mimic human DN progression—including type 2 diabetes and mixed neuropathies. Longitudinal studies examining pain relief and neuroprotection are essential to assess true disease-modifying potential. Combining pharmacological agents targeting distinct mechanisms (e.g., inflammation, oxidative stress, and ion channel modulation) may enhance efficacy and reduce required doses.
6. Conclusions
Repurposed pharmacological agents show potential for improving DN management by targeting key pathogenic mechanisms. Greater clinical benefits are likely achieved through multi-targeted therapies that address both symptom control and disease progression. However, rigorous clinical validation is essential before these approaches can be integrated into evidence-based care.
Author Contributions
Conceptualization, C.P.; methodology, C.P. and A.Z.; data curation, C.P. and O.C.Ș.; writing—original draft preparation, O.C.Ș., C.P., and C.A.; writing—review and editing, A.Z.; visualization, C.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Acknowledgments
Publication of this paper was supported by the University of Medicine and Pharmacy Carol Davila through the institutional program Publish not Perish.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Feldman, E.L.; Callaghan, B.C.; Pop-Busui, R.; Zochodne, D.W.; Wright, D.E.; Bennett, D.L.; Bril, V.; Russell, J.W.; Viswanathan, V. Diabetic Neuropathy. Nat. Rev. Dis. Prim. 2019, 5, 41. [Google Scholar] [CrossRef] [PubMed]
- Terminology|International Association for the Study of Pain. Available online: https://www.iasp-pain.org/resources/terminology/ (accessed on 17 October 2022).
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.B.; et al. Neuropathic Pain. Nat. Rev. Dis. Prim. 2017, 3, 17002. [Google Scholar] [CrossRef]
- Hicks, C.W.; Selvin, E. Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes. Curr. Diab. Rep. 2019, 19, 86. [Google Scholar] [CrossRef]
- Bates, D.; Schultheis, B.C.; Hanes, M.C.; Jolly, S.M.; Chakravarthy, K.V.; Deer, T.R.; Levy, R.M.; Hunter, C.W. A Comprehensive Algorithm for Management of Neuropathic Pain. Pain Med. 2019, 20 (Suppl. 1), S2–S12. [Google Scholar] [CrossRef] [PubMed]
- Attal, N. Pharmacological Treatments of Neuropathic Pain: The Latest Recommendations. Rev. Neurol. 2019, 175, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Moisset, X.; Bouhassira, D.; Avez Couturier, J.; Alchaar, H.; Conradi, S.; Delmotte, M.H.; Lanteri-Minet, M.; Lefaucheur, J.P.; Mick, G.; Piano, V.; et al. Pharmacological and Non-Pharmacological Treatments for Neuropathic Pain: Systematic Review and French Recommendations. Rev. Neurol. 2020, 176, 325–352. [Google Scholar] [CrossRef]
- Hennemann-Krause, L.; Sredni, S. Systemic Drug Therapy for Neuropathic Pain. Rev. Dor 2016, 17, 91–94. [Google Scholar] [CrossRef]
- Rowbotham, M.C. Tricyclic Antidepressants and Opioids-Better Together? Pain 2015, 156, 1373–1374. [Google Scholar] [CrossRef]
- Shinu, P.; Morsy, M.A.; Nair, A.B.; Al Mouslem, A.K.; Venugopala, K.N.; Goyal, M.; Bansal, M.; Jacob, S.; Deb, P.K. Novel Therapies for the Treatment of Neuropathic Pain: Potential and Pitfalls. J. Clin. Med. 2022, 11, 3002. [Google Scholar] [CrossRef]
- Kopsky, D.J.; Keppel Hesselink, J.M. High Doses of Topical Amitriptyline in Neuropathic Pain: Two Cases and Literature Review. Pain Pract. 2012, 12, 148–153. [Google Scholar] [CrossRef]
- Gabriel, M.; Sharma, V. Antidepressant Discontinuation Syndrome. CMAJ 2017, 189, E747. [Google Scholar] [CrossRef] [PubMed]
- Maloney, J.; Pew, S.; Wie, C.; Gupta, R.; Freeman, J.; Strand, N. Comprehensive Review of Topical Analgesics for Chronic Pain. Curr. Pain Headache Rep. 2021, 25, 7. [Google Scholar] [CrossRef]
- Attal, N.; de Andrade, D.C.; Adam, F.; Ranoux, D.; Teixeira, M.J.; Galhardoni, R.; Raicher, I.; Üçeyler, N.; Sommer, C.; Bouhassira, D. Safety and Efficacy of Repeated Injections of Botulinum Toxin A in Peripheral Neuropathic Pain (BOTNEP): A Randomised, Double-Blind, Placebo-Controlled Trial. Lancet Neurol. 2016, 15, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for Neuropathic Pain in Adults: A Systematic Review and Meta-Analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef]
- Cao, X.J.; Wu, R.; Qian, H.Y.; Chen, X.; Zhu, H.Y.; Xu, G.Y.; Sun, Y.Z.; Zhang, P.A. Metformin Attenuates Diabetic Neuropathic Pain via AMPK/NF-ΚB Signaling Pathway in Dorsal Root Ganglion of Diabetic Rats. Brain Res. 2021, 1772, 147663. [Google Scholar] [CrossRef] [PubMed]
- Yalçın, M.B.; Bora, E.S.; Çakır, A.; Akbulut, S.; Erbaş, O. Autophagy and Anti-Inflammation Ameliorate Diabetic Neuropathy with Rilmenidine. Acta Cirúrgica Bras. 2023, 38, e387823. [Google Scholar] [CrossRef]
