Abstract
Introduction: Gingival recession, characterized by the apical displacement of the gingival margin, presents challenges to oral health. This study compares the effectiveness of the coronally advanced flap (CAF) and the tunnel technique (TT) for treating gingival recessions. Methods: Bibliographical searches included PubMed, Embase, Web of Science, Cochrane, Scopus, and the grey literature, with keywords “root coverage” “coronary advanced flap”, and “tunnel”. A systematic coreview was performed that included 26 studies evaluating root coverage, and 14 articles were included for the meta-analysis. Three groups were analyzed: Group 1 compared TT with connective tissue graft (CTG) versus CAF with CTG; Group 2 examined TT with CTG and/or other biomaterials versus TT with CTG alone; Group 3 compared TT with CAF, regardless of complementary biomaterials. Meta-analysis assessed mean root coverage (MRC), complete root coverage (CRC), and keratinized tissue gain (KTG). Results: In Group 1, TT with CTG demonstrated superior MRC compared with CAF with CTG (−8.68 CI95% −17.19 to −0.17; p = 0.0457). In Group 2, TT with CTG and/or other biomaterials showed similar MRC (4.17 CI95% −17.91 to 26.26; p = 0.7110) and CRC (0.37 CI95% −1.14 to 1.89; p = 0.6269) to TT with CTG alone, with variations in keratinized tissue gain. Group 3 indicated higher potential MRC for TT compared with CAF (5.73 CI95% −8.90 to 13.55; p = 0.685) but without statistically significant differences. Conclusions: This study suggests that TT with CTG might offer better root coverage than CAF with CTG; however, biomaterial selection requires consideration.
1. Introduction
Gingival recession (GR) is defined as the displacement of the gingival margin apical to the cementum–enamel junction (CEJ) of a tooth or dental implant abutment [1,2]. This condition is of great importance in oral health as it can compromise not only dental esthetics but also overall periodontal health [3]. Recent surveys revealed that 88% of people aged 65 and older and 50% of people aged 18 to 64 have one or more recession sites [4]. The highest prevalence of gingival recessions varies between 58% and 99.7% in epidemiological studies [5]. Gingival recessions can be caused by several factors, including inadequate oral hygiene, gingivitis, periodontal diseases, dental caries, trauma, or unsuccessful restorations [6,7]. Gingival recession leads to dental hypersensitivity, and increased risk of root caries and plaque accumulation, and can be linked to minimal or no presence of keratinized tissue [8]. Root coverage surgery aims to achieve a comprehensive esthetic outcome rather than solely complete root coverage [9]. A systematic review demonstrated that connective tissue grafts (CTGs) or enamel matrix derivates (EMDs) increase the likelihood of obtaining complete root coverage in single gingival recessions Miller Class I and II [10]. Class I involves recession that stays above the mucogingival line, while Class II extends beyond it but without affecting the bone or interdental soft tissues. In Class III, the recession also extends beyond the mucogingival junction, but with partial loss of interdental bone or soft tissue, which may limit the potential for full root coverage (Figure 1).

Figure 1.
(A) Miller Class I (RT1), (B) Miller Class II (RT2), (C) Miller Class III (RT3).
Periodontal plastic surgery aims to maintain an adequate mucogingival complex, emphasizing the importance of the amount and position of the attached gingiva [11]. Currently, different surgical procedures have been proposed to maintain the papilla’s integrity when complete root coverage or regenerative therapy is needed, the most representative being the coronally advanced flap (CAF) and the tunnelling technique (TT) [12]. Connective tissue has proven to be the gold standard in root-coverage treatments [13]. Recent studies have shown that connective tissue + EMD has a favorable impact on the healing and regeneration process of periodontal wounds, manifesting through the generation of the periodontal ligament, root cementum, and, to some extent, alveolar bone [14]. Bajishov et al., in 2021, concluded that the depth of recession, amount of keratinized gingiva, and gingival thickness were significant predictors of complete or partial root coverage [15]. TT is a conservative technique that improves esthetic results [16]. Another advantage of this TT is the large blood supply and nutrition of the graft, and the healing period is faster than in a CAF, with less postoperative morbidity due to the limited opening of the flap [17]. A systematic review and meta-analysis demonstrated that TT is effective in treatments of localized and multiple gingival recessions, with a mean root coverage (MRC) of 82.75 ± 19.7% and 87.87 ± 16.45%, respectively [18]. On the other hand, the vestibular incision subperiosteal tunnel access (VISTA) technique achieved an MRC of 88.15 ± 20.79% and a cRC of 67.85 ± 21.72%, which was significantly higher compared with the tunnel technique [19]. Additionally, the application of the tunnel technique with coronally advanced flap (TCAF) and connective tissue graft (CTG) resulted in improvements in clinical, esthetic outcomes, and patient perception in gingival recessions classified as Miller Type II (RT2) with papillary deficiency [20]. In recent years, the use of leucocyte and platelet-rich fibrin (L-PRF) has gained attention in this area. A systematic review with meta-analysis demonstrated that combining L-PRF with CAF significantly improved CRC compared with CAF alone; however, in cases of limited basal keratinized mucosa width, the use of CTG may be preferable [21]. Furthermore, another systematic review from 2022 concluded that L-PRF could be an appropriate substitute for increasing keratinized mucosa around implants [22].
The aim of the study was to analyze whether root coverage is more effective with TT compared with CAF.
