
Genetic Variants in the TBC1D2B Gene Are Associated with Ramon Syndrome and Hereditary Gingival Fibromatosis

 , , , ,
, , , ,  ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Results
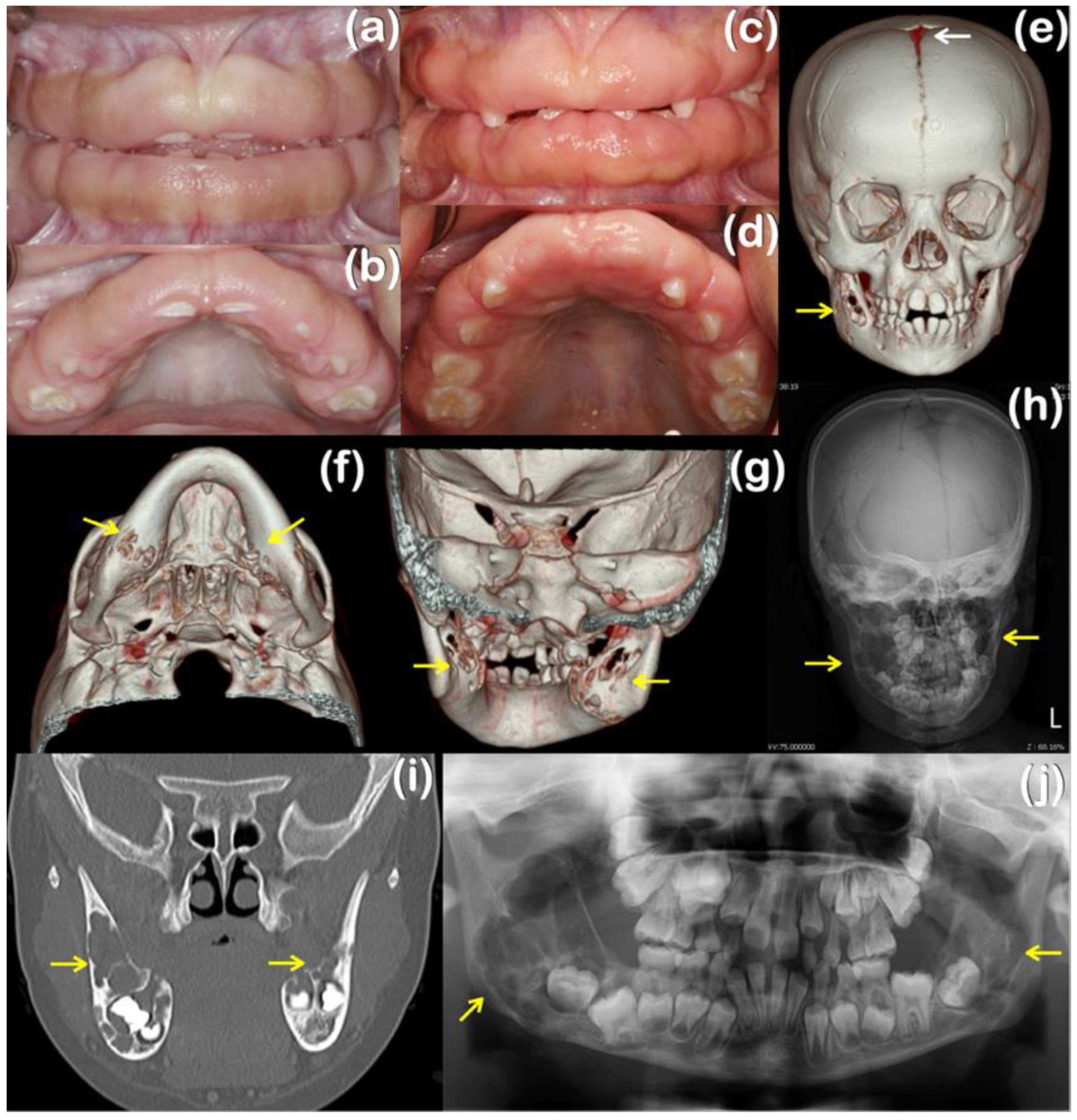
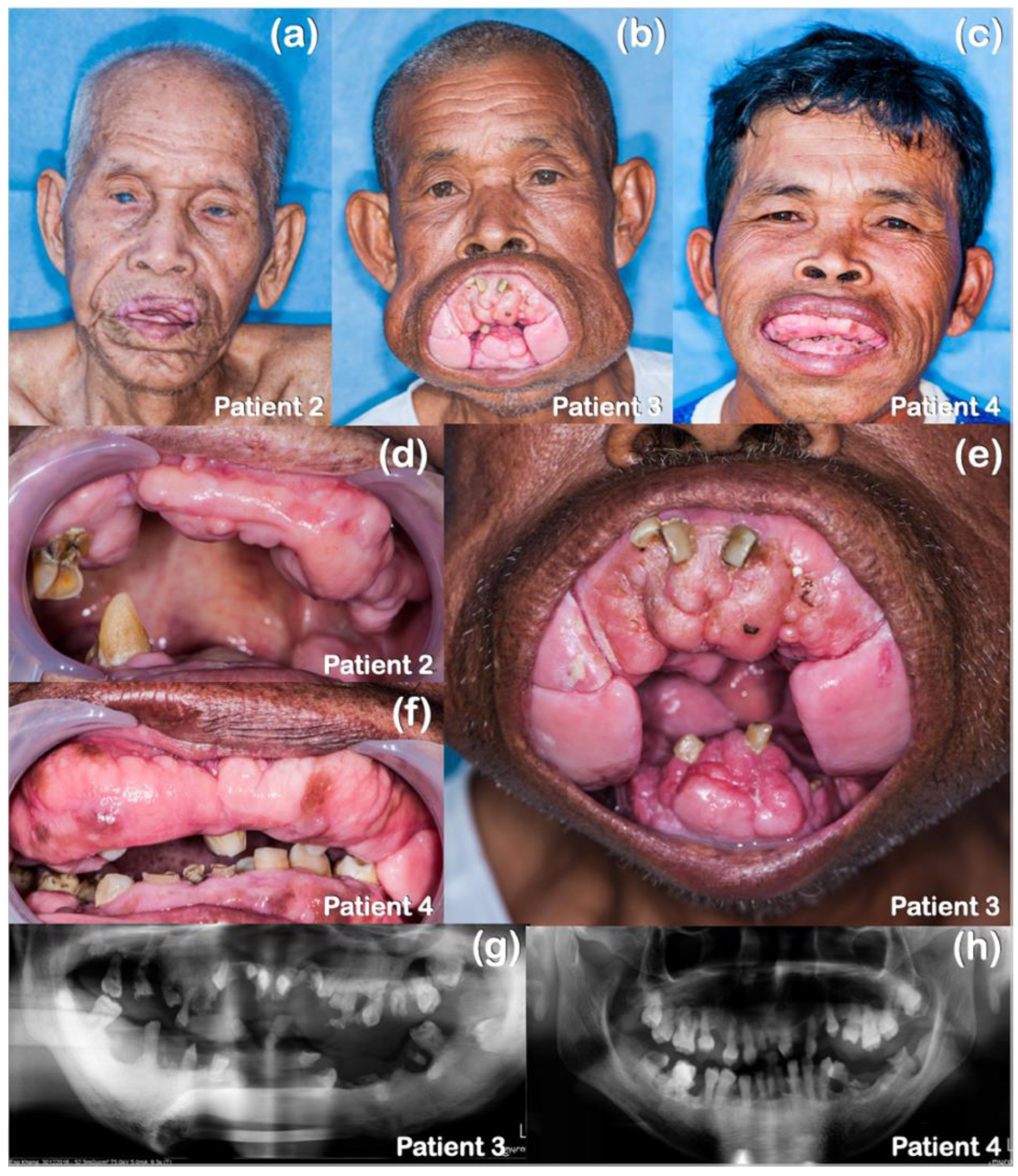
2.1. Patient Reports
2.2. Bioinformatic and Mutation Analysis