- Attia, M.A.; Soliman, N.; Eladl, M.A.; Bilasy, S.E.; El-Abaseri, T.B.; Ali, H.S.; Abbas, F.; Ibrahim, D.; Osman, N.M.S.; Hashish, A.A.; et al. Topiramate Affords Neuroprotection in Diabetic Neuropathy Model via Downregulating Spinal GFAP/Inflammatory Burden and Improving Neurofilament Production. Toxicol. Mech. Methods 2023, 33, 563–577. [Google Scholar] [CrossRef]
- Yang, Y.; Zhao, B.; Wang, Y.; Lan, H.; Liu, X.; Hu, Y.; Cao, P. Diabetic Neuropathy: Cutting-Edge Research and Future Directions. Signal Transduct. Target. Ther. 2025, 10, 132. [Google Scholar] [CrossRef]
- Tesfaye, S.; Boulton, A.J.M.; Dickenson, A.H. Mechanisms and Management of Diabetic Painful Distal Symmetrical Polyneuropathy. Diabetes Care 2013, 36, 2456–2465. [Google Scholar] [CrossRef]
- Feldman, E.L.; Nave, K.A.; Jensen, T.S.; Bennett, D.L.H. New Horizons in Diabetic Neuropathy: Mechanisms, Bioenergetics, and Pain. Neuron 2017, 93, 1296–1313. [Google Scholar] [CrossRef]
- Rosenberger, D.C.; Blechschmidt, V.; Timmerman, H.; Wolff, A.; Treede, R.-D. Challenges of Neuropathic Pain: Focus on Diabetic Neuropathy. J. Neural Transm. 2020, 127, 589–624. [Google Scholar] [CrossRef] [PubMed]
- Thrainsdottir, S.; Malik, R.A.; Dahlin, L.B.; Wiksell, P.; Eriksson, K.F.; Rosén, I.; Petersson, J.; Greene, D.A.; Sundkvist, G. Endoneurial Capillary Abnormalities Presage Deterioration of Glucose Tolerance and Accompany Peripheral Neuropathy in Man. Diabetes 2003, 52, 2615–2622. [Google Scholar] [CrossRef] [PubMed]
- Hill, R.E.; Williams, P.E. Perineurial Cell Basement Membrane Thickening and Myelinated Nerve Fibre Loss in Diabetic and Nondiabetic Peripheral Nerve. J. Neurol. Sci. 2004, 217, 157–163. [Google Scholar] [CrossRef]
- Nukada, H. Ischemia and Diabetic Neuropathy. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2014; pp. 469–487. [Google Scholar]
- Cameron, N.E.; Eaton, S.E.M.; Cotter, M.A.; Tesfaye, S. Vascular Factors and Metabolic Interactions in the Pathogenesis of Diabetic Neuropathy. Diabetologia 2001, 44, 1973–1988. [Google Scholar] [CrossRef]
- Mizukami, H.; Osonoi, S. Collateral Glucose-Utlizing Pathwaya in Diabetic Polyneuropathy. Int. J. Mol. Sci. 2020, 22, 94. [Google Scholar] [CrossRef]
- Bansal, D.; Badhan, Y.; Gudala, K.; Schifano, F. Ruboxistaurin for the Treatment of Diabetic Peripheral Neuropathy: A Systematic Review of Randomized Clinical Trials. Diabetes Metab. J. 2013, 37, 375. [Google Scholar] [CrossRef] [PubMed]
- Coppey, L.J.; Davidson, E.P.; Rinehart, T.W.; Gellett, J.S.; Oltman, C.L.; Lund, D.D.; Yorek, M.A. ACE Inhibitor or Angiotensin II Receptor Antagonist Attenuates Diabetic Neuropathy in Streptozotocin-Induced Diabetic Rats. Diabetes 2006, 55, 341–348. [Google Scholar] [CrossRef]
- Yorek, M.A. Vascular Impairment of Epineurial Arterioles of the Sciatic Nerve: Implications for Diabetic Peripheral Neuropathy. Rev. Diabet. Stud. 2015, 12, 13–28. [Google Scholar] [CrossRef]
- Shillo, P.R.; Selvarajah, D.; Greig, M.; Rao, G.D.; Edden, R.A.E.; Wilkinson, I.D.; Tesfaye, S. Diabetes UK Type 2 Diabetes Research Award. Diabet. Med. 2016, 33, 15–16. [Google Scholar] [CrossRef]
- Dewanjee, S.; Das, S.; Das, A.K.; Bhattacharjee, N.; Dihingia, A.; Dua, T.K.; Kalita, J.; Manna, P. Molecular Mechanism of Diabetic Neuropathy and Its Pharmacotherapeutic Targets. Eur. J. Pharmacol. 2018, 833, 472–523. [Google Scholar] [CrossRef]
- Chen, J.-L.; Lu, J.-H.; Xie, C.-S.; Shen, Y.-J.; Wang, J.-W.; Ye, X.-Y.; Zhang, M.-B.; Jia, G.-L.; Tao, Y.-X.; Li, J.; et al. Caveolin-1 in Spinal Cord Modulates Type-2 Diabetic Neuropathic Pain through the Rac1/NOX2/NR2B Signaling Pathway. Am. J. Transl. Res. 2020, 12, 1714–1727. [Google Scholar] [CrossRef]
- Eid, S.A.; El Massry, M.; Hichor, M.; Haddad, M.; Grenier, J.; Dia, B.; Barakat, R.; Boutary, S.; Chanal, J.; Aractingi, S.; et al. Targeting the NADPH Oxidase-4 and Liver X Receptor Pathway Preserves Schwann Cell Integrity in Diabetic Mice. Diabetes 2020, 69, 448–464. [Google Scholar] [CrossRef]
- Giacco, F.; Brownlee, M. Oxidative Stress and Diabetic Complications. Circ. Res. 2010, 107, 1058–1070. [Google Scholar] [CrossRef] [PubMed]
- Fernyhough, P.; Roy Chowdhury, S.K.; Schmidt, R.E. Mitochondrial Stress and the Pathogenesis of Diabetic Neuropathy. Expert Rev. Endocrinol. Metab. 2010, 5, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Vincent, A.M.; Hayes, J.M.; McLean, L.L.; Vivekanandan-Giri, A.; Pennathur, S.; Feldman, E.L. Dyslipidemia-Induced Neuropathy in Mice. Diabetes 2009, 58, 2376–2385. [Google Scholar] [CrossRef] [PubMed]
- Tesco, G.; Lomoio, S. Pathophysiology of Neurodegenerative Diseases: An Interplay among Axonal Transport Failure, Oxidative Stress, and Inflammation? Semin. Immunol. 2022, 59, 101628. [Google Scholar] [CrossRef]