2. Materials and Methods
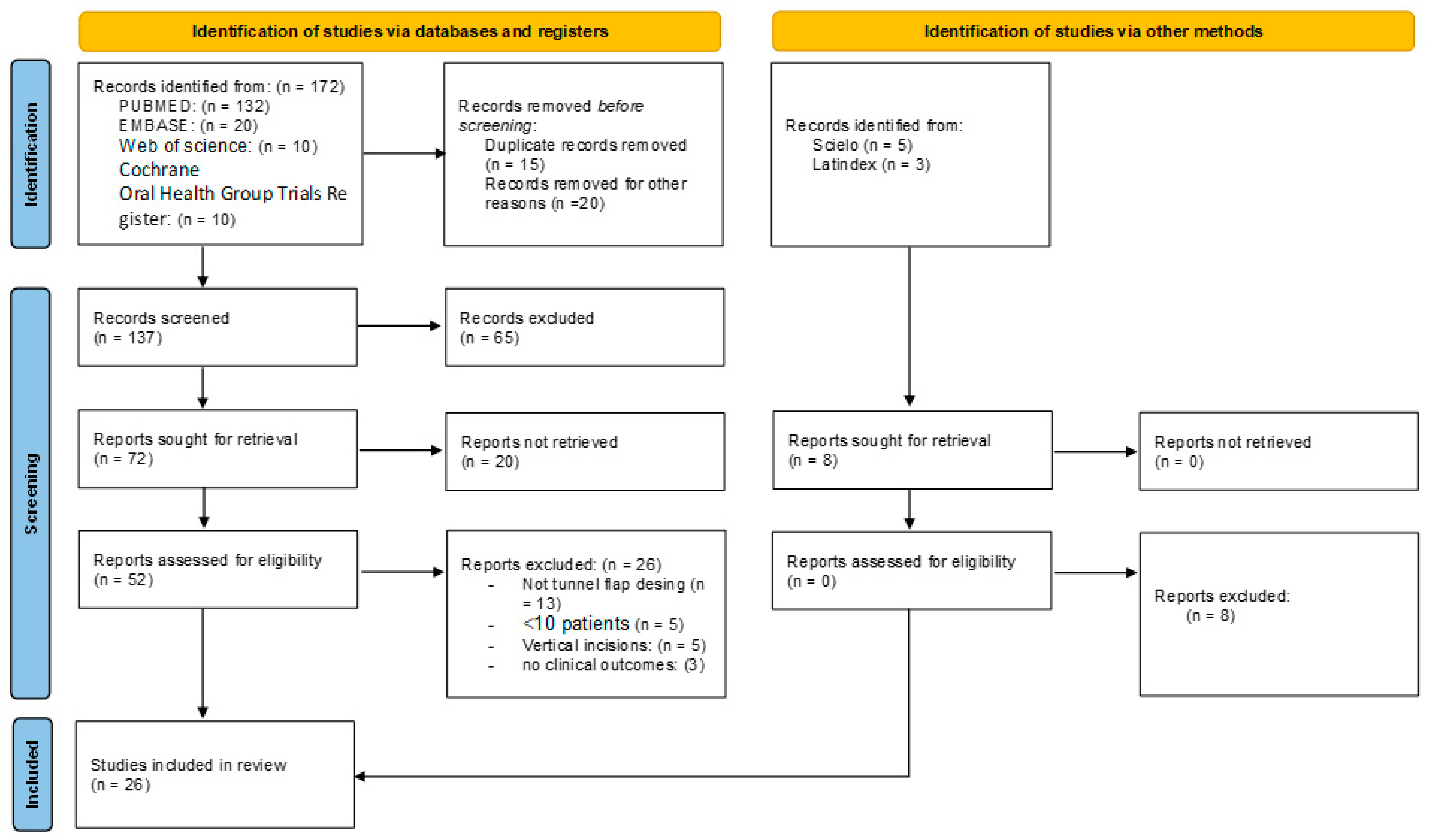
A specific protocol was designed for the search and restore procedures complying with the PRISMA guidelines [23] (Figure 2). The PICO question was as follows: is root covering more effective with TT compared with CAF? P—patients with Miller Type I, II, and III gingival recession; RT1, RT2, or RT3 [24] single or multiple. I—intervention of all gingival recessions treated with TT. C—comparison of TT and CAF. O—evaluation of root coverage. The protocol was registered in PROSPERO with reference ID: CRD42023425664.
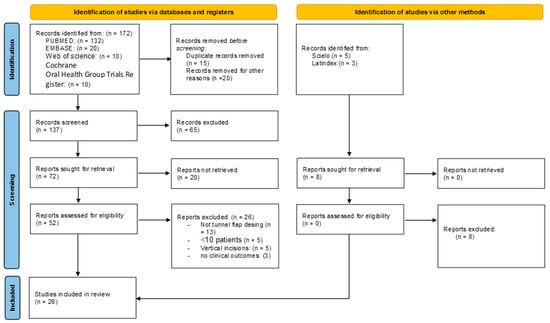
Figure 2.
Flowchart of selected studies.
2.1. Search Strategy and Database Screening
A bibliographic search was performed by LCB and BVR covering the last 10 years, (upper limit: December 2022) in various databases, including PubMed, Embase, Web of Science, Cochrane, Scopus, and the grey literature. In addition, relevant journals, such as the Journal of Periodontology, were reviewed.
Searches combined thesaurus and free terms to maximize sensitivity. The algorithm “Root coverage” AND (“coronary advanced flap” OR “tunnel”) was adapted for syntax in each database. Duplicated articles were manually removed after EndNote reference software import and automatic duplicate removal (Endnote X9.3.2, Clarivate Analytics, Philadelphia, PA, USA).
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
All references identified from computerized databases were manually retrieved (by LCB and BVR) and articles were included if they satisfied the following criteria: (1) evaluation of root coverage; (2) randomized clinical trial; (3) case–control studies involving at least 10 patients with single or multiple gingival recessions; (4) studies published within the last 10 years; (5) minimum study follow-up of 6 and 12 months.
2.2.2. Exclusion Criteria
(1) If the TT involved vertical incisions or incisions in the papillae; (2) if the research had fewer than 10 patients; (3) if there was no coronally advanced flap; (4) case reports.
2.3. Study Selection and Data Extraction Process
Data were retrieved by three investigators (LCB, APJ, and MPS) using a custom-made extraction sheet. Disagreements between researchers were resolved by a third researcher (BVR) blinded to the study hypothesis.
During the search, titles and abstracts of all possible records were reviewed and the inclusion of any text with insufficient data was discussed using a full-text protocol. All eligible articles were then reviewed and, if important data were missing for the current systematic review and meta-analysis, attempts were made to contact the corresponding author of the study to address or clarify any concerns.
Data were extracted (by LCB, APJ, and MPS) regarding author, year of publication, country, study design, periodontal status and habits, type and location of recession, type of surgical technique, use of connective tissue or other biomaterials with full description, number of patients, number of recessions, follow-up in months, and outcome variables, e.g., mean root coverage (MRC), complete root coverage (CRC), keratinized tissue gain (KTG), and root coverage esthetic score (RCES).
2.4. Quality and Risk of Bias Assessment
Risk of bias was measured using the Cochrane risk of bias tool (ECA) [25] for the assessment of randomized controlled trials.
2.5. Statistical Analysis
Pooled weighted mean differences (WMDs) and standard deviations (SDs) were calculated. The contribution of each study was weighted accordingly, and the random effects model was selected, as heterogeneity between studies was assumed. Forest plots were produced to summarize the differences in both groups. For the statistical analysis of heterogeneity, the parameters of Cochran’s Q test (χ2) and Higgins I2 were calculated. Cochran’s Q test p < 0.1 was considered significant to assume apparent heterogeneity. The I2 index was used to quantify the percentage of heterogeneity, with values of 25, 50, and 75% considered to indicate low, moderate, and high heterogeneity, respectively [26]. Publication bias was assessed visually using funnel plots and also using the test proposed by Egger et al. [27] (where pEgger < 0.1 was considered significant). The R Metafor software package (v.4.2.1; https://www.r-project.org, accessed on 15 June 2023) was used for all statistical analyses. The significance level was set at p < 0.05.
3. Results
3.1. Study Selection
The searches, following PRISMA guidelines, can be seen in Figure 1. A total of 172 articles were identified, of which 145 articles were excluded. Finally, 26 articles were included for qualitative analysis, and 14 for quantitative analysis. The reviewers’ agreement by k-agreement score was 0.91, considered almost perfect according to the scale classification.