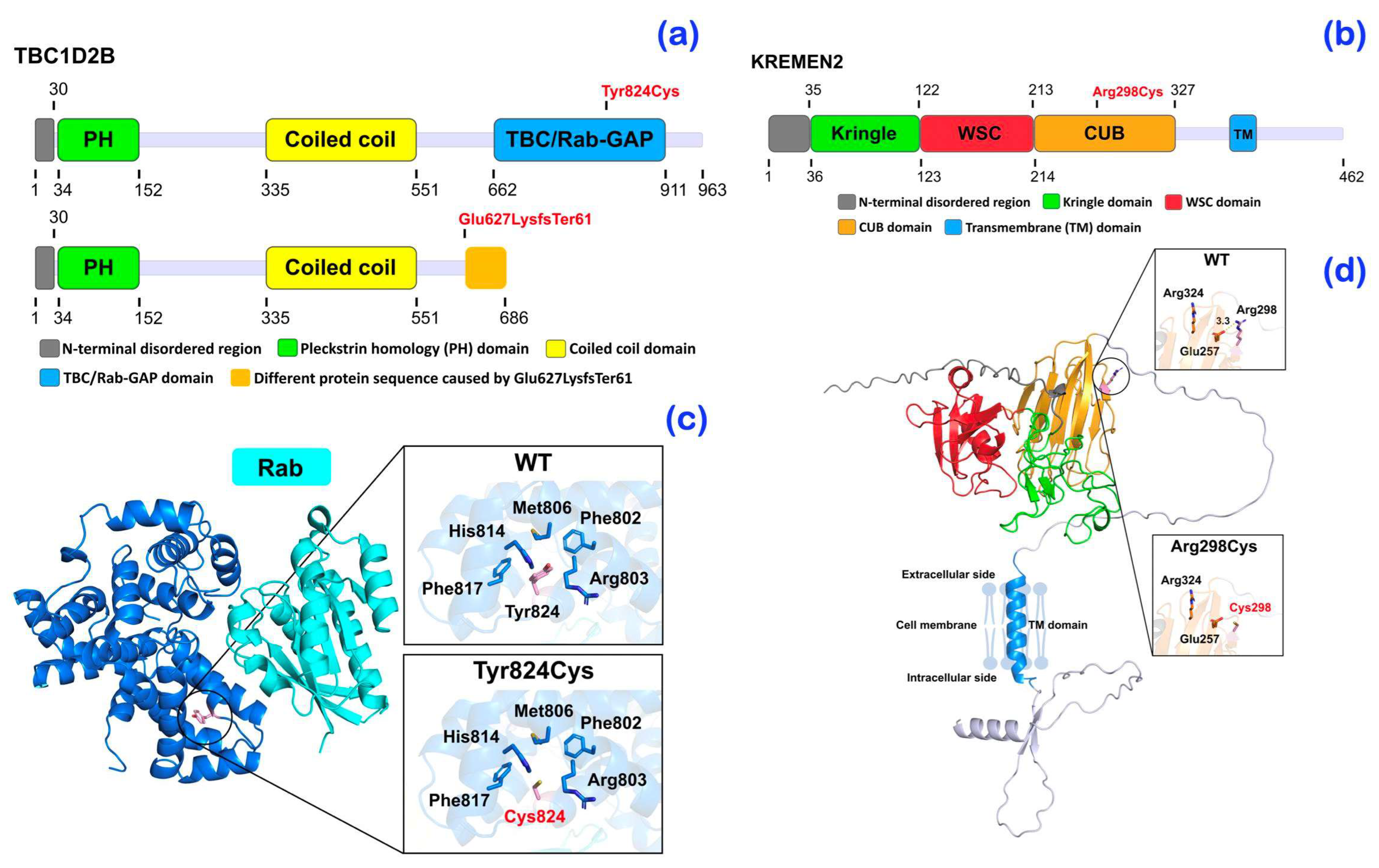
2.3. Protein Models
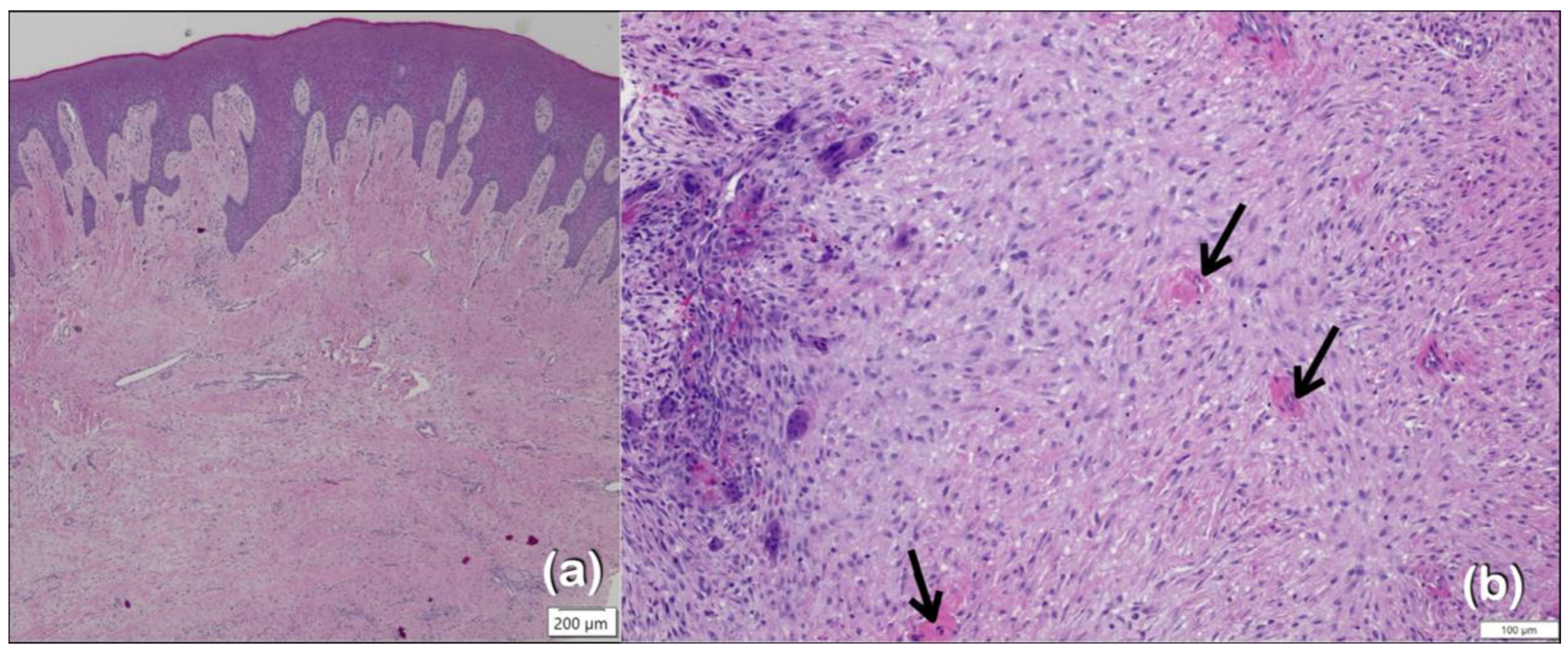
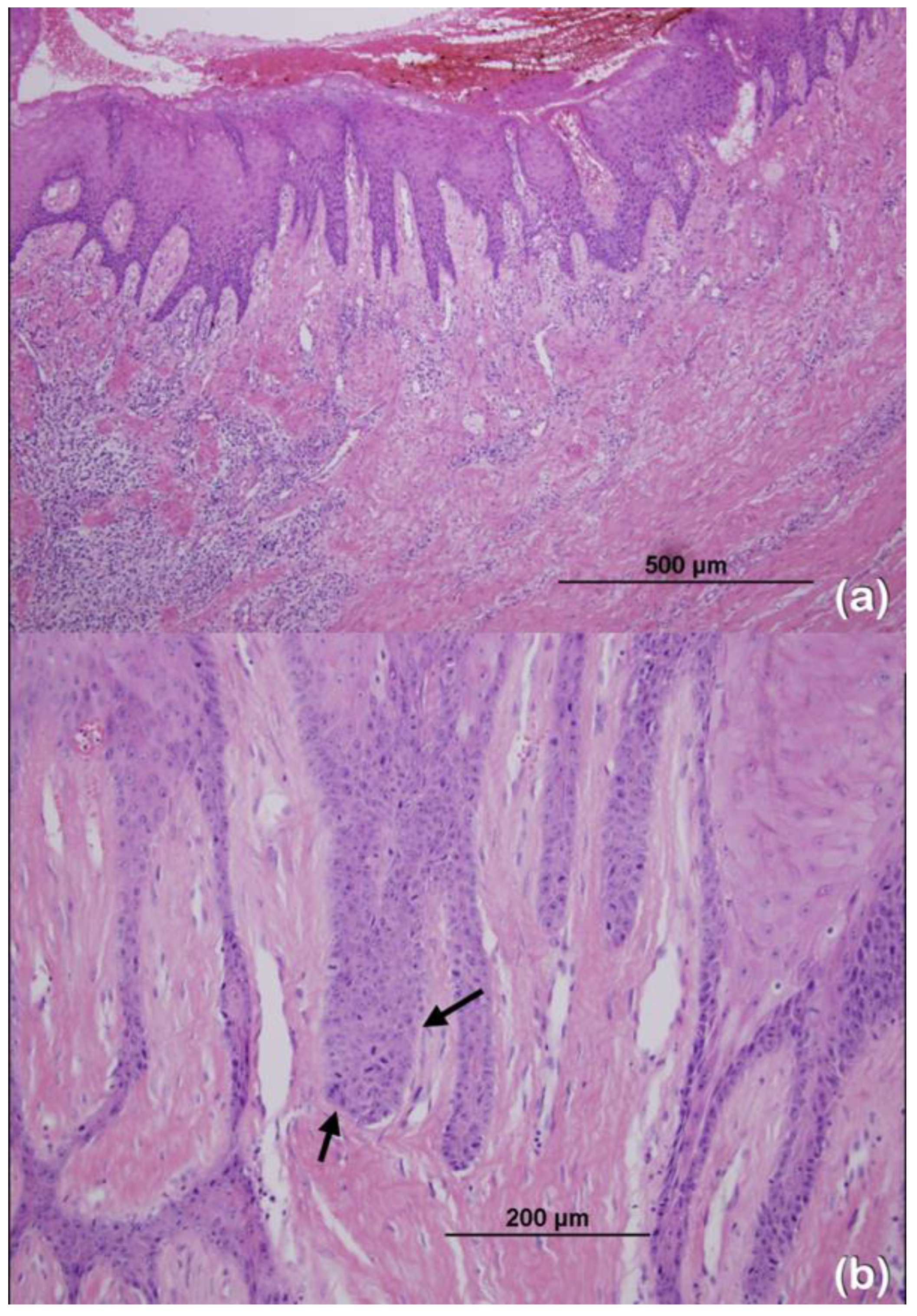
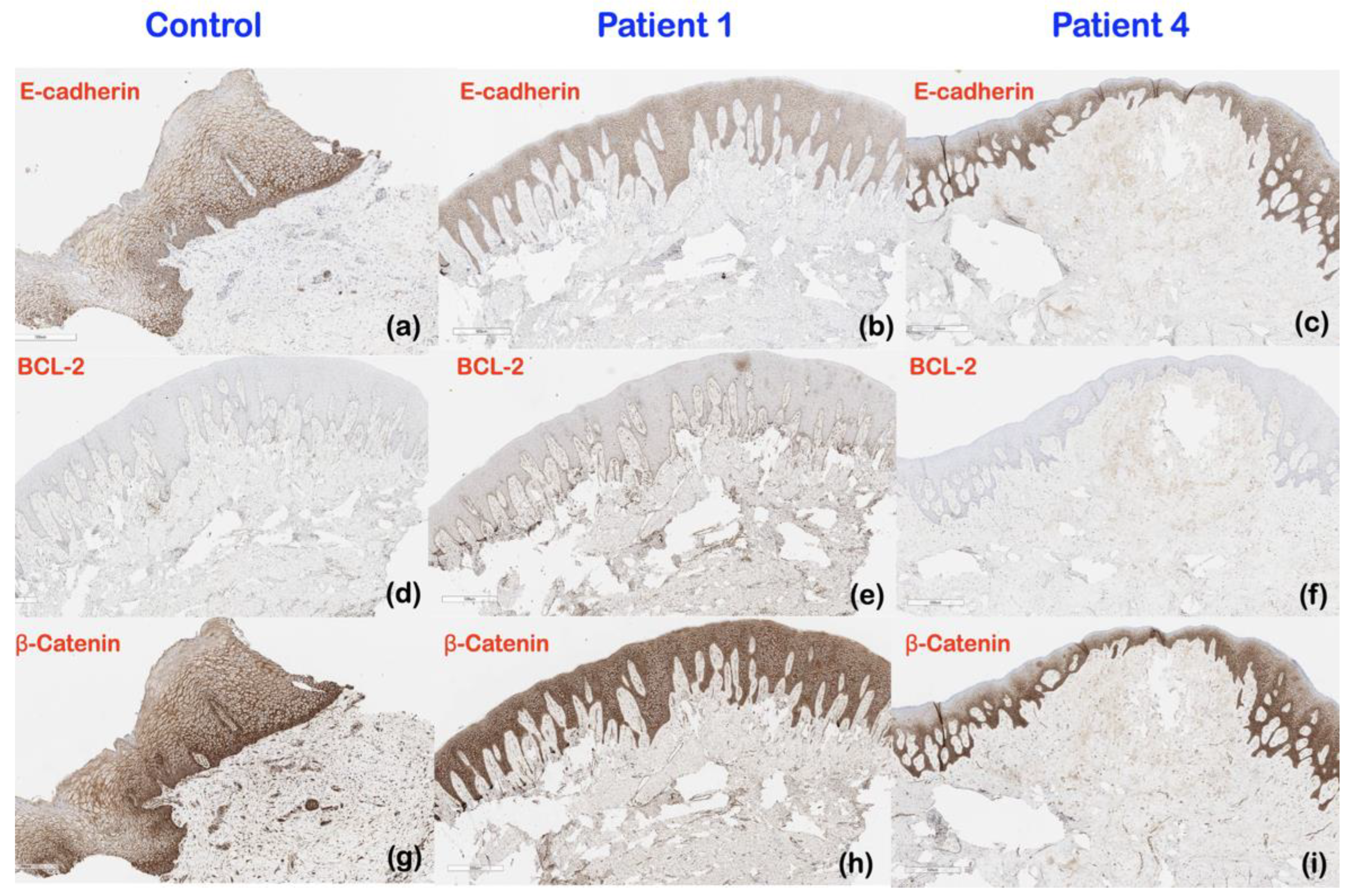
2.4. Immunohistochemical Findings
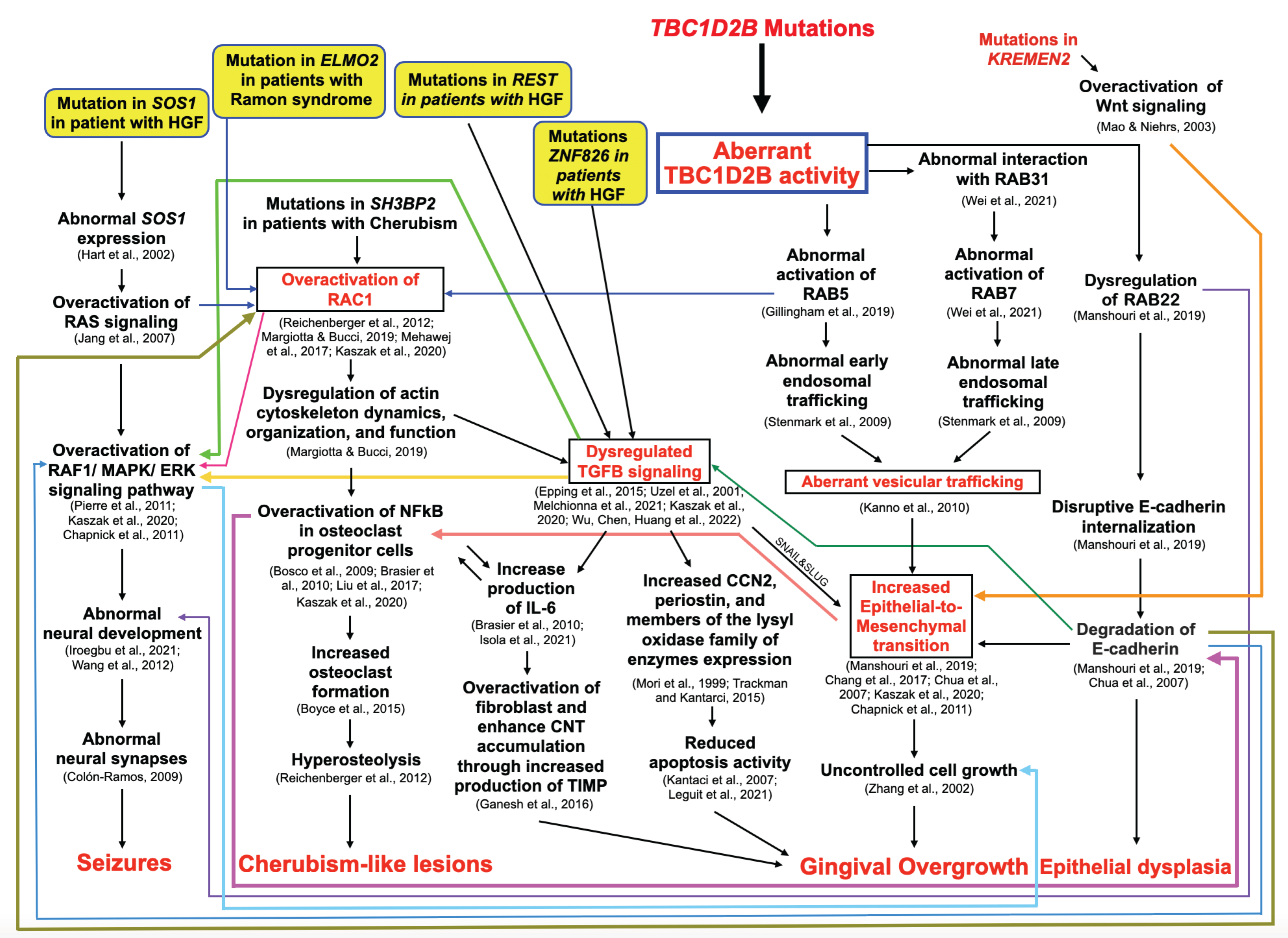
3. Discussion
3.1. Genetic Variant in the TBC1D2B Gene and Ramon Syndrome