- Vincent, A.M.; Kato, K.; McLean, L.L.; Soules, M.E.; Feldman, E.L. Sensory Neurons and Schwann Cells Respond to Oxidative Stress by Increasing Antioxidant Defense Mechanisms. Antioxid. Redox Signal. 2009, 11, 425–438. [Google Scholar] [CrossRef]
- Hinder, L.M.; Figueroa-Romero, C.; Pacut, C.; Hong, Y.; Vivekanandan-Giri, A.; Pennathur, S.; Feldman, E.L. Long-Chain Acyl Coenzyme A Synthetase 1 Overexpression in Primary Cultured Schwann Cells Prevents Long Chain Fatty Acid-Induced Oxidative Stress and Mitochondrial Dysfunction. Antioxid. Redox Signal. 2014, 21, 588–600. [Google Scholar] [CrossRef]
- Xu, J.; Wu, S.; Wang, J.; Wang, J.; Yan, Y.; Zhu, M.; Zhang, D.; Jiang, C.; Liu, T. Oxidative Stress Induced by NOX2 Contributes to Neuropathic Pain via Plasma Membrane Translocation of PKCε in Rat Dorsal Root Ganglion Neurons. J. Neuroinflamm. 2021, 18, 106. [Google Scholar] [CrossRef]
- Jiao, Y.; Zhang, Y.; Wang, C.; Yu, Y.; Li, Y.; Cui, W.; Li, Q.; Yu, Y. MicroRNA-7a-5p Ameliorates Diabetic Peripheral Neuropathy by Regulating VDAC1/JNK/C-JUN Pathway. Diabet. Med. 2023, 40, e14890. [Google Scholar] [CrossRef]
- Zhu, J.; Hu, Z.; Luo, Y.; Liu, Y.; Luo, W.; Du, X.; Luo, Z.; Hu, J.; Peng, S. Diabetic Peripheral Neuropathy: Pathogenetic Mechanisms and Treatment. Front. Endocrinol. 2024, 14, 1265372. [Google Scholar] [CrossRef] [PubMed]
- Nowicki, M.; Müller, K.; Serke, H.; Kosacka, J.; Vilser, C.; Ricken, A.; Spanel-Borowski, K. Oxidized Low-Density Lipoprotein (OxLDL)-Induced Cell Death in Dorsal Root Ganglion Cell Cultures Depends Not on the Lectin-like OxLDL Receptor-1 but on the Toll-like Receptor-4. J. Neurosci. Res. 2010, 88, 403–412. [Google Scholar] [CrossRef]
- Vincent, A.M.; Perrone, L.; Sullivan, K.A.; Backus, C.; Sastry, A.M.; Lastoskie, C.; Feldman, E.L. Receptor for Advanced Glycation End Products Activation Injures Primary Sensory Neurons via Oxidative Stress. Endocrinology 2007, 148, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.N.; Hanni, K.B.; Markesbery, W.R. Oxidized Low-Density Lipoprotein Induces Neuronal Death: Implications for Calcium, Reactive Oxygen Species, and Caspases. J. Neurochem. 1999, 72, 2601–2609. [Google Scholar] [CrossRef]
- Cotter, M.A.; Cameron, N.E. Effect of the NAD(P)H Oxidase Inhibitor, Apocynin, on Peripheral Nerve Perfusion and Function in Diabetic Rats. Life Sci. 2003, 73, 1813–1824. [Google Scholar] [CrossRef] [PubMed]
- Herder, C.; Kannenberg, J.M.; Huth, C.; Carstensen-Kirberg, M.; Rathmann, W.; Koenig, W.; Heier, M.; Püttgen, S.; Thorand, B.; Peters, A.; et al. Proinflammatory Cytokines Predict the Incidence and Progression of Distal Sensorimotor Polyneuropathy: KORA F4/FF4 Study. Diabetes Care 2017, 40, 569–576. [Google Scholar] [CrossRef]
- Ji, R.-R.; Xu, Z.-Z.; Gao, Y.-J. Emerging Targets in Neuroinflammation-Driven Chronic Pain. Nat. Rev. Drug Discov. 2014, 13, 533–548. [Google Scholar] [CrossRef]
- Tang, W.; Lv, Q.; Chen, X.; Zou, J.; Liu, Z.; Shi, Y. CD8 + T Cell-Mediated Cytotoxicity toward Schwann Cells Promotes Diabetic Peripheral Neuropathy. Cell. Physiol. Biochem. 2013, 32, 827–837. [Google Scholar] [CrossRef]
- Vydyanathan, A.; Wu, Z.Z.; Chen, S.R.; Pan, H.L. A-Type Voltage-Gated K+ Currents Influence Firing Properties of Isolectin B4-Positive but Not Isolectin B4-Negative Primary Sensory Neurons. J. Neurophysiol. 2005, 93, 3401–3409. [Google Scholar] [CrossRef]
- Wang, Q.; Xie, Y.; Ma, S.; Luo, H.; Qiu, Y. Role of Microglia in Diabetic Neuropathic Pain. Front. Cell Dev. Biol. 2024, 12, 1421191. [Google Scholar] [CrossRef]
- Gao, Y.-J.; Zhang, L.; Samad, O.A.; Suter, M.R.; Yasuhiko, K.; Xu, Z.-Z.; Park, J.-Y.; Lind, A.-L.; Ma, Q.; Ji, R.-R. JNK-Induced MCP-1 Production in Spinal Cord Astrocytes Contributes to Central Sensitization and Neuropathic Pain. J. Neurosci. 2009, 29, 4096–4108. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Liu, X.; Xiong, H.; Wang, W.; Liu, Y.; Yin, L.; Tu, C.; Wang, H.; Xiang, X.; Xu, J.; et al. CXCL13/CXCR5 Signaling Contributes to Diabetes-Induced Tactile Allodynia via Activating PERK, PSTAT3, PAKT Pathways and pro-Inflammatory Cytokines Production in the Spinal Cord of Male Mice. Brain Behav. Immun. 2019, 80, 711–724. [Google Scholar] [CrossRef] [PubMed]
- Middleton, S.J.; Barry, A.M.; Comini, M.; Li, Y.; Ray, P.R.; Shiers, S.; Themistocleous, A.C.; Uhelski, M.L.; Yang, X.; Dougherty, P.M.; et al. Studying Human Nociceptors: From Fundamentals to Clinic. Brain 2021, 144, 1312–1335. [Google Scholar] [CrossRef]
- Craner, M.J.; Klein, J.P.; Renganathan, M.; Black, J.A.; Waxman, S.G. Changes of Sodium Channel Expression in Experimental Painful Diabetic Neuropathy. Ann. Neurol. 2002, 52, 786–792. [Google Scholar] [CrossRef]
- Hoeijmakers, J.G.J.; Faber, C.G.; Merkies, I.S.J.; Waxman, S.G. Channelopathies, Painful Neuropathy, and Diabetes: Which Way Does the Causal Arrow Point? Trends Mol. Med. 2014, 20, 544–550. [Google Scholar] [CrossRef]
