

Convolutional Neural Networks in the Diagnosis of Colon Adenocarcinoma

 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
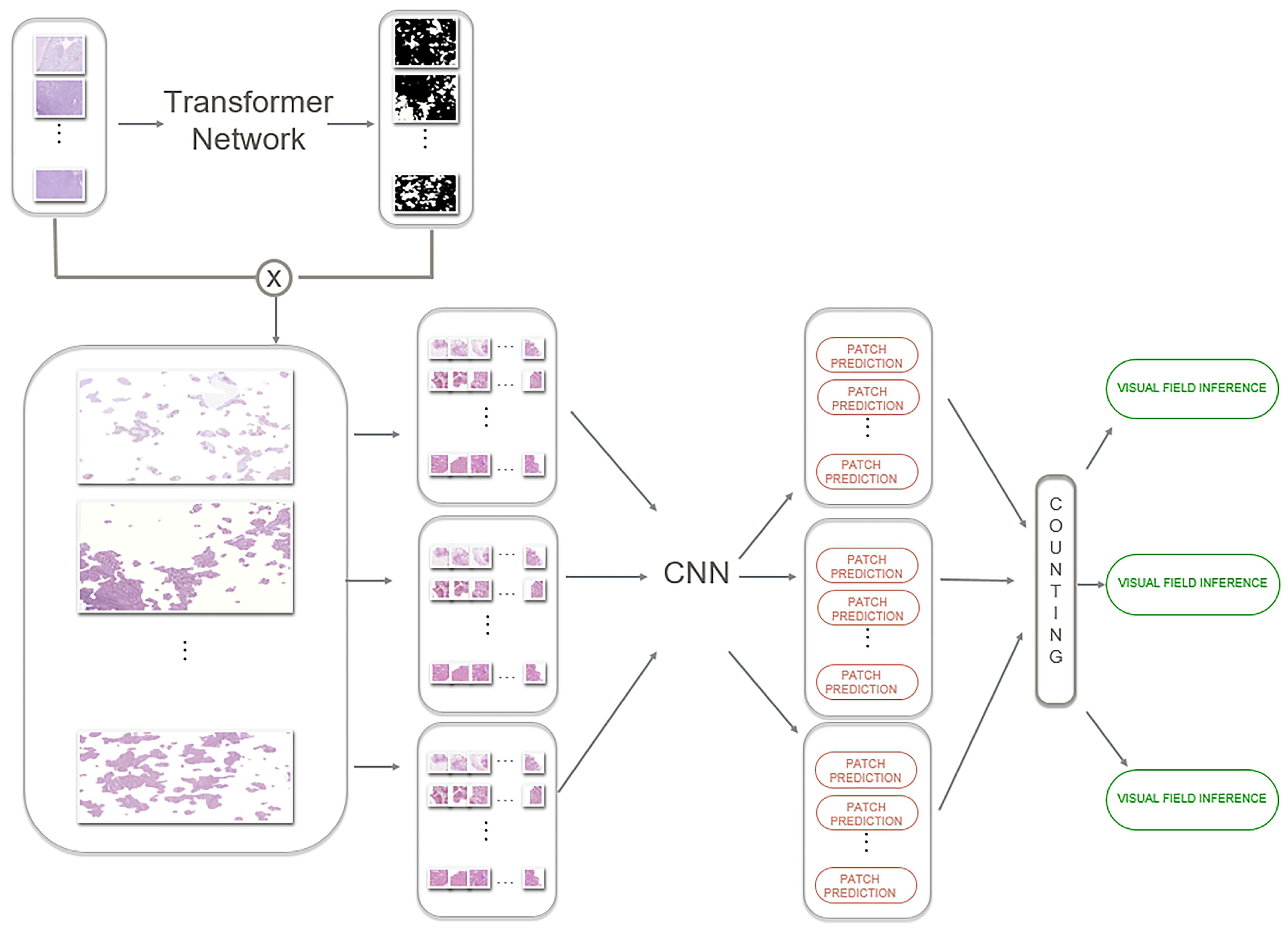
- This is an innovative two-stage pipeline approach, as opposed to previous approaches that grade carcinoma initiating from patches containing glandular regions and other indiscriminative areas (e.g., epithelium).
- This is among the first clinical approaches of this type of pipeline. This study provides early evidence of its suitability for clinical practice and a systematic report of the capabilities of the proposed model.
- In this new data flow, we attempted to understand which CNN model is most suited to extract information from glandular regions and how different models could be combined to further improve cancer staging capabilities. The current work represents a few attempts at applying machine learning strategies in actual clinical practice for colon cancer grading.
- This is among the first attempts to concentrate classification only on glandular regions, which shows a focus of attention similar to the diagnosis of a pathologist. This is one of the most important contributions of the self-attention mechanism learning approach.