3.2. Genetic Variants in the TBC1D2B Gene and Gingival Fibromatosis
3.2.1. Genetic Mechanisms and Clinical Implications
3.2.2. Immunohistochemistry Results and Clinical Implications
3.3. Genetic Variants in TBC1D2B and KREMEN2 and Hereditary Gingival Fibromatosis
3.3.1. A Heterozygous Missense Variant in the TBC1D2B Gene in Patients 2–4
3.3.2. A Novel Heterozygous Variant in the KREMEN2 Gene in Patients 2–4
3.3.3. Genetic Variant in the KREMEN2 Gene and Dense Mandibular Bone in Patients 3 and 4
3.4. Genetic Variant in the TBC1D2B Gene and Cherubism-like Lesions
3.5. Genetic Variant in the TBC1D2B Gene and Seizures
3.6. Genetic Variants in the TBC1D2B Gene and Epithelial Dysplasia
3.7. Genetic Variants in the TBC1D2B Gene and Recurrence of Overgrown Gingiva
3.8. Future Research Directions
4. Materials and Methods
4.1. Ethics Statement
4.2. Patient Recruitment
4.3. Whole Exome Sequencing, Mutation Analysis, and Bioinformatic Analyses
4.4. Structural Assessment of Variants
4.5. Immunohistochemistry
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramon, Y.; Berman, W.; Bubis, J.J. Gingival fibromatosis combined with cherubism. Oral Surg. Oral Med. Oral Pathol. 1967, 24, 435–448. [Google Scholar] [CrossRef] [PubMed]
- Pridmore, C.; Baraitser, M.; Leonard, J. Ramon syndrome with diabetes mellitus and vascular skin lesions in two sibs. Clin. Dysmorphol. 1992, 1, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Suhanya, J.; Aggarwal, C.; Mohideen, K.; Jayachandran, S.; Ponniah, I. Cherubism combined with epilepsy, mental retardation and gingival fibromatosis (Ramon syndrome): A case report. Head Neck Pathol. 2010, 4, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Pina-Neto, J.M.; Moreno, A.F.; Silva, L.R.; Velludo, M.A.; Petean, E