3.2. Study Characteristics
Of the 26 articles included, 69% were randomized controlled trials [15,16,17,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42] and 31% were case series [43,44,45,46,47,48,49,50]. Most of them were conducted in Europe [17,29,31,32,33,34,35,38,40,42,43,45,46,47,48,49,50], followed by Asia [15,28,30,37,39,41]. The total number of patients in this study was 612, and the total number of recessions analyzed in this study was 1708. The main characteristics of the included studies are shown in Table 1.

Table 1.
General overview of the included studies.
3.3. Type of Intervention
The interventions were heterogeneous and included comparisons such as TT + CTG versus CAF + CTG [15,28], TT + acellular dermal matrix (ADM) [25], TT + CTG versus CAF + EMD [26], TT + CTG versus TT + xenogeneic collagen matrix (XCM) [16,30], and other combinations, as detailed in Table 2.
Table 2.
Overview of the intervention characteristics and outcomes.
3.4. Risk of Bias
The risk of bias was assessed using the Cochrane risk of bias tool. The majority of studies had a low or uncertain risk of bias in most areas, indicating a generally good methodological quality of the included studies, as shown in Table 3.
Table 3.
Cochrane risk of bias of systematic reviews of interventions.
3.5. Meta-Analysis
Subgroup analysis was conducted due to the variability of interventions. Three comparison groups were created: Group 1: TT with CTG vs. CAF with CTG; Group 2: TT with CTG and other biomaterials vs. TT with CTG; Group 3: TT vs. CAF regardless of the type of biomaterial. The extracted results from the meta-analysis and the degree of heterogeneity are shown in Table 4.
Table 4.
Meta-analysis results for the different study groups. SE—standard error. CI—confidence Interval.
3.5.1. Group 1: Tunnel Technique with Connective Tissue vs. Coronally Advanced Flap with Connective Tissue
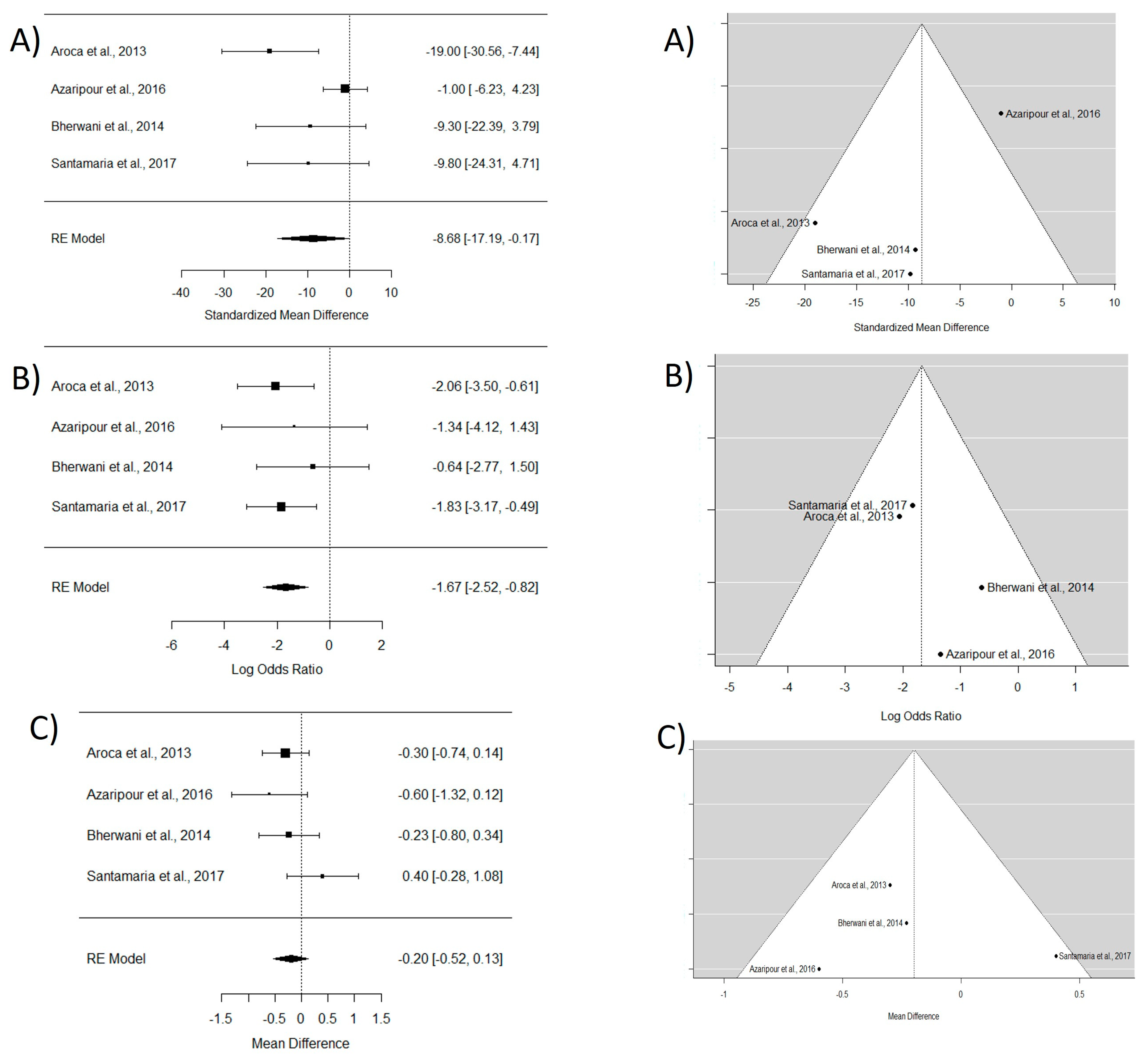
In the analysis of the four included articles [16,17,30,31], an 8.6 mm root coverage estimate (CI95% −17.19 to −0.17) in favor of CAF with CTG compared with TT with CTG was obtained. Regarding CRC, the WMD between CAF and TT was −1.67, indicating that CAF shows better outcomes than TT in terms of root coverage. No significant differences were found in terms of keratinized tissue gain between the two techniques (refer to Figure 3).
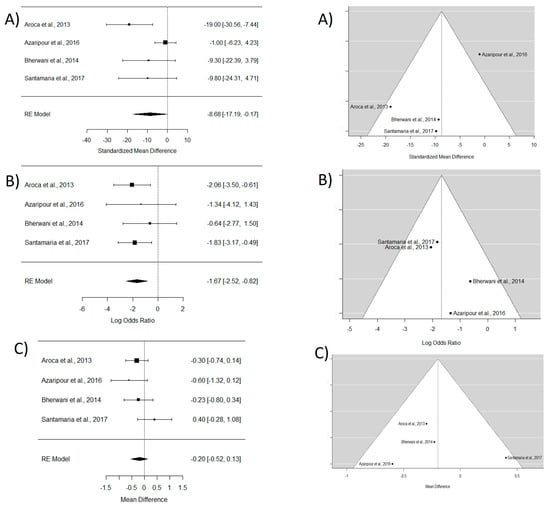
Figure 3.