2. Related Work
3. Methods
3.1. Patients
3.2. Development of the Algorithm
3.3. Training of the Algorithm
3.4. Diagnosis of Patients
4. Results
4.1. Development of the Algorithm
4.2. Training of the Algorithm
4.3. Diagnosis of Patients
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Testa, U.; Pelosi, E.; Castelli, G. Colorectal cancer: Genetic abnormalities, tumor progression, tumor heterogeneity, clonal evolution and tumor-initiating cells. Med. Sci. 2018, 6, 31. [Google Scholar] [CrossRef]
- Hermanek, P. Colorectal carcinoma: Histopathological diagnosis and staging. Bailliere’s Clin. Gastroenterol. 1989, 3, 511–529. [Google Scholar] [CrossRef]
- Lanza, G.; Messerini, L.; Gafa, R.; Risio, M.; Gruppo Italiano Patologi Apparato Digerente (GIPAD); Societa Italiana di Anatomia Patologica e Citopatologia Diagnostica/International Academy of Pathology, Italian Division. Colorectal tumors: The histology report. Dig. Liver Dis. 2011, 43 (Suppl. S4), S344–S355. [Google Scholar] [CrossRef]
- Tong, Y.; Liu, D.; Zhang, J. Connection and distinction of tumor regression grading systems of gastrointestinal cancer. Pathol. Res. Pract. 2020, 216, 153073. [Google Scholar] [CrossRef]
- Cammarota, F.; Laukkanen, M.O. Mesenchymal Stem/Stromal Cells in Stromal Evolution and Cancer Progression. Stem Cells Int. 2016, 2016, 4824573. [Google Scholar] [CrossRef]
- Fleming, M.; Ravula, S.; Tatishchev, S.F.; Wang, H.L. Colorectal carcinoma: Pathologic aspects. J. Gastrointest. Oncol. 2012, 3, 153–173. [Google Scholar] [CrossRef] [PubMed]
- Deng, S.; Zhang, X.; Yan, W.; Chang, E.I.; Fan, Y.; Lai, M.; Xu, Y. Deep learning in digital pathology image analysis: A survey. Front. Med. 2020, 14, 470–487. [Google Scholar] [CrossRef] [PubMed]
- Salvi, M.; Acharya, U.R.; Molinari, F.; Meiburger, K.M. The impact of pre- and post-image processing techniques on deep learning frameworks: A comprehensive review for digital pathology image analysis. Comput. Biol. Med. 2021, 128, 104129. [Google Scholar] [CrossRef] [PubMed]
- Ciompi, F.; Geessink, O.; Bejnordi, B.E.; de Souza, G.S.; Baidoshvili, A.; Litjens, G.; van Ginneken, B.; Nagtegaal, I.; van der Laak, J. The Importance of Stain Normalization in Colorectal Tissue Classification with Convolutional Networks. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, Australia, 18–21 April 2017; pp. 160–163. [Google Scholar] [CrossRef]
- Wang, E.K.; Zhang, X.; Pan, L.; Cheng, C.; Dimitrakopoulou-Strauss, A.; Li, Y.; Zhe, N. Multi-Path Dilated Residual Network for Nuclei Segmentation and Detection. Cells 2019, 8, 499. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.J.; Tao, Y.H. Deep Learning Techniques for the Classification of Colorectal Cancer Tissue. Electronics 2021, 10, 662. [Google Scholar] [CrossRef]
- Swiderska-Chadaj, Z.; Pinckaers, H.; van Rijthoven, M.; Balkenhol, M.; Melnikova, M.; Geessink, O.; Manson, Q.; Sherman, M.; Polonia, A.; Parry, J.; et al. Learning to detect lymphocytes in immunohistochemistry with deep learning. Med. Image Anal. 2019, 58, 101547. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Chiang, S.F.; Sahoo, P.K.; Mohapatra, S.K.; You, J.F.; Onthoni, D.D.; Hung, H.Y.; Chiang, J.M.; Huang, Y.; Tsai, W.S. Prediction of Colon Cancer Stages and Survival Period with Machine Learning Approach. Cancers 2019, 11, 2007. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Suganthan, P.N. Visual Tracking With Convolutional Random Vector Functional Link Network. IEEE Trans. Cybern. 2017, 47, 3243–3253. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Naseer, M.; Hayat, M.; Zamir, S.W.; Khan, F.S.; Shah, M. Transformers in Vision: A Survey. ACM Comput. Surv. 2022, 54, 1–41. [Google Scholar] [CrossRef]