- Andersen, S.T.; Witte, D.R.; Dalsgaard, E.-M.; Andersen, H.; Nawroth, P.; Fleming, T.; Jensen, T.M.; Finnerup, N.B.; Jensen, T.S.; Lauritzen, T.; et al. Risk Factors for Incident Diabetic Polyneuropathy in a Cohort With Screen-Detected Type 2 Diabetes Followed for 13 Years: ADDITION-Denmark. Diabetes Care 2018, 41, 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- Bierhaus, A.; Fleming, T.; Stoyanov, S.; Leffler, A.; Babes, A.; Neacsu, C.; Sauer, S.K.; Eberhardt, M.; Schnölzer, M.; Lasitschka, F.; et al. Methylglyoxal Modification of Nav1.8 Facilitates Nociceptive Neuron Firing and Causes Hyperalgesia in Diabetic Neuropathy. Nat. Med. 2012, 18, 926–933. [Google Scholar] [CrossRef]
- Andersson, D.A.; Gentry, C.; Light, E.; Vastani, N.; Vallortigara, J.; Bierhaus, A.; Fleming, T.; Bevan, S. Methylglyoxal Evokes Pain by Stimulating TRPA1. PLoS ONE 2013, 8, e77986. [Google Scholar] [CrossRef]
- Düll, M.M.; Riegel, K.; Tappenbeck, J.; Ries, V.; Strupf, M.; Fleming, T.; Sauer, S.K.; Namer, B. Methylglyoxal Causes Pain and Hyperalgesia in Human through C-Fiber Activation. Pain 2019, 160, 2497–2507. [Google Scholar] [CrossRef]
- Hong, S.; Agresta, L.; Guo, C.; Wiley, J.W. The TRPV1 Receptor Is Associated with Preferential Stress in Large Dorsal Root Ganglion Neurons in Early Diabetic Sensory Neuropathy. J. Neurochem. 2008, 105, 1212–1222. [Google Scholar] [CrossRef]
- Jagodic, M.M.; Pathirathna, S.; Nelson, M.T.; Mancuso, S.; Joksovic, P.M.; Rosenberg, E.R.; Bayliss, D.A.; Jevtovic-Todorovic, V.; Todorovic, S.M. Cell-Specific Alterations of T-Type Calcium Current in Painful Diabetic Neuropathy Enhance Excitability of Sensory Neurons. J. Neurosci. 2007, 27, 3305–3316. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, M.; Furusawa, K.; Kamijo, M.; Kimura, T.; Matsunaga, M.; Baba, M. Upregulation of MRNAs Coding for AMPA and NMDA Receptor Subunits and Metabotropic Glutamate Receptors in the Dorsal Horn of the Spinal Cord in a Rat Model of Diabetes Mellitus. Mol. Brain Res. 2005, 136, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, J.M.; dos Santos, G.G.; Neves, A.F.; Athie, M.C.P.; Bonet, I.J.M.; Nishijima, C.M.; Farias, F.H.; Figueiredo, J.G.; Hernandez-Olmos, V.; Alshaibani, S.; et al. Diabetes-Induced Neuropathic Mechanical Hyperalgesia Depends on P2X4 Receptor Activation in Dorsal Root Ganglia. Neuroscience 2019, 398, 158–170. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Li, L.; Liu, H.; Li, H.; Liu, Z.; Li, Z. KCNQ2/3/5 Channels in Dorsal Root Ganglion Neurons Can Be Therapeutic Targets of Neuropathic Pain in Diabetic Rats. Mol. Pain 2018, 14, 1744806918793229. [Google Scholar] [CrossRef]
- Rumora, A.E.; Savelieff, M.G.; Sakowski, S.A.; Feldman, E.L. Disorders of Mitochondrial Dynamics in Peripheral Neuropathy: Clues from Hereditary Neuropathy and Diabetes. Int. Rev. Neurobiol. 2019, 145, 127–176. [Google Scholar]
- Fernyhough, P. Mitochondrial Dysfunction in Diabetic Neuropathy: A Series of Unfortunate Metabolic Events. Curr. Diab. Rep. 2015, 15, 89. [Google Scholar] [CrossRef]
- Russell, J.W.; Golovoy, D.; Vincent, A.M.; Mahendru, P.; Olzmann, J.A.; Mentzer, A.; Feldman, E.L. High Glucose-induced Oxidative Stress and Mitochondrial Dysfunction in Neurons. FASEB J. 2002, 16, 1738–1748. [Google Scholar] [CrossRef]
- Chowdhury, S.K.R.; Zherebitskaya, E.; Smith, D.R.; Akude, E.; Chattopadhyay, S.; Jolivalt, C.G.; Calcutt, N.A.; Fernyhough, P. Mitochondrial Respiratory Chain Dysfunction in Dorsal Root Ganglia of Streptozotocin-Induced Diabetic Rats and Its Correction by Insulin Treatment. Diabetes 2010, 59, 1082–1091. [Google Scholar] [CrossRef]
- Rumora, A.E.; Lentz, S.I.; Hinder, L.M.; Jackson, S.W.; Valesano, A.; Levinson, G.E.; Feldman, E.L. Dyslipidemia Impairs Mitochondrial Trafficking and Function in Sensory Neurons. FASEB J. 2018, 32, 195–207. [Google Scholar] [CrossRef]
- Viader, A.; Sasaki, Y.; Kim, S.; Strickland, A.; Workman, C.S.; Yang, K.; Gross, R.W.; Milbrandt, J. Aberrant Schwann Cell Lipid Metabolism Linked to Mitochondrial Deficits Leads to Axon Degeneration and Neuropathy. Neuron 2013, 77, 886–898. [Google Scholar] [CrossRef]
- Padilla, A.; Descorbeth, M.; Almeyda, A.L.; Payne, K.; De Leon, M. Hyperglycemia Magnifies Schwann Cell Dysfunction and Cell Death Triggered by PA-Induced Lipotoxicity. Brain Res. 2011, 1370, 64. [Google Scholar] [CrossRef] [PubMed]
- Legrand-Poels, S.; Esser, N.; L’Homme, L.; Scheen, A.; Paquot, N.; Piette, J. Free Fatty Acids as Modulators of the NLRP3 Inflammasome in Obesity/Type 2 Diabetes. Biochem. Pharmacol. 2014, 92, 131–141. [Google Scholar] [CrossRef]