Tunnel technique with connective tissue vs. coronally advanced flap with connective tissue. Forest plots (left column) and funnel plots (right column) for Group 1. (A) Keratinized tissue gain. (B) Mean root coverage. (C) Complete root coverage. [16,17,30,31].
3.5.2. Group 2: Tunnel Technique with Connective and/or Other Materials vs. Tunnel Technique with Connective
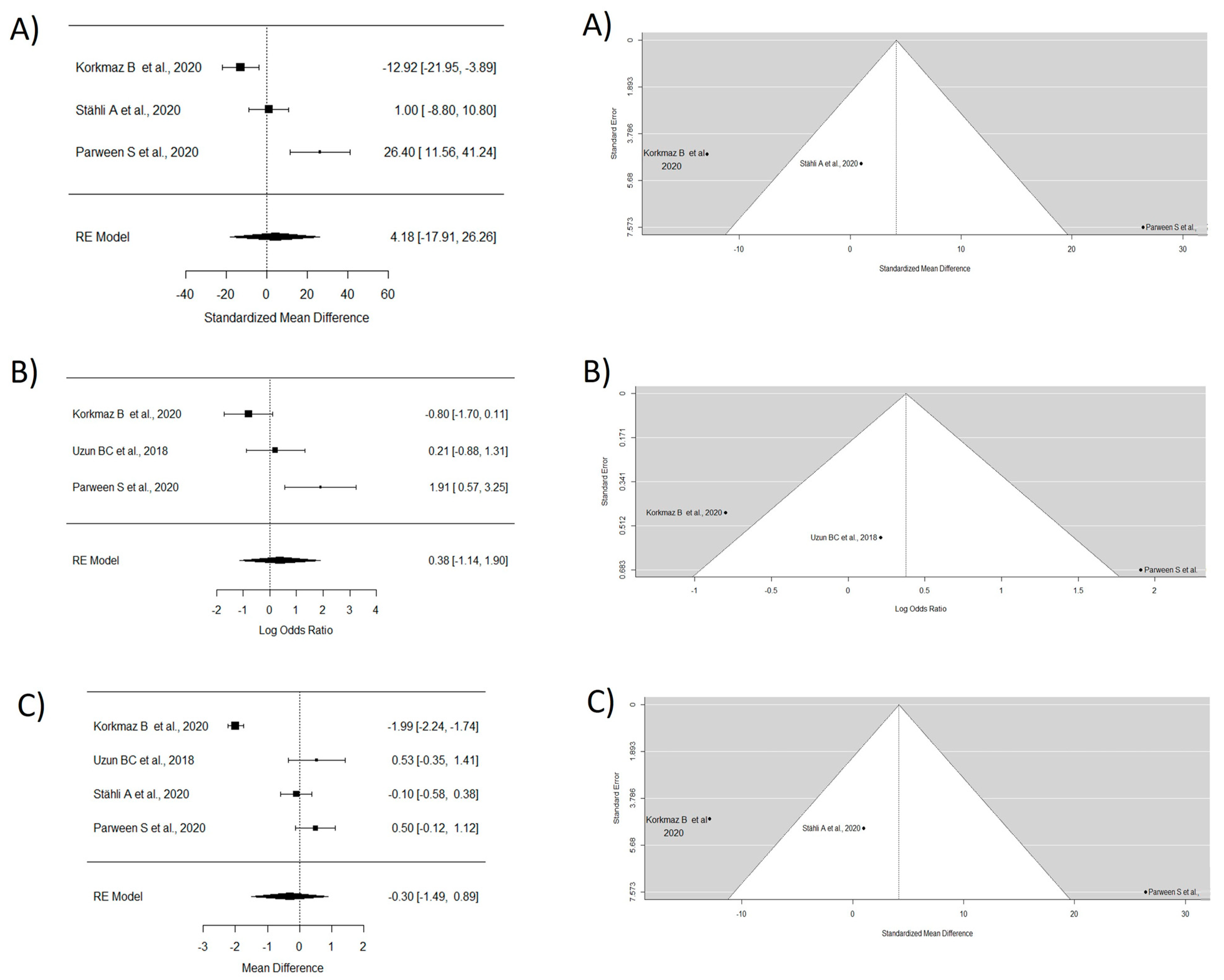
Four articles were analyzed in this group [37,39,40,41]. The MRC study did not incorporate the research carried out by Uzun et al. [39] due to insufficient data. The WMD of 4.17 demonstrated superior outcomes with the usage of CTG combined with other materials in contrast to CTG alone. However, no significant differences were observed. The study by Stähli A et al. [40] was not considered for CRC analysis due to the lack of data, and a WMD of 0.37 in favor of TT with CTG and/or other materials was observed, though without significant differences. For keratinized tissue gain, the random effects model showed a WMD of −0.30, indicating a greater keratinized tissue gain with CTG exclusively, though without significant differences between groups and with high heterogeneity (Figure 4).
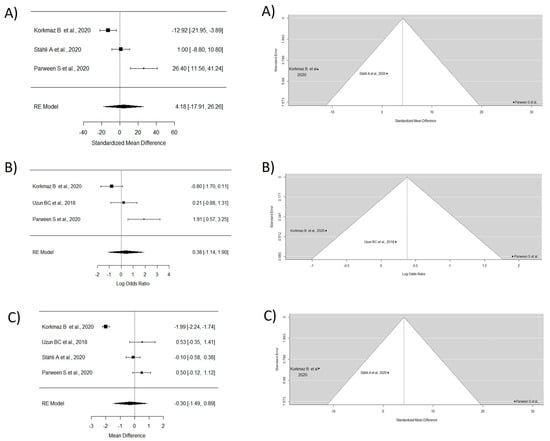
Figure 4.
Tunnel technique with connective and or other materials vs. tunnel technique with connective. Forest plots (left column) and funnel plots (right column) for Group 2. (A) Keratinized tissue gain. (B) Mean root coverage. (C) Complete root coverage [37,39,40,41].