- Radosavovic, I.; Johnson, J.; Xie, S.N.; Lo, W.Y.; Dollár, P. On Network Design Spaces for Visual Recognition. In Proceedings of the 2019 IEEE/CVF International Conference on Computer Vision (ICCV), Seoul, Republic of Korea, 27 October 27–2 November 2019; pp. 1882–1890. [Google Scholar] [CrossRef]
- Awan, R.; Sirinukunwattana, K.; Epstein, D.; Jefferyes, S.; Qidwai, U.; Aftab, Z.; Mujeeb, I.; Snead, D.; Rajpoot, N. Glandular Morphometrics for Objective Grading of Colorectal Adenocarcinoma Histology Images. Sci. Rep. 2017, 7, 16852. [Google Scholar] [CrossRef] [PubMed]
- Liang, P.; Nakada, I.; Hong, J.W.; Tabuchi, T.; Motohashi, G.; Takemura, A.; Nakachi, T.; Kasuga, T.; Tabuchi, T. Prognostic significance of immunohistochemically detected blood and lymphatic vessel invasion in colorectal carcinoma: Its impact on prognosis. Ann. Surg. Oncol. 2007, 14, 470–477. [Google Scholar] [CrossRef]
- Altunbay, D.; Cigir, C.; Sokmensuer, C.; Gunduz-Demir, C. Color Graphs for Automated Cancer Diagnosis and Grading. IEEE Trans. Biomed. Eng. 2010, 57, 665–674. [Google Scholar] [CrossRef]
- Hou, L.; Samaras, D.; Kurc, T.M.; Gao, Y.; Davis, J.E.; Saltz, J.H. Patch-based Convolutional Neural Network for Whole Slide Tissue Image Classification. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27 June–30 June 2016; pp. 2424–2433. [Google Scholar] [CrossRef]
- Pei, Y.; Mu, L.; Fu, Y.; He, K.; Li, H.; Gu, S.X.; Liu, X.M.; Li, M.Y.; Zhang, H.M.; Li, X.Y. Colorectal Tumor Segmentation of CT Scans Based on a Convolutional Neural Network With an Attention Mechanism. IEEE Access 2020, 8, 64131–64138. [Google Scholar] [CrossRef]
- Zhou, Y.N.; Graham, S.; Koohbanani, N.A.; Shaban, M.; Heng, P.A.; Rajpoot, N. CGC-Net: Cell Graph Convolutional Network for Grading of Colorectal Cancer Histology Images. In Proceedings of the IEEE/CVF International Conference on Computer Vision Workshops, Seoul, Republic of Korea, 27 October–28 October 2019; pp. 388–398. [Google Scholar] [CrossRef]
- Zhan, Z.W.; Liao, G.L.; Ren, X.; Xiong, G.S.; Zhou, W.L.; Jiang, W.C.; Xiao, H. RA-CNN: A Semantic-Enhanced Method in a Multi-Semantic Environment. Int. J. Softw. Sci. Comput. Intell. 2022, 14, 1–14. [Google Scholar] [CrossRef]
- Shaban, M.; Awan, R.; Fraz, M.M.; Azam, A.; Tsang, Y.W.; Snead, D.; Rajpoot, N.M. Context-Aware Convolutional Neural Network for Grading of Colorectal Cancer Histology Images. IEEE Trans. Med. Imaging 2020, 39, 2395–2405. [Google Scholar] [CrossRef]
- Vuong, T.L.T.; Lee, D.; Kwak, J.T.; Kim, K. Multi-task Deep Learning for Colon Cancer Grading. In Proceedings of the 2020 International Conference on Electronics, Information, and Communication (ICEIC), Barcelona, Spain, 19–22 January 2020. [Google Scholar] [CrossRef]
- Sirinukunwattana, K.; Alham, N.K.; Verrill, C.; Rittscher, J. Improving Whole Slide Segmentation Through Visual Context—A Systematic Study. In Medical Image Computing and Computer Assisted Intervention—MICCAI 2018, Pt II; Springer: Cham, Switzerland, 2018; Volume 11071, pp. 192–200. [Google Scholar] [CrossRef]