- Xu, X.; Chen, H.; Ling, B.-Y.; Xu, L.; Cao, H.; Zhang, Y.-Q. Extracellular Signal-Regulated Protein Kinase Activation in Spinal Cord Contributes to Pain Hypersensitivity in a Mouse Model of Type 2 Diabetes. Neurosci. Bull. 2014, 30, 53–66. [Google Scholar] [CrossRef] [PubMed]
- Shillo, P.; Yiangou, Y.; Donatien, P.; Greig, M.; Selvarajah, D.; Wilkinson, I.D.; Anand, P.; Tesfaye, S. Nerve and Vascular Biomarkers in Skin Biopsies Differentiate Painful From Painless Peripheral Neuropathy in Type 2 Diabetes. Front. Pain Res. 2021, 2, 731658. [Google Scholar] [CrossRef]
- Selvarajah, D.; Wilkinson, I.D.; Fang, F.; Sankar, A.; Davies, J.; Boland, E.; Harding, J.; Rao, G.; Gandhi, R.; Tracey, I.; et al. Structural and Functional Abnormalities of the Primary Somatosensory Cortex in Diabetic Peripheral Neuropathy: A Multimodal MRI Study. Diabetes 2019, 68, 796–806. [Google Scholar] [CrossRef]
- Teh, K.; Wilkinson, I.D.; Heiberg-Gibbons, F.; Awadh, M.; Kelsall, A.; Pallai, S.; Sloan, G.; Tesfaye, S.; Selvarajah, D. Somatosensory Network Functional Connectivity Differentiates Clinical Pain Phenotypes in Diabetic Neuropathy. Diabetologia 2021, 64, 1412–1421. [Google Scholar] [CrossRef] [PubMed]
- Segerdahl, A.R.; Themistocleous, A.C.; Fido, D.; Bennett, D.L.; Tracey, I. A Brain-Based Pain Facilitation Mechanism Contributes to Painful Diabetic Polyneuropathy. Brain 2018, 141, 357–364. [Google Scholar] [CrossRef]
- Zhou, X.; Wang, B.; Zhu, L.; Hao, S. A Novel Improved Therapy Strategy for Diabetic Nephropathy. Organogenesis 2012, 8, 18–21. [Google Scholar] [CrossRef]
- Bhol, N.K.; Bhanjadeo, M.M.; Singh, A.K.; Dash, U.C.; Ojha, R.R.; Majhi, S.; Duttaroy, A.K.; Jena, A.B. The Interplay between Cytokines, Inflammation, and Antioxidants: Mechanistic Insights and Therapeutic Potentials of Various Antioxidants and Anti-Cytokine Compounds. Biomed. Pharmacother. 2024, 178, 117177. [Google Scholar] [CrossRef]
- Nashtahosseini, Z.; Eslami, M.; Paraandavaji, E.; Haraj, A.; Dowlat, B.F.; Hosseinzadeh, E.; Oksenych, V.; Naderian, R. Cytokine Signaling in Diabetic Neuropathy: A Key Player in Peripheral Nerve Damage. Biomedicines 2025, 13, 589. [Google Scholar] [CrossRef]
- Duzhyy, D.E.; Voitenko, N.V.; Belan, P.V. Peripheral Inflammation Results in Increased Excitability of Capsaicin-Insensitive Nociceptive DRG Neurons Mediated by Upregulation of ASICs and Voltage-Gated Ion Channels. Front. Cell. Neurosci. 2021, 15, 723295. [Google Scholar] [CrossRef] [PubMed]
- Maingret, F.; Coste, B.; Padilla, F.; Clerc, N.; Crest, M.; Korogod, S.M.; Delmas, P. Inflammatory Mediators Increase Nav1.9 Current and Excitability in Nociceptors through a Coincident Detection Mechanism. J. Gen. Physiol. 2008, 131, 211–225. [Google Scholar] [CrossRef]
- Wu, J.; Hu, H.; Li, X. Spinal Neuron-Glial Crosstalk and Ion Channel Dysregulation in Diabetic Neuropathic Pain. Front. Immunol. 2025, 16, 1480534. [Google Scholar] [CrossRef]
- Ma, J.; Yu, H.; Liu, J.; Chen, Y.; Wang, Q.; Xiang, L. Metformin Attenuates Hyperalgesia and Allodynia in Rats with Painful Diabetic Neuropathy Induced by Streptozotocin. Eur. J. Pharmacol. 2015, 764, 599–606. [Google Scholar] [CrossRef]
- Liu, F.; You, F.; Yang, L.; Wang, S.; Xie, D. Metformin Improves Diabetic Neuropathy by Reducing Inflammation through Up-Regulating the Expression of MiR-146a and Suppressing Oxidative Stress. J. Diabetes Complicat. 2024, 38, 108737. [Google Scholar] [CrossRef] [PubMed]
- Haddad, M.; Eid, S.; Harb, F.; Massry, M.E.L.; Azar, S.; Sauleau, E.-A.; Eid, A.A. Activation of 20-HETE Synthase Triggers Oxidative Injury and Peripheral Nerve Damage in Type 2 Diabetic Mice. J. Pain 2022, 23, 1371–1388. [Google Scholar] [CrossRef] [PubMed]
- Abdelkader, N.F.; Elbaset, M.A.; Moustafa, P.E.; Ibrahim, S.M. Empagliflozin Mitigates Type 2 Diabetes-Associated Peripheral Neuropathy: A Glucose-Independent Effect through AMPK Signaling. Arch. Pharm. Res. 2022, 45, 475–493. [Google Scholar] [CrossRef]
- Lee, S.-O.; Kuthati, Y.; Huang, W.-H.; Wong, C.-S. Semaglutide Ameliorates Diabetic Neuropathic Pain by Inhibiting Neuroinflammation in the Spinal Cord. Cells 2024, 13, 1857. [Google Scholar] [CrossRef]
- Akbarian, R.; Chamanara, M.; Rashidian, A.; Abdollahi, A.; Ejtemaei Mehr, S.; Dehpour, A.R. Atorvastatin Prevents the Development of Diabetic Neuropathic Nociception by Possible Involvement of Nitrergic System. J. Appl. Biomed. 2021, 19, 48–56. [Google Scholar] [CrossRef]
- McIver, L.A.; Siddique, M.S. Atorvastatin; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Cui, N.; Feng, Y.; Wang, M.; Lu, X.; Huang, Y.; Chen, Y.; Shi, X. Protective Effect of Alirocumab, a PCSK9 Inhibitor, on the Sciatic Nerve of Rats with Diabetic Peripheral Neuropathy. Endocr. J. 2024, 71, EJ23–EJ0359. [Google Scholar] [CrossRef]
- Alirocumab: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB09302 (accessed on 18 June 2025).