3.5.3. Group 3: Tunnel Technique vs. Coronal Flap (Without Considering the Coadjutant Material Used)
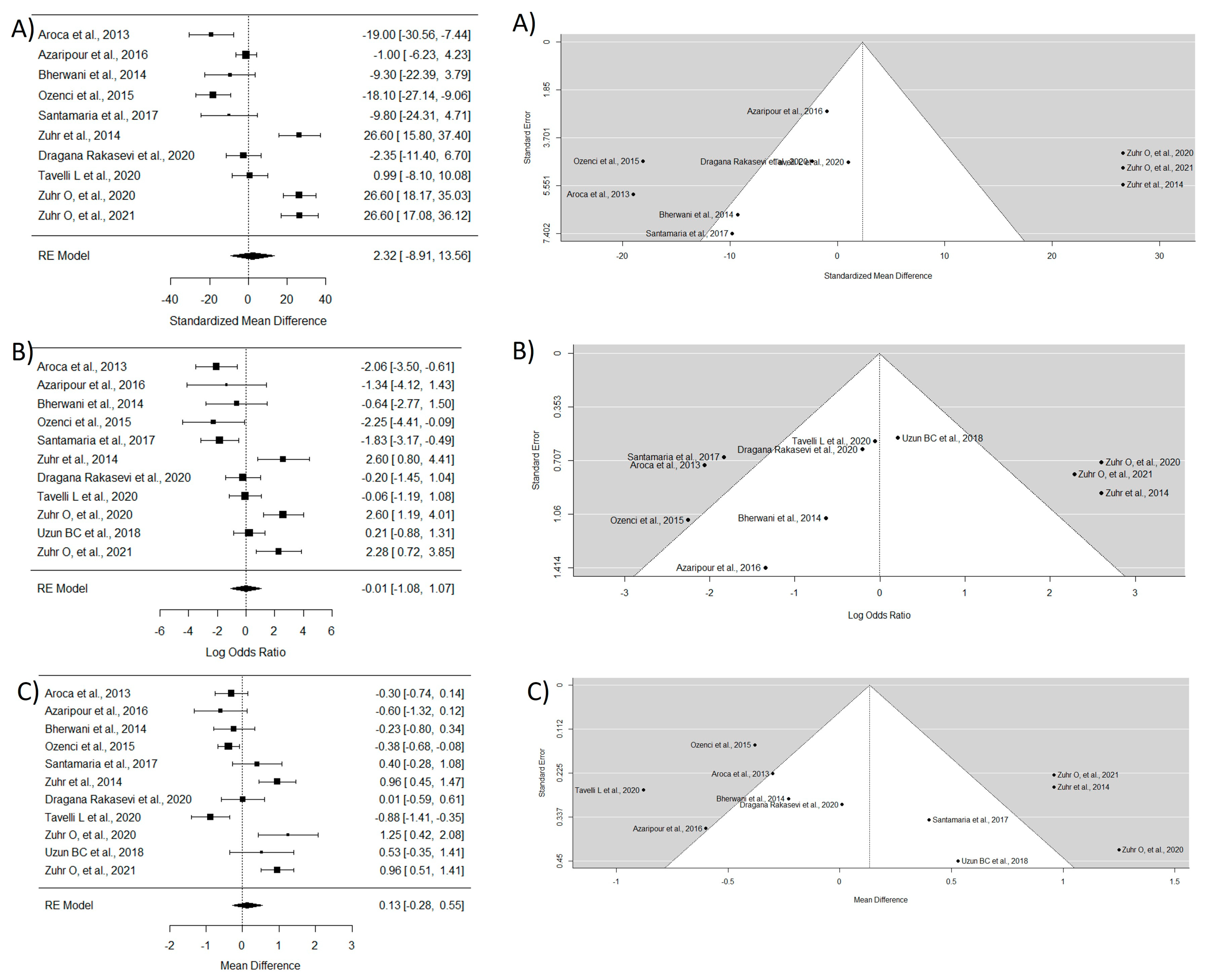
This group included 11 essays [16,17,28,29,30,31,34,37,38,39,42]. To study MRC, the study by Uzun BC et al. [39] was excluded due to the lack of necessary data. The WMD between groups was 2.32, indicating that TT has a greater ability for root coverage, though without statistically significant differences and with very high heterogeneity. The WMD for CRC was −0.006, indicating that there is not a large difference in the ability of both techniques to achieve complete coverage of the exposed root. Regarding KTG, a significantly greater mean difference was observed in the CAF technique compared with TT (WMD = 0.13) (Figure 5).
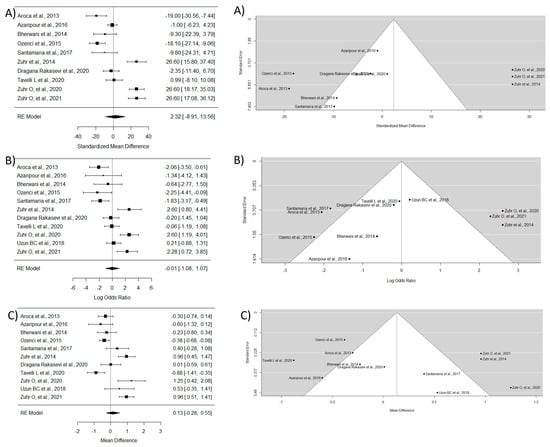
Figure 5.
Tunnel technique vs. coronal flap without considering the coadjutant material used. Forest plots (left column) and funnel plots (right column) for Group 3. (A) Keratinized tissue gain. (B) Mean root coverage. (C) Complete root coverage [16,17,28,29,30,31,34,37,38,39,42].
4. Discussion
The results of this systematic review and meta-analysis provide information on the comparative efficacy of TT and CAF techniques in achieving root coverage. Regarding mean root coverage, the analysis revealed that the CAF technique with CTG showed better results compared with the TT technique with CTG. This result is consistent with prior research that has demonstrated better outcomes with the CAF method for root coverage [16,20,30]. This difference between methods could be related to operator experience (especially with TT) and it is also important to note that the mean difference in CRM, although statistically significant, may not be clinically relevant.
Two systematic reviews and meta-analyses were examined, including one conducted by Tavelli et al. [20]. Tavelli et al. concluded that the tunnel technique was more effective in root coverage, achieving an MRC of 82.8% for localized recessions and 87.9% for multiple recessions. However, CAF yielded a higher CRC compared with TT when using CTG or an acellular dermal matrix in both techniques. Meanwhile, Tovalino et al., in 2023, [51] found that TT and CAF had similar primary and secondary outcomes. This aligns with the findings of Azaripour et al., Tavelli et al., and Zuhr et al. [31,36,38], suggesting that both techniques are equally effective in achieving complete root coverage. The minimal difference in CRC could be attributed to the gold standard nature of CTG in root coverage procedures. Therefore, while CAF may exhibit slightly better CRC, the advantages of TT, such as improved esthetics and faster healing, make it a viable alternative [16,17,29].
In terms of KTG, the analysis indicated that the CAF technique resulted in higher values compared with TT. This result is in line with previous studies that have emphasized the importance of KTG in improving periodontal health and esthetics [20,28]. However, Rebele et al. found that the TT technique resulted in thicker gingiva according to digital measurements. It is important to mention that, although statistically significant, the clinical significance of the difference in KTG could vary according to the individual needs of patients and clinical situations.