- Tummala, S.; Kadry, S.; Nadeem, A.; Rauf, H.T.; Gul, N. An Explainable Classification Method Based on Complex Scaling in Histopathology Images for Lung and Colon Cancer. Diagnostics 2023, 13, 1594. [Google Scholar] [CrossRef]
- Bousis, D.; Verras, G.I.; Bouchagier, K.; Antzoulas, A.; Panagiotopoulos, I.; Katinioti, A.; Kehagias, D.; Kaplanis, C.; Kotis, K.; Anagnostopoulos, C.N.; et al. The role of deep learning in diagnosing colorectal cancer. Prz. Gastroenterol. 2023, 18, 266–273. [Google Scholar] [CrossRef]
- Bokhorst, J.M.; Nagtegaal, I.D.; Fraggetta, F.; Vatrano, S.; Mesker, W.; Vieth, M.; van der Laak, J.; Ciompi, F. Deep learning for multi-class semantic segmentation enables colorectal cancer detection and classification in digital pathology images. Sci. Rep. 2023, 13, 8398. [Google Scholar] [CrossRef]
- Reis, H.C.; Turk, V. Transfer Learning Approach and Nucleus Segmentation with MedCLNet Colon Cancer Database. J. Digit. Imaging 2023, 36, 306–325. [Google Scholar] [CrossRef] [PubMed]
- Gertych, A.; Swiderska-Chadaj, Z.; Ma, Z.; Ing, N.; Markiewicz, T.; Cierniak, S.; Salemi, H.; Guzman, S.; Walts, A.E.; Knudsen, B.S. Convolutional neural networks can accurately distinguish four histologic growth patterns of lung adenocarcinoma in digital slides. Sci. Rep. 2019, 9, 1483. [Google Scholar] [CrossRef]
- Chen, W.F.; Ou, H.Y.; Lin, H.Y.; Wei, C.P.; Liao, C.C.; Cheng, Y.F.; Pan, C.T. Development of Novel Residual-Dense-Attention (RDA) U-Net Network Architecture for Hepatocellular Carcinoma Segmentation. Diagnostics 2022, 12, 1916. [Google Scholar] [CrossRef]
- Zhang, Z.; Liang, X.; Dong, X.; Xie, Y.; Cao, G. A Sparse-View CT Reconstruction Method Based on Combination of DenseNet and Deconvolution. IEEE Trans. Med. Imaging 2018, 37, 1407–1417. [Google Scholar] [CrossRef]
- Eun, D.I.; Woo, I.; Park, B.; Kim, N.; Lee, A.S.; Seo, J.B. CT kernel conversions using convolutional neural net for super-resolution with simplified squeeze-and-excitation blocks and progressive learning among smooth and sharp kernels. Comput. Methods Programs Biomed. 2020, 196, 105615. [Google Scholar] [CrossRef] [PubMed]
- Marques, G.; Ferreras, A.; de la Torre-Diez, I. An ensemble-based approach for automated medical diagnosis of malaria using EfficientNet. Multimed. Tools Appl. 2022, 81, 28061–28078. [Google Scholar] [CrossRef] [PubMed]
- Sirinukunwattana, K.; Pluim, J.P.W.; Chen, H.; Qi, X.; Heng, P.A.; Guo, Y.B.; Wang, L.Y.; Matuszewski, B.J.; Bruni, E.; Sanchez, U.; et al. Gland segmentation in colon histology images: The glas challenge contest. Med. Image Anal. 2017, 35, 489–502. [Google Scholar] [CrossRef]
- Shakeel, P.M.; Burhanuddin, M.A.; Desa, M.I. Automatic lung cancer detection from CT image using improved deep neural network and ensemble classifier. Neural Comput. Appl. 2022, 34, 9579–9592. [Google Scholar] [CrossRef]
- Carcagnì, P.; Leo, M.; Cuna, A.; Mazzeo, P.L.; Spagnolo, P.; Celeste, G.; Distante, C. Classification of Skin Lesions by Combining Multilevel Learnings in a DenseNet Architecture. Lect. Notes Comput. Sci. 2019, 11751, 335–344. [Google Scholar] [CrossRef]
- Montagnon, E.; Cerny, M.; Cadrin-Chenevert, A.; Hamilton, V.; Derennes, T.; Ilinca, A.; Vandenbroucke-Menu, F.; Turcotte, S.; Kadoury, S.; Tang, A. Deep learning workflow in radiology: A primer. Insights Imaging 2020, 11, 22. [Google Scholar] [CrossRef] [PubMed]