- Pecikoza, U.; Tomić, M.; Nastić, K.; Micov, A.; Stepanović-Petrović, R. Synergism between Metformin and Analgesics/Vitamin B12 in a Model of Painful Diabetic Neuropathy. Biomed. Pharmacother. 2022, 153, 113441. [Google Scholar] [CrossRef]
- Duloxetine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00476 (accessed on 18 June 2025).
- Vitamin B12: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00115 (accessed on 18 June 2025).
- Alkhudhayri, S.; Sajini, R.; Alharbi, B.; Qabbani, J.; Al-Hindi, Y.; Fairaq, A.; Yousef, A. Investigating the Beneficial Effect of Aliskiren in Attenuating Neuropathic Pain in Diabetic Sprague-Dawley Rats. Endocrinol. Diabetes Metab. 2021, 4, e00209. [Google Scholar] [CrossRef] [PubMed]
- Gliclazide: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB01120 (accessed on 18 June 2025).
- Aliskiren: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB09026 (accessed on 18 June 2025).
- Elkholy, S.E.; Elaidy, S.M.; El-Sherbeeny, N.A.; Toraih, E.A.; El-Gawly, H.W. Neuroprotective Effects of Ranolazine versus Pioglitazone in Experimental Diabetic Neuropathy: Targeting Nav1.7 Channels and PPAR-γ. Life Sci. 2020, 250, 117557. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, Q.; Bai, Y.; Zheng, H.; Ji, L.; Zhu, X.; Sun, W.; Liu, X.; Zhang, S.; Li, Y.; et al. Glycogen Synthesis Kinase-3β Involves in the Analgesic Effect of Liraglutide on Diabetic Neuropathic Pain. J. Diabetes Complicat. 2023, 37, 108416. [Google Scholar] [CrossRef]
- Gateva, P.; Hristov, M.; Ivanova, N.; Vasileva, D.; Ivanova, A.; Sabit, Z.; Bogdanov, T.; Apostolova, S.; Tzoneva, R. Antinociceptive Behavior, Glutamine/Glutamate, and Neopterin in Early-Stage Streptozotocin-Induced Diabetic Neuropathy in Liraglutide-Treated Mice under a Standard or Enriched Environment. Int. J. Mol. Sci. 2024, 25, 10786. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Mizukami, H.; Osonoi, S.; Ogasawara, S.; Hara, Y.; Kudoh, K.; Takeuchi, Y.; Sasaki, T.; Daimon, M.; Yagihashi, S. Inhibitory Effects of Xanthine Oxidase Inhibitor, Topiroxostat, on Development of Neuropathy in Db/Db Mice. Neurobiol. Dis. 2021, 155, 105392. [Google Scholar] [CrossRef]
- Topiroxostat: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB01685 (accessed on 18 June 2025).
- Wei, Y.; Huang, Y.; Huang, R.; Ruan, Y.; Feng, T.; Zhou, F.; Zhang, W.; Lu, J.; Xie, S.; Yao, Y.; et al. Antihypertensive Drug Amlodipine Besylate Shows Potential in Alleviating Diabetic Peripheral Neuropathy. Diabetes 2025, 74, 983–997. [Google Scholar] [CrossRef]
- Amlodipine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00381 (accessed on 18 June 2025).
- Nayak, B.P.; Minaz, N.; Pasha, K. Molsidomine Ameliorates Diabetic Peripheral Neuropathy Complications in Wistar Rats. Anim. Model. Exp. Med. 2021, 4, 243–248. [Google Scholar] [CrossRef]
- Molsidomine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB09282 (accessed on 18 June 2025).
- Gölboyu, B.E.; Erdoğan, M.A.; Erbaş, O. Trimetazidine Provides Protection against Diabetic Polyneuropathy in Rats via Modulation of Soluble HMGB1. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 5854–5861. [Google Scholar] [CrossRef]
- Trimetazidine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB09069 (accessed on 30 January 2025).
- Xu, J.; Xu, X.; Ling, Y.; Wang, Y.; Huang, Y.; Yang, J.; Wang, J.; Shen, X. Vincamine as an Agonist of G-Protein-Coupled Receptor 40 Effectively Ameliorates Diabetic Peripheral Neuropathy in Mice. Acta Pharmacol. Sin. 2023, 44, 2388–2403. [Google Scholar] [CrossRef]
- Melatonin: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB01065 (accessed on 18 June 2025).
- Che, H.; Li, H.; Li, Y.; Wang, Y.; Yang, Z.; Wang, R.; Wang, L. Melatonin Exerts Neuroprotective Effects by Inhibiting Neuronal Pyroptosis and Autophagy in STZ-induced Diabetic Mice. FASEB J. 2020, 34, 14042–14054. [Google Scholar] [CrossRef]
- Ghazipour, A.M.; Pourheydar, B.; Naderi, R. The Effect of Tropisetron on Peripheral Diabetic Neuropathy: Possible Protective Actions against Inflammation and Apoptosis. Cell Stress Chaperones 2022, 27, 513–521. [Google Scholar] [CrossRef]
- Tropisetron: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB11699 (accessed on 18 June 2025).
- Topiramate: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00273 (accessed on 18 June 2025).
- Thakur, V.; Gonzalez, M.A.; Parada, M.; Martinez, R.D.; Chattopadhyay, M. Role of Histone Deacetylase Inhibitor in Diabetic Painful Neuropathy. Mol. Neurobiol. 2024, 61, 2283–2296. [Google Scholar] [CrossRef] [PubMed]
- Romidepsin: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB06176 (accessed on 18 June 2025).
- Salama, R.A.M.; Raafat, F.A.; Hasanin, A.H.; Hendawy, N.; Saleh, L.A.; Habib, E.K.; Hamza, M.; Hassan, A.N.E. A Neuroprotective Effect of Pentoxifylline in Rats with Diabetic Neuropathy: Mitigation of Inflammatory and Vascular Alterations. Int. Immunopharmacol. 2024, 128, 111533. [Google Scholar] [CrossRef] [PubMed]
- Pentoxifylline: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00806 (accessed on 18 June 2025).