Studies like Santamaria et al. [16] described that the average percentage of MCR was significantly higher in the CAF + CTG group (87.2 ± 27.1%) compared with the TT + CTG group (77.4 ± 20.4%; p = 0.02), and CRC was highest in the CAF + CTG group (71.4%) in contrast with the TT + CTG group (28.6%; p = 0.01). In another study by Azaripour et al. [31], it was determined that mCR was 98.3 ± 9.3% in CAF + CTG and 97.2 ± 9.8% in MMTT + CTG, and CRC was 96% in CAF + CTG and 90.5% in MMTT + CTG, concluding that there were no significant differences in both techniques.
Other materials have been used for root coverage, as demonstrated by the study of Dragana Rakasevic et al. [34], which obtained an MCR of 85.25 ± 14.9 in the TT + XCM (xenogeneic collagen matrix) group and 87.6 ± 15.1 in the CAF + CTG group, and CRC was 46.8% in TT + XCM and 51.9% in CAF + CTG, yielding similar results in both techniques. Another study [28] utilized an acellular dermal matrix (ADM), which obtained an MRC of 75.72 ± 6.54 in the TT + ADM group, while it was 93.81 ± 13.10 in the CAF + ADM group, and CRC was 37.36 ± 21.10 in TT + ADM and 85.00 ± 33.75 in CAF + ADM, concluding that both TT + ADM and CAF + ADM proved to be effective in root coverage of multiple recessions. In a related study, Tavelli L et al. [36] found an MRC of 89.13 ± 15.19 in TT + ADM and 88.14 ± 16.91 in CAF + ADM, and a CRC of 51.2% in TT + ADM and 52.6% in CAF + ADM, concluding that there were no significant differences.
Meanwhile, Zuhr O et al. [42], using enamel matrix derivatives (EMDs), demonstrated that the MRC in the TT + CTG group was 98.4 ± 3.6% and in the CAF + EMD group was 71.8 ± 20.3%, while the CRC in the TT + CTG group was 82.2% and in CAF + EMD was 32%, determining that TT + CTG showed significantly superior long-term results compared with CAF + EMD in terms of CRC and MRC.
The results of this study provide valuable information for clinicians when selecting the appropriate surgical technique for root coverage procedures. Although the CAF technique with CTG may yield slightly superior results in MRC and KTG, TT offers several advantages that contribute to its clinical relevance. TT is associated with better esthetics due to its conservative nature, preserving the interdental papilla and avoiding vertical incisions [17,29]. In addition, TT has a shorter healing period and lower postoperative morbidity due to limited flap opening [36]. Therefore, the choice between both techniques should consider factors such as patient preferences, esthetic requirements, and clinician experience.
This study has some limitations that need to be acknowledged. First, the main surgical techniques (CAF and TT) were complemented with various regeneration materials (as described in Section 2), which means that heterogeneity in terms of materials used for root coverage and study designs could have introduced biases in the results, making overall conclusions complex due to the diversity of materials used. Second, the studies included in the analysis had non-uniform follow-up periods, leading to variability in the assessment of results. Additionally, the reported results may have been influenced by different definitions of success and the use of different measurement methods in different studies. Future research should aim to standardize outcome measurements, follow-up periods, and patient characteristics to enable more precise comparisons between techniques. Long-term studies with larger sample sizes are also needed to provide a comprehensive understanding of the durability and stability of root coverage achieved with both TT and CAF. Furthermore, investigating patient-reported outcomes, including esthetic satisfaction and patient discomfort, may enhance the comprehensive evaluation of the clinical effectiveness of each method.
5. Conclusions
In conclusion, this systematic review and this meta-analysis contribute to the understanding of root coverage techniques in the treatment of gingival recessions. The results suggest that both the tunnel technique and coronally advanced flap technique with connective tissue graft are effective in achieving root coverage. While the CAF technique may offer slightly better mean root coverage and keratinized tissue gain, the tunnel technique provides advantages in terms of esthetics, healing period, and patient comfort. The choice between the two techniques should be based on patient preferences, clinical considerations and clinical skills by the operator, and mastery of both techniques. Further research is needed to address the limitations and provide a more comprehensive assessment of these techniques.
Author Contributions
Conceptualization, A.P.-J., L.C.-B. and M.P.-S.; methodology, F.F.V.E.S., E.P.-I. and A.P.-J.; software, M.P.-S. and M.C.-A.; validation, F.F.V.E.S., L.C.-B., A.P.-J. and B.V.-R.; resources, A.P.-J., F.F.V.E.S., L.C.-B. and E.P.-I.; writing—original draft preparation, F.F.V.E.S., M.C.-A., A.P.-J. and L.C.-B.; writing—review and editing, A.P.-J., F.F.V.E.S., E.P.-I. and M.P.-S.; visualization, L.C.-B., B.V.-R., F.F.V.E.S. and M.C.-A.; supervision, F.F.V.E.S. and M.P.-S.; project administration, L.C.-B., F.F.V.E.S., A.P.-J. and M.P.-S. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Dataset available on request from the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Imber, J.; Kasaj, A. Treatment of Gingival Recession: When and How? Int. Dent. J. 2021, 71, 178–187. [Google Scholar] [CrossRef]
- Pini Prato, G. Mucogingival deformities. Ann. Periodontol. 1999, 4, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Niemczyk, W.; Niemczyk, S.; Prokurat, M.; Grudnik, K.; Migas, M.; Wągrowska, K.; Lau, K.; Kasperczyk, J. Etiology of gingival recession-a literature review. Wiad. Lek. 2024, 77, 1080–1085. [Google Scholar] [CrossRef] [PubMed]
- Kassab, M.M.; Cohen, R.E. The etiology and prevalence of gingival recession. J. Am. Dent. Assoc. 2003, 134, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Vignoletti, F.; Di Martino, M.; Clementini, M.; Di Domenico, G.L.; de Sanctis, M. Prevalence and risk indicators of gingival recessions in an Italian school of dentistry and dental hygiene: A cross-sectional study. Clin. Oral. Investig. 2020, 24, 991–1000. [Google Scholar] [CrossRef] [PubMed]