- Ueno, H.; Kajiwara, Y.; Shimazaki, H.; Shinto, E.; Hashiguchi, Y.; Nakanishi, K.; Maekawa, K.; Katsurada, Y.; Nakamura, T.; Mochizuki, H.; et al. New criteria for histologic grading of colorectal cancer. Am. J. Surg. Pathol. 2012, 36, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Compton, C.C. Optimal pathologic staging: Defining stage II disease. Clin. Cancer Res. 2007, 13, 6862s–6870s. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Collins, G.; Wang, H.; Toh, J.W.T. Pathological Features and Prognostication in Colorectal Cancer. Curr. Oncol. 2021, 28, 5356–5383. [Google Scholar] [CrossRef]
- Puppa, G.; Sonzogni, A.; Colombari, R.; Pelosi, G. TNM staging system of colorectal carcinoma: A critical appraisal of challenging issues. Arch. Pathol. Lab. Med. 2010, 134, 837–852. [Google Scholar] [CrossRef] [PubMed]
- Klaver, C.E.L.; van Huijgevoort, N.C.M.; de Buck van Overstraeten, A.; Wolthuis, A.M.; Tanis, P.J.; van der Bilt, J.D.W.; Sagaert, X.; D’Hoore, A. Locally Advanced Colorectal Cancer: True Peritoneal Tumor Penetration is Associated with Peritoneal Metastases. Ann. Surg. Oncol. 2018, 25, 212–220. [Google Scholar] [CrossRef]
- Maffeis, V.; Nicole, L.; Cappellesso, R. RAS, Cellular Plasticity, and Tumor Budding in Colorectal Cancer. Front. Oncol. 2019, 9, 1255. [Google Scholar] [CrossRef]
- Maguire, A.; Sheahan, K. Controversies in the pathological assessment of colorectal cancer. World J. Gastroenterol. 2014, 20, 9850–9861. [Google Scholar] [CrossRef]
- Harada, S.; Morlote, D. Molecular Pathology of Colorectal Cancer. Adv. Anat. Pathol. 2020, 27, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.T.; Duong, H.Q. The molecular characteristics of colorectal cancer: Implications for diagnosis and therapy. Oncol. Lett. 2018, 16, 9–18. [Google Scholar] [CrossRef]
- Vaswani, A.; Shazeer, N.; Parmar, N.; Uszkoreit, J.; Jones, L.; Gomez, A.N.; Kaiser, L.; Polosukhin, I. Attention Is All You Need. In Proceedings of the 31st Annual Conference on Neural Information Processing Systems (NIPS 2017), Long Beach, CA, USA, 4 December 2017; Volume 30. [Google Scholar] [CrossRef]
- Awan, R.; Al-Maadeed, S.; Al-Saady, R.; Bouridane, A. Glandular structure-guided classification of microscopic colorectal images using deep learning. Comput. Electr. Eng. 2020, 85, 106450. [Google Scholar] [CrossRef]
- Shi, Q.S.; Katuwal, R.; Suganthan, P.N.; Tanveer, M. Random vector functional link neural network based ensemble deep learning. Pattern Recogn. 2021, 117, 107978. [Google Scholar] [CrossRef]
- Ho, C.; Zhao, Z.; Chen, X.F.; Sauer, J.; Saraf, S.A.; Jialdasani, R.; Taghipour, K.; Sathe, A.; Khor, L.Y.; Lim, K.H.; et al. A promising deep learning-assistive algorithm for histopathological screening of colorectal cancer. Sci. Rep. 2022, 12, 2222. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Dataset | Normal | Low Grade | High Grade | Total |
|---|---|---|---|---|
| CRC | 71 | 33 | 35 | 139 |
| Extended CRC | 120 | 120 | 60 | 300 |
| Directory ID | Clinical Diagnosis | Number of Images |
|---|---|---|
| Patient 1 | Intermediate | 202 |
| Patient 2 | High | 192 |
| Patient 3 | Low | 146 |
| Patient 4 | Low | 240 |
| Patient 5 | Intermediate | 242 |
| Patient 6 | Intermediate | 156 |
| Patient 7 | High | 270 |
| Patient 8 | High | 180 |
| Patient 9 | High | 189 |
| Patient 10 | Intermediate | 328 |
| Patient 11 | High | 110 |
| No Tumor | Low Grade | High Grade | Background | |
|---|---|---|---|---|
| Fold 1 | 20911 | 28298 | 13084 | 8799 |
| Fold 2 | 22430 | 29042 | 12412 | 8768 |
| Fold 3 | 22879 | 28388 | 13495 | 6302 |