- Eisa, N.H.; Helmy, S.A.; El-Kashef, D.H.; El-Sherbiny, M.; Elsherbiny, N.M. Pramipexole Protects against Diabetic Neuropathy: Effect on Oxidative Stress, TLR4/IRAK-1/TRAF-6/NF-ΚB and Downstream Inflammatory Mediators. Int. Immunopharmacol. 2024, 128, 111514. [Google Scholar] [CrossRef]
- Al-Rejaie, S.S.; Abuohashish, H.M.; Ahmed, M.M.; Arrejaie, A.S.; Aleisa, A.M.; AlSharari, S.D. Telmisartan Inhibits Hyperalgesia and Inflammatory Progression in a Diabetic Neuropathic Pain Model of Wistar Rats. Neurosci. J. 2015, 20, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Kolahdouz, M.; Jafari, F.; Falanji, F.; Nazemi, S.; Mohammadzadeh, M.; Molavi, M.; Amin, B. Clavulanic Acid Attenuating Effect on the Diabetic Neuropathic Pain in Rats. Neurochem. Res. 2021, 46, 1759–1770. [Google Scholar] [CrossRef]
- Clavulanic Acid: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00766 (accessed on 18 June 2025).
- Turan Yücel, N.; Can, Ö.D.; Demir Özkay, Ü. Catecholaminergic and Opioidergic System Mediated Effects of Reboxetine on Diabetic Neuropathic Pain. Psychopharmacology 2020, 237, 1131–1145. [Google Scholar] [CrossRef]
- Ismail, C.A.N.; Suppian, R.; Ab Aziz, C.B.; Long, I. Ifenprodil Reduced Expression of Activated Microglia, BDNF and DREAM Proteins in the Spinal Cord Following Formalin Injection During the Early Stage of Painful Diabetic Neuropathy in Rats. J. Mol. Neurosci. 2021, 71, 379–393. [Google Scholar] [CrossRef]
- Ifenprodil: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB08954 (accessed on 18 June 2025).
- Gazzo, G.; Salgado Ferrer, M.; Poisbeau, P. The Non-Benzodiazepine Anxiolytic Etifoxine Limits Mechanical Allodynia and Anxiety-like Symptoms in a Mouse Model of Streptozotocin-Induced Diabetic Neuropathy. PLoS ONE 2021, 16, e0248092. [Google Scholar] [CrossRef]
- Etifoxine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB08986 (accessed on 18 June 2025).
- Zhang, X.; Xia, L.; Xie, A.; Liao, O.; Ju, F.; Zhou, Y. Low Concentration of Bupivacaine Ameliorates Painful Diabetic Neuropathy by Mediating MiR-23a/PDE4B Axis in Microglia. Eur. J. Pharmacol. 2021, 891, 173719. [Google Scholar] [CrossRef] [PubMed]
- Bupivacaine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00297 (accessed on 18 June 2025).
- Dastgheib, M.; Shetab-Boushehri, S.V.; Baeeri, M.; Gholami, M.; Karimi, M.Y.; Hosseini, A. Rolipram and Pentoxifylline Combination Ameliorates Experimental Diabetic Neuropathy through Inhibition of Oxidative Stress and Inflammatory Pathways in the Dorsal Root Ganglion Neurons. Metab. Brain Dis. 2022, 37, 2615–2627. [Google Scholar] [CrossRef]
- Rolipram: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB01954 (accessed on 18 June 2025).
- Pușcașu, C.; Negreș, S.; Zbârcea, C.E.; Ungurianu, A.; Ștefănescu, E.; Blebea, N.M.; Chiriță, C. Evaluating the Antihyperalgesic Potential of Sildenafil–Metformin Combination and Its Impact on Biochemical Markers in Alloxan-Induced Diabetic Neuropathy in Rats. Pharmaceuticals 2024, 17, 783. [Google Scholar] [CrossRef] [PubMed]
- Sildenafil: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00203 (accessed on 18 June 2025).
- Pușcașu, C.; Ungurianu, A.; Șeremet, O.C.; Andrei, C.; Mihai, D.P.; Negreș, S. The Influence of Sildenafil–Metformin Combination on Hyperalgesia and Biochemical Markers in Diabetic Neuropathy in Mice. Medicina 2023, 59, 1375. [Google Scholar] [CrossRef]
- Alomar, S.Y.; El-Gheit, R.E.A.; Enan, E.T.; El-Bayoumi, K.S.; Shoaeir, M.Z.; Elkazaz, A.Y.; Al Thagfan, S.S.; Zaitone, S.A.; El-Sayed, R.M. Novel Mechanism for Memantine in Attenuating Diabetic Neuropathic Pain in Mice via Downregulating the Spinal HMGB1/TRL4/NF-KB Inflammatory Axis. Pharmaceuticals 2021, 14, 307. [Google Scholar] [CrossRef] [PubMed]
- Memantine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB01043 (accessed on 18 June 2025).
- Djouhri, L.; Malki, M.I.; Zeidan, A.; Nagi, K.; Smith, T. Activation of Kv7 Channels with the Anticonvulsant Retigabine Alleviates Neuropathic Pain Behaviour in the Streptozotocin Rat Model of Diabetic Neuropathy. J. Drug Target. 2019, 27, 1118–1126. [Google Scholar] [CrossRef]
- Ezogabine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB04953 (accessed on 18 June 2025).
- Tseng, K.-Y.; Wang, H.-C.; Wang, Y.-H.; Su, M.-P.; Cheng, K.-F.; Cheng, K.-I.; Chang, L.-L. Peripheral Nerve Denervation in Streptozotocin-Induced Diabetic Rats Is Reduced by Cilostazol. Medicina 2023, 59, 553. [Google Scholar] [CrossRef]
- Cilostazol: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB01166 (accessed on 18 June 2025).
- Notartomaso, S.; Scarselli, P.; Mascio, G.; Liberatore, F.; Mazzon, E.; Mammana, S.; Gugliandolo, A.; Cruccu, G.; Bruno, V.; Nicoletti, F.; et al. N-Acetylcysteine Causes Analgesia in a Mouse Model of Painful Diabetic Neuropathy. Mol. Pain 2020, 16, 1744806920904292. [Google Scholar] [CrossRef]
- Acetylcysteine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB06151 (accessed on 18 June 2025).