- Heasman, P.A.; Ritchie, M.; Asuni, A.; Gavillet, E.; Simonsen, J.L.; Nyvad, B. Gingival recession and root caries in the ageing population: A critical evaluation of treatments. J. Clin. Periodontol. 2017, 44 (Suppl. S18), S178–S193. [Google Scholar] [CrossRef]
- Guttiganur, N.; Aspalli, S.; Sanikop, M.V.; Desai, A.; Gaddale, R.; Devanoorkar, A. Classification systems for gingival recession and suggestion of a new classification system. Indian J. Dent. Res. 2018, 29, 233–237. [Google Scholar] [CrossRef]
- Zucchelli, G.; Mounssif, I. Periodontal plastic surgery. Periodontology 2000 2015, 68, 333–368. [Google Scholar] [CrossRef]
- Cairo, F.; Rotundo, R.; Miller, P.D.; Pini Prato, G.P. Root coverage esthetic score: A system to evaluate the esthetic outcome of the treatment of gingival recession through evaluation of clinical cases. J. Periodontol. 2009, 80, 705–710. [Google Scholar] [CrossRef]
- Cairo, F.; Pagliaro, U.; Nieri, M. Treatment of gingival recession with coronally advanced flap procedures: A systematic review. J. Clin. Periodontol. 2008, 35 (Suppl. S8), 136–162. [Google Scholar] [CrossRef]
- Pini Prato, G.P.; De Sanctis, M. Soft-tissue plastic surgery. Curr. Opin. Dent. 1991, 1, 98–103. [Google Scholar] [PubMed]
- Aslan, S.; Buduneli, N.; Cortellini, P. Entire papilla preservation technique in the regenerative treatment of deep intrabony defects: 1-Year results. J. Clin. Periodontol. 2017, 44, 926–932. [Google Scholar] [CrossRef]
- Park, H.C.; Kim, S.G.; Oh, J.S.; You, J.S.; Kim, J.S.; Lim, S.C.; Jeong, M.A.; Kim, J.S.; Jung, C.; Kwon, Y.S.; et al. Early Bone Formation at a Femur Defect Using CGF and PRF Grafts in Adult Dogs: A Comparative Study. Implant Dent. 2016, 25, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Shirakata, Y.; Nakamura, T.; Shinohara, Y.; Nakamura-Hasegawa, K.; Hashiguchi, C.; Takeuchi, N.; Imafuji, T.; Sculean, A.; Noguchi, K. Split-mouth evaluation of connective tissue graft with or without enamel matrix derivative for the treatment of isolated gingival recession defects in dogs. Clin. Oral Investig. 2019, 23, 3339–3349. [Google Scholar] [CrossRef]
- Bakhishov, H.; Isler, S.C.; Bozyel, B.; Yıldırım, B.; Tekindal, M.A.; Ozdemir, B. De-epithelialized gingival graft versus subepithelial connective tissue graft in the treatment of multiple adjacent gingival recessions using the tunnel technique: 1-year results of a randomized clinical trial. J. Clin. Periodontol. 2021, 48, 970–983. [Google Scholar] [CrossRef]
- Santamaria, M.P.; Neves, F.L.d.S.; Silveira, C.A.; Mathias, I.F.; Fernandes-Dias, S.B.; Jardini, M.A.N.; Tatakis, D.N. Connective tissue graft and tunnel or trapezoidal flap for the treatment of single maxillary gingival recessions: A randomized clinical trial. J. Clin. Periodontol. 2017, 44, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Aroca, S.; Molnár, B.; Windisch, P.; Gera, I.; Salvi, G.E.; Nikolidakis, D.; Sculean, A. Treatment of multiple adjacent Miller class I and II gingival recessions with a Modified Coronally Advanced Tunnel (MCAT) technique and a collagen matrix or palatal connective tissue graft: A randomized, controlled clinical trial. J. Clin. Periodontol. 2013, 40, 713–720. [Google Scholar] [CrossRef]
- Tavelli, L.; Barootchi, S.; Nguyen, T.V.N.; Tattan, M.; Ravidà, A.; Wang, H. Efficacy of tunnel technique in the treatment of localized and multiple gingival recessions: A systematic review and meta-analysis. J. Periodontol. 2018, 89, 1075–1090. [Google Scholar] [CrossRef]
- Sabri, H.; SamavatiJame, F.; Sarkarat, F.; Wang, H.L.; Zadeh, H.H. Clinical efficacy of Vestibular Incision Subperiosteal Tunnel Access (VISTA) for treatment of multiple gingival recession defects: A systematic review, meta-analysis and meta-regression. Clin. Oral Investig. 2023, 27, 7171–7187. [Google Scholar] [CrossRef]
- Barootchi, S.; Tavelli, L. Tunneled coronally advanced flap for the treatment of isolated gingival recessions with deficient papilla. Int. J. Esthet. Dent. 2022, 17, 14–26. [Google Scholar]
- Miron, R.J.; Moraschini, V.; Del Fabbro, M.; Piattelli, A.; Fujioka-Kobayashi, M.; Zhang, Y.; Saulacic, N.; Schaller, B.; Kawase, T.; Cosgarea, R.; et al. Use of platelet-rich fibrin for the treatment of gingival recessions: A systematic review and meta-analysis. Clin. Oral Investig. 2020, 24, 2543–2557. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, S.; Grieco, M.; Valentini, G.; Sorana, A.S.; Dolci, M. Increasing the width of the keratinized mucosa around implants with L-PRF: Report of a case and systematic review. Oral Implantol. 2023, 15, 44–52. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; A Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Nieri, M.; Cincinelli, S.; Mervelt, J.; Pagliaro, U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: An explorative and reliability study. J. Clin. Periodontol. 2011, 38, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomized trials. BMJ. 2011, 343, d5928. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Ozenci, I.; Ipci, S.D.; Cakar, G.; Yilmaz, S. Tunnel technique versus coronally advanced flap with acellular dermal matrix graft in the treatment of multiple gingival recessions. J. Clin. Periodontol. 2015, 42, 1135–1142. [Google Scholar] [CrossRef]
- Rebele, S.F.; Zuhr, O.; Schneider, D.; Jung, R.E.; Hürzeler, M.B. Tunnel technique with connective tissue graft versus coronally advanced flap with enamel matrix derivative for root coverage: A RCT using 3D digital measuring methods. Part II. Volumetric studies on healing dynamics and gingival dimensions. J. Clin. Periodontol. 2014, 41, 593–603. [Google Scholar] [CrossRef]
- Bherwani, C.; Kulloli, A.; Kathariya, R.; Shetty, S.; Agrawal, P.; Gujar, D.; Desai, A. Zucchelli’s technique or tunnel technique with subepithelial connective tissue graft for treatment of multiple gingival recessions. J. Int. Acad. Periodontol. 2014, 16, 34–42. [Google Scholar]
- Azaripour, A.; Kissinger, M.; Farina, V.S.L.; Van Noorden, C.J.; Gerhold-Ay, A.; Willershausen, B.; Cortellini, P. Root coverage with connective tissue graft associated with coronally advanced flap or tunnel technique: A randomized, double-blind, mono-centre clinical trial. J. Clin. Periodontol. 2016, 43, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Bednarz, W.; Żurek, J.; Gedrange, T.; Dominiak, M. A Preliminary Clinical Comparison of the Use of Fascia Lata Allograft and Autogenous Connective Tissue Graft in Multiple Gingival Recession Coverage Based on the Tunnel Technique. Adv. Clin. Exp. Med. 2016, 25, 587–598. [Google Scholar] [CrossRef]