| Model | Average (%) (Binary) | Weighted (%) (Binary) | Average (%) (3-Classes) | Weghted (%) (3-Classes) |
|---|---|---|---|---|
| D121 | 94.98 ± 2.14 | 95.69 ± 1.99 | 87.24 ± 2.94 | 83.33 ± 2.04 |
| EffB0 | 93.63 ± 0.94 | 93.80 ± 1.10 | 85.89 ± 3.64 | 83.55 ± 3.54 |
| EffB1 | 95.64 ± 1.23 | 94.79 ± 1.15 | 85.89 ± 3.64 | 83.56 ± 3.39 |
| EffB2 | 96.99 ± 2.94 | 96.65 ± 3.11 | 87.58 ± 3.36 | 85.54 ± 2.21 |
| EffB3 | 96.65 ± 2.05 | 96.22 ± 2.22 | 86.57 ± 2.68 | 83.31 ± 1.82 |
| EffB4 | 95.31 ± 1.24 | 94.36 ± 1.27 | 84.89 ± 2.91 | 82.44 ± 1.84 |
| EffB5 | 95.98 ± 1.62 | 95.66 ± 1.72 | 87.57 ± 3.37 | 84.98 ± 3.80 |
| EffB7 | 95.98 ± 1.62 | 95.36 ± 1.68 | 86.90 ± 3.01 | 84.41 ± 2.78 |
| ResNet-50 | 94.96 ± 0.79 | 95.45 ± 1.20 | 86.57 ± 2.43 | 80.60 ± 1.73 |
| Res152 | 95.64 ± 0.94 | 95.82 ± 1.01 | 84.22 ± 4.58 | 79.99 ± 4.13 |
| SER50 | 93.30 ± 2.47 | 93.14 ± 2.54 | 84.89 ± 3.02 | 81.63 ± 2.08 |
| Model | Average (%) (Binary) | Weighted (%) (Binary) | Average (%) (3-Classes) | Weighted (%) (3-Classes) |
|---|---|---|---|---|
| 200MF | 92.97 ± 3.73 | 93.87 ± 2.92 | 83.90 ± 0.76 | 80.54 ± 1.03 |
| 400MF | 93.97 ± 2.94 | 93.99 ± 3.11 | 84.23 ± 2.62 | 81.92 ± 1.74 |
| 800MF | 93.65 ± 4.77 | 94.15 ± 4.17 | 84.24 ± 1.63 | 81.10 ± 1.41 |
| 4.0GF | 95.64 ± 0.94 | 95.37 ± 1.52 | 84.55 ± 2.57 | 81.36 ± 1.43 |
| 6.4GF | 94.31 ± 2.48 | 94.26 ± 2.15 | 86.57 ± 2.12 | 83.58 ± 2.21 |
| 8.0GF | 91.95 ± 2.15 | 92.19 ± 2.40 | 82.55 ± 1.70 | 80.81 ± 2.06 |
| 12GF | 93.97 ± 2.93 | 94.28 ± 2.93 | 84.22 ± 2.41 | 82.21 ± 3.09 |
| 16GF | 94.97 ± 1.62 | 94.24 ± 2.08 | 85.22 ± 3.93 | 83.29 ± 3.45 |
| 32GF | 94.64 ± 2.49 | 94.55 ± 2.79 | 84.56 ± 2.68 | 81.65 ± 2.39 |
| (a) | ||||
| Label | Models | Strategy | ||
| E1 | DenseNet121 EfficientNet-B7 RegNetY16GF | Max-Voting | ||
| E2 | DenseNet121 EfficientNet-B7 RegNetY16GF SE-ResNet50 | Max-Voting | ||
| E3 | DenseNet121 EfficientNet-B7 RegNetY16GF RegNetY6.4GF | Max-Voting | ||
| E4 | DenseNet121 EfficientNet-B7 RegNetY6.4GF | Max-Voting | ||
| E5 | DenseNet121 EfficientNet-B2 RegNetY16GF | Max-Voting | ||
| E6 | DenseNet121 EfficientNet-B2 RegNetY16GF | Max-Voting | ||
| E7 | DenseNet121 EfficientNet-B2 | Argmax | ||
| E8 | DenseNet121 EfficientNet-B7 RegNetY16GF SE-ResNet50 | Argmax | ||
| E9 | EfficientNet-B7 RegNetY16GF SE-ResNet50 | Argmax | ||
| E10 | DenseNet121 EfficientNet-B2 RegNetY16GF | Argmax | ||
| E11 | DenseNet121 EfficientNet-B2 RegNetY16GF | Argmax | ||
| E12 | EfficientNet-B1 EfficientNet-B2 | Argmax | ||
| (b) | ||||
| Model | Average (%) (Binary) | Weighted (%) (Binary) | Average (%) (3-classes) | Weighted (%) (3-classes) |
| E1 | 95.65 ± 1.87 | 95.52 ± 1.85 | 86.90 ± 4.16 | 84.15 ± 3.81 |
| E2 | 95.31 ± 2.48 | 95.68 ± 2.41 | 87.24 ± 3.37 | 83.88 ± 3.08 |
| E3 | 95.31 ± 1.68 | 95.40 ± 1.89 | 87.23 ± 4.18 | 84.15 ± 4.10 |
| E4 | 94.98 ± 1.62 | 95.12 ± 1.88 | 87.23 ± 1.18 | 84.15 ± 4.10 |
| E5 | 95.98 ± 2.45 | 95.81 ± 2.72 | 86.90 ± 4.39 | 84.15 ± 3.81 |
| E6 | 95.31 ± 2.34 | 95.40 ± 2.37 | 86.23 ± 3.37 | 83.32 ± 2.74 |
| E7 | 95.65 ± 2.05 | 95.82 ± 2.23 | 87.91 ± 3.33 | 84.72 ± 3.43 |
| E8 | 95.98 ± 2.15 | 95.95 ± 2.26 | 87.57 ± 3.75 | 84.71 ± 3.44 |
| E9 | 97.32 ± 1.26 | 97.33 ± 1.57 | 88.24 ± 4.26 | 85.53 ± 3.76 |
| T + E5 | 99.00 ± 0.82 | 99.02 ± 0.71 | 89.24 ± 4.09 | 87.49 ± 3.61 |
| T + E7 | 99.33 ± 0.94 | 99.44 ± 0.79 | 89.58 ± 3.83 | 87.22 ± 3.87 |
| T + E10 | 98.33 ± 1.25 | 98.46 ± 1.10 | 88.24 ± 4.10 | 85.52 ± 3.88 |