- Jolivalt, C.G.; Frizzi, K.E.; Han, M.M.; Mota, A.J.; Guernsey, L.S.; Kotra, L.P.; Fernyhough, P.; Calcutt, N.A. Topical Delivery of Muscarinic Receptor Antagonists Prevents and Reverses Peripheral Neuropathy in Female Diabetic Mice. J. Pharmacol. Exp. Ther. 2020, 374, 44–51. [Google Scholar] [CrossRef]
- Pirenzepine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00670 (accessed on 18 June 2025).
- Casselini, C.M.; Parson, H.K.; Frizzi, K.E.; Marquez, A.; Smith, D.R.; Guernsey, L.; Nemmani, R.; Tayarani, A.; Jolivalt, C.G.; Weaver, J.; et al. A Muscarinic Receptor Antagonist Reverses Multiple Indices of Diabetic Peripheral Neuropathy: Preclinical and Clinical Studies Using Oxybutynin. Acta Neuropathol. 2024, 147, 60. [Google Scholar] [CrossRef]
- Oxybutynin: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB01062 (accessed on 18 June 2025).
- Atropine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00572 (accessed on 18 June 2025).
- Xu, X.; Xu, X.; Hao, Y.; Zhu, X.; Lu, J.; Ouyang, X.; Lu, Y.; Huang, X.; Li, Y.; Wang, J.; et al. Antispasmodic Drug Drofenine as an Inhibitor of Kv2.1 Channel Ameliorates Peripheral Neuropathy in Diabetic Mice. iScience 2020, 23, 101617. [Google Scholar] [CrossRef] [PubMed]
- Santos, D.F.S.; Donahue, R.R.; Laird, D.E.; Oliveira, M.C.G.; Taylor, B.K. The PPARγ Agonist Pioglitazone Produces a Female-Predominant Inhibition of Hyperalgesia Associated with Surgical Incision, Peripheral Nerve Injury, and Painful Diabetic Neuropathy. Neuropharmacology 2022, 205, 108907. [Google Scholar] [CrossRef]
- Ozcan, S.; Bulmus, O.; Ulker, N.; Canpolat, S.; Etem, E.O.; Oruc, S.; Yardimci, A.; Bulmus, F.G.; Ayar, A.; Kelestimur, H.; et al. Agomelatine Potentiates Anti-Nociceptive Effects of Morphine in a Mice Model for Diabetic Neuropathy: Involvement of NMDA Receptor Subtype NR1 within the Raphe Nucleus and Periaqueductal Grey. Neurol. Res. 2020, 42, 554–563. [Google Scholar] [CrossRef]
- Agomelatine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB06594 (accessed on 18 June 2025).
- Morphine: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00295 (accessed on 18 June 2025).
- Magar, A.; Devasani, K.; Majumdar, A. Melatonin Ameliorates Neuropathy in Diabetic Rats by Abating Mitochondrial Dysfunction and Metabolic Derangements. Endocr. Metab. Sci. 2020, 1, 100067. [Google Scholar] [CrossRef]
- Gabapentin: Uses, Interactions, Mechanism of Action|DrugBank Online. Available online: https://go.drugbank.com/drugs/DB00996 (accessed on 18 June 2025).
- Brock, C.; Hansen, C.S.; Karmisholt, J.; Møller, H.J.; Juhl, A.; Farmer, A.D.; Drewes, A.M.; Riahi, S.; Lervang, H.H.; Jakobsen, P.E.; et al. Liraglutide Treatment Reduced Interleukin-6 in Adults with Type 1 Diabetes but Did Not Improve Established Autonomic or Polyneuropathy. Br. J. Clin. Pharmacol. 2019, 85, 2512–2523. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Robinson, M.; Wong, N.; Chan, E.; Charles, M.A. The Effect of Pentoxifylline on Current Perception Thresholds in Patients with Diabetic Sensory Neuropathy. J. Diabetes Complicat. 1997, 11, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Carroll, D.G.; Kline, K.M.; Malnar, K.F. Role of Topiramate for the Treatment of Painful Diabetic Peripheral Neuropathy. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2004, 24, 1186–1193. [Google Scholar] [CrossRef]
- Alexandre, K.; Sh, A.A.; Nikoloz, G.; Ketevan, C. Clinical and Pharmacological Basis for the Use of Telmisartan in Patients with Diabetic Neuropathy Diabetes & Its Complications. Patients Diabet. Neuropathy Diabetes Complicat. 2018, 2, 1–7. [Google Scholar]
- Alexandre, K.; Sh, A.A.; Nikoloz, G.; Ketevan, C. 1 of 6 Diabetes Complications. Diabetes Mellit. Patients Peripher. Neuropathy Diabetes Complicat. 2018, 2, 1–6. [Google Scholar]
- Rosales, R.L.; Delgado-Delos Santos, M.M.S.; Mercado-Asis, L.B. Cilostazol: A Pilot Study on Safety and Clinical Efficacy in Neuropathies of Diabetes Mellitus Type 2 (ASCEND). Angiology 2011, 62, 625–635. [Google Scholar] [CrossRef]
- Dhanapalaratnam, R.; Issar, T.; Wang, L.L.; Tran, D.; Poynten, A.M.; Milner, K.-L.; Kwai, N.C.G.; Krishnan, A.V. Effect of Metformin on Peripheral Nerve Morphology in Type 2 Diabetes: A Cross-Sectional Observational Study. Diabetes 2024, 73, 1875–1882. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Yu, H.; Wu, J.; Chen, H.; Wang, M.; Wang, S.; Qin, X.; Wu, T.; Wu, Y.; Hu, Y. Metformin Treatment and Risk of Diabetic Peripheral Neuropathy in Patients with Type 2 Diabetes Mellitus in Beijing, China. Front. Endocrinol. 2023, 14, 1082720. [Google Scholar] [CrossRef] [PubMed]
- El-Haggar, S.M.; Hafez, Y.M.; El Sharkawy, A.M.; Khalifa, M. Effect of Empagliflozin in Peripheral Diabetic Neuropathy of Patients with Type 2 Diabetes Mellitus. Med. Clínica 2024, 163, 53–61. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.Gov. Study Details A Research Study to Investigate the Effects of CagriSema Compared to Placebo in People with Type 2 Diabetes and Painful Diabetic Peripheral Neuropathy|ClinicalTrials.Gov. Available online: https://clinicaltrials.gov/study/NCT06797869 (accessed on 23 June 2025).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).