- Cieślik-Wegemund, M.; Wierucka-Młynarczyk, B.; Tanasiewicz, M.; Gilowski, Ł. Tunnel Technique with Collagen Matrix Compared With Connective Tissue Graft for Treatment of Periodontal Recession: A Randomized Clinical Trial. J. Periodontol. 2016, 87, 1436–1443. [Google Scholar] [CrossRef] [PubMed]
- Rakasevic, D.L.; Milinkovic, I.Z.; Jankovic, S.M.; Soldatovic, I.A.; Aleksic, Z.M.; Nikolic-Jakoba, N.S. The use of collagen porcine dermal matrix and connective tissue graft with modified coronally advanced tunnel technique in the treatment of multiple adjacent type I gingival recessions: A randomized, controlled clinical trial. J. Esthet. Restor. Dent. 2020, 32, 681–690. [Google Scholar] [CrossRef]
- Górski, B.; Górska, R.; Wysokińska-Miszczuk, J.; Kaczyński, T. Tunnel technique with enamel matrix derivative in addition to subepithelial connective tissue graft compared with connective tissue graft alone for the treatment of multiple gingival recessions: A randomized clinical trial. Clin. Oral Investig. 2020, 24, 4475–4486. [Google Scholar] [CrossRef]
- Tavelli, L.; Barootchi, S.; Di Gianfilippo, R.; Modarressi, M.; Cairo, F.; Rasperini, G.; Wang, H. Acellular dermal matrix and coronally advanced flap or tunnel technique in the treatment of multiple adjacent gingival recessions. A 12-year follow-up from a randomized clinical trial. J. Clin. Periodontol. 2019, 46, 937–948. [Google Scholar] [PubMed]
- Korkmaz, B.; Balli, U. Clinical evaluation of the treatment of multiple gingival recessions with connective tissue graft or concentrated growth factor using tunnel technique: A randomized controlled clinical trial. Clin. Oral Investig. 2021, 25, 6347–6356. [Google Scholar] [CrossRef] [PubMed]
- Zuhr, O.; Rebele, S.F.; Vach, K.; Petsos, H.; Hürzeler, M.B. Tunnel technique with connective tissue graft versus coronally advanced flap with enamel matrix derivate for root coverage: 2-year results of an RCT using 3D digital measuring for volumetric comparison of gingival dimensions. J. Clin. Periodontol. 2020, 47, 1144–1158. [Google Scholar] [CrossRef]
- Uzun, B.C.; Ercan, E.; Tunalı, M. Effectiveness and predictability of titanium-prepared platelet-rich fibrin for the management of multiple gingival recessions. Clin. Oral Investig. 2018, 22, 1345–1354. [Google Scholar] [CrossRef]
- Stähli, A.; Imber, J.; Raptis, E.; Salvi, G.; Eick, S.; Sculean, A. Effect of enamel matrix derivative on wound healing following gingival recession coverage using the modified coronally advanced tunnel and subepithelial connective tissue graft: A randomised, controlled, clinical study. Clin. Oral Investig. 2020, 24, 1043–1051. [Google Scholar] [CrossRef]
- Parween, S.; George, J.P.; Prabhuji, M. Treatment of Multiple Mandibular Gingival Recession Defects Using MCAT Technique and SCTG With and Without rhPDGF-BB: A Randomized Controlled Clinical Trial. Int. J. Periodontics Restor. Dent. 2020, 40, e43–e51. [Google Scholar] [CrossRef] [PubMed]
- Zuhr, O.; Akakpo, D.; Eickholz, P.; Vach, K.; Hürzeler, M.B.; Petsos, H. Tunnel technique with connective tissue graft versus coronally advanced flap with enamel matrix derivate for root coverage: 5-year results of an RCT using 3D digital measurement technology for volumetric comparison of soft tissue changes. J. Clin. Periodontol. 2021, 48, 949–961. [Google Scholar] [CrossRef]
- Sculean, A.; Cosgarea, R.; Stähli, A.B.; Katsaros, C.; Arweiler, N.B.; Brecx, M.; Deppe, H. The modified coronally advanced tunnel combined with an enamel matrix derivative and subepithelial connective tissue graft for the treatment of isolated mandibular Miller Class I and II gingival recessions: A report of 16 cases. Quintessence Int. 2014, 45, 829–835. [Google Scholar] [PubMed]
- Chaparro, A.; De la Fuente, M.; Albers, D.; Hernandez, D.; Villalobos, A.; Gaedechens, D.; De la Fuente, M. Root Coverage of Multiple Miller Class I and II Recession Defects Using Acellular Dermal Matrix and Tunneling Technique in Maxilla and Mandible: A 1-Year Report. Int. J. Periodontics Restor. Dent. 2015, 35, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Vincent-Bugnas, S.; Charbit, Y.; Lamure, J.; Mahler, P.; Dard, M.M. Modified Tunnel Technique Combined with Enamel Matrix Derivative: A Minimally Invasive Treatment for Single or Multiple Class I Recession Defects. J. Esthet. Restor. Dent. 2015, 27, 145–154. [Google Scholar] [CrossRef]
- Cosgarea, R.; Juncar, R.; Arweiler, N.; Lascu, L.; Sculean, A. Clinical evaluation of a porcine acellular dermal matrix for the treatment of multiple adjacent class I, II, and III gingival recessions using the modified coronally advanced tunnel technique. Quintessence Int. 2016, 47, 739–747. [Google Scholar]
- Nart, J.; Valles, C. Subepithelial Connective Tissue Graft in Combination with a Tunnel Technique for the Treatment of Miller Class II and III Gingival Recessions in Mandibular Incisors: Clinical and Esthetic Results. Int. J. Periodontics Restor. Dent. 2016, 36, 591–598. [Google Scholar] [CrossRef]
- Sculean, A.; Cosgarea, R.; Stähli, A.; Katsaros, C.; Arweiler, N.B.; Miron, R.J.; Deppe, H. Treatment of multiple adjacent maxillary Miller Class I, II, and III gingival recessions with the modified coronally advanced tunnel, enamel matrix derivative, and subepithelial connective tissue graft: A report of 12 cases. Quintessence Int. 2016, 47, 653–659. [Google Scholar]
- Thalmair, T.; Fickl, S.; Wachtel, H. Coverage of Multiple Mandibular Gingival Recessions Using Tunnel Technique with Connective Tissue Graft: A Prospective Case Series. Int. J. Periodontics Restor. Dent. 2016, 36, 859–867. [Google Scholar] [CrossRef]
- Vincent-Bugnas, S.; Borie, G.; Charbit, Y. Treatment of multiple maxillary adjacent class I and II gingival recessions with modified coronally advanced tunnel and a new xenogeneic acellular dermal matrix. J. Esthet. Restor. Dent. 2018, 30, 89–95. [Google Scholar] [CrossRef]
- Mayta-Tovalino, F.; Barboza, J.J.; Pasupuleti, V.; Hernandez, A.V. Efficacy of Tunnel Technique (TUN) versus Coronally Advanced Flap (CAF) in the Management of Multiple Gingival Recession Defects: A Meta-Analysis. Int. J. Dent. 2023, 2023, 8671484. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).