| T + E11 | 99.33 ± 0.94 | 99.44 ± 0.79 | 90.25 ± 3.74 | 88.06 ± 3.14 |
| T + E12 | 99.00 ± 0.82 | 99.02 ± 0.71 | 89.92 ± 3.00 | 87.49 ± 2.36 |
| Patient 1 | Hepatic metastasis from moderately differentiated adenocarcinoma. Pathological stage: pTx, pNx, pM1a. Observations: Residues of mild hepatic steatosis, surgical margins free of neoplasia, KRas mutation at exon 2. |
| Patient 2 | Poorly differentiated adenocarcinoma. Pathological stage: pT4a, pNx. Observations: Diffuse infiltration to omental tissue, positive immunohistochemical staining for cytokeratin 20 and CDX2 but negative for cytokeratin 7, suggesting large intestine origin for the pathology. |
| Patient 3 | Well-differentiated adenocarcinoma. Pathological stage: pT1, pNx. Observations: No metastasis, KRas mutation at exon 2. |
| Patient 4 | Poorly differentiated adenocarcinoma. Pathological stage: pT3, pN0. Observations: Neoplastic infiltration to the muscular layer and to perivisceral fat, no lymphovascular infiltration, nine tumor buds observed suggesting an intermediate risk of vascular metastasis, lymph nodes free of neoplasia, omemtum free of neoplasia, surgical margins free of neoplasia. KRas mutation at exon 2. |
| Patient 5 | Moderately differentiated colloid adenocarcinoma and tubulovillous adenoma with low-grade epithelial dysplasia. Pathological stage: pT3 pN0. Observations: Neoplastic infiltration to the perivisceral fat, 19 lymph nodes have metastasis, no lymphovascular infiltration, appendix free of neoplasia, surgical margins free of neoplasia. KRas mutation at exon 2. |
| Patient 6 | Moderately differentiated adenocarcinoma. Pathological stage: pT3 pN1a. Observations: Neoplastic invasion to muscle layer and to visceral fat, one lymph node has metastasis suggesting low risk of vascular metastasis. |
| Patient 7 | Poorly differentiated adenocarcinoma. Pathological stage: pT3, pN0. Observations: Neoplastic infiltration to muscle layer and to visceral fat, one tumor bud observed suggesting low risk of vascular metastasis, lymph nodes free of metastasis, surgical margins free of neoplasia. |
| Patient 8 | Poorly differentiated adenocarcinoma. Pathological stage: pT4b pNx. Observations: Neoplastic infiltration to ovary capsule and extrinsically to colon wall, fallopian tubes free of infiltration, atrophic endometrium, chronic cervicitis. Positive immunohistochemical staining for CDX2 and cytokeratin 20 but negative for PAX8, cytokeratin 7, WT1, and p53, suggesting large intestine origin for the pathology. |
| Patient 9 | Poorly differentiated adenocarcinoma. Pathological stage: pT4b, pN1b. Observations: The neoplasm infiltrates the muscular layer up to the perivisceral fat. Over ten tumor buds observed suggesting a high risk of vascular metastasis, neoplastic infiltration at omentum, extrinsic neoplastic infiltration on the serosa of the bowel, no lymphovascular infiltration, three lymph nodes have metastasis, mucosa of the small intestine free of neoplasia, surgical margins free of neoplasia. KRas mutation at exon 2. |
| Patient 10 | Moderately differentiated adenocarcinoma. Pathological stage: pT3, pN0. Observations: The neoplasm infiltrates the muscular layer up to the perivisceral fat. Over ten tumor buds observed suggesting a high risk of vascular metastasis, a moderate peritumoral infiltration, no lymphovascular infiltration, lymph nodes free of neoplasia, surgical margins free of neoplasia. |
| Patient 11 | Poorly differentiated adenocarcinoma with hepatic metastasis. Pathological stage: pT3 pN2p pM1a Observations: Neoplastic infiltration to muscle layer and to visceral fat, chronic lithiasic cholecystitis, surgical margins free of neoplasia. KRas mutation at exon 2. Observations: Neoplastic infiltration to muscle layer and to visceral fat, chronic lithiasic cholecystitis, surgical margins free of neoplasia. KRas mutation at exon 2. |
| Patient | Clinical Diagnosis | Algorithm Well-Differentiated | Algorithm Moderately Differentiated | Algorithm Poorly Differentiated |
|---|---|---|---|---|
| Patient 1 | Moderately differentiated | 2% (4) | 19% (38) | 79% (160) |
| Patient 2 | Poorly differentiated | 4% (8) | 14% (27) | 82% (157) |
| Patient 3 | Well differentiated | 61% (89) | 21% (30) | 18% (27) |
| Patient 4 | Poorly differentiated | 5% (12) | 22% (53) | 73% (175) |
| Patient 5 | Moderately differentiated | 0% (0) | 48% (115) | 52% (126) |
| Patient 6 | Moderately differentiated | 0% (0) | 52% (81) | 48% (75) |
| Patient 7 | Poorly differentiated | 0% (0) | 21% (57) | 79% (213) |
| Patient 8 | Poorly differentiated | 0% (0) | 3% (5) | 97% (178) |
| Patient 9 | Poorly differentiated | 0% (0) | 6% (11) | 94% (178) |
| Patient 10 | Moderately differentiated | 0% (0) | 38% (124) | 62% (204) |
| Patient 11 | Poorly differentiated | 3% (3) | 74% (81) | 13% (26) |
| Model | Average (%) (Binary) | Weight (%) (Binary) | Average (%) (3-Classes) | Weight (%) (3-Classes) |
|---|---|---|---|---|
| Proposed Solutions | ||||
| EffB2 | 96.99 ± 2.94 | 96.65 ± 3.11 | 87.58 ± 3.36 | 85.54 ± 2.21 |
| 4.0GF | 95.64 ± 0.94 | 95.37 ± 1.52 | 84.55 ± 2.57 | 81.36 ± 1.43 |
| 6.4GF | 94.31 ± 2.48 | 94.26 ± 2.15 | 86.57 ± 2.12 | 83.58 ± 2.21 |
| T + EffB1 | 99.67 ± 0.47 | 99.72 ± 0.39 | 89.58 ± 4.17 | 87.50 ± 3.54 |
| T + EffB2 | 98.66 ± 0.95 | 98.74 ± 0.91 | 89.92 ± 2.50 | 87.22 ± 2.08 |
| T + E11 | 99.33 ± 0.94 | 99.44 ± 0.79 | 90.25 ± 3.74 | 88.06 ± 3.14 |
| Previous Work | ||||
| ResNet50 [24] | 95.67 ± 2.05 | 95.69 ± 1.53 | 86.33 ± 0.94 | 80.56 ± 1.04 |
| LR+LA-CNN [24] | 97.67 ± 0.94 | 97.64 ± 0.79 | 86.67 ± 1.70 | 84.17 ± 2.36 |
| CNN-LSTM [26] | 95.33 ± 2.87 | 94.17 ± 3.58 | 82.33 ± 2.62 | 83.89 ± 2.08 |
| CNN-SVM [20] | 96.00 ± 0.82 | 96.39 ± 1.37 | 82.00 ± 1.63 | 76.67 ± 2.97 |
| CNN-LR [20] | 96.33 ± 1.70 | 96.39 ± 1.37 | 86.67 ± 1.25 | 82.50 ± 0.68 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leo, M.; Carcagnì, P.; Signore, L.; Corcione, F.; Benincasa, G.; Laukkanen, M.O.; Distante, C. Convolutional Neural Networks in the Diagnosis of Colon Adenocarcinoma. AI 2024, 5, 324-341. https://doi.org/10.3390/ai5010016
Leo M, Carcagnì P, Signore L, Corcione F, Benincasa G, Laukkanen MO, Distante C. Convolutional Neural Networks in the Diagnosis of Colon Adenocarcinoma. AI. 2024; 5(1):324-341. https://doi.org/10.3390/ai5010016
Chicago/Turabian StyleLeo, Marco, Pierluigi Carcagnì, Luca Signore, Francesco Corcione, Giulio Benincasa, Mikko O. Laukkanen, and Cosimo Distante. 2024. "Convolutional Neural Networks in the Diagnosis of Colon Adenocarcinoma" AI 5, no. 1: 324-341. https://doi.org/10.3390/ai5010016
APA StyleLeo, M., Carcagnì, P., Signore, L., Corcione, F., Benincasa, G., Laukkanen, M. O., & Distante, C. (2024). Convolutional Neural Networks in the Diagnosis of Colon Adenocarcinoma. AI, 5(1), 324-341. https://doi.org/10.3390/ai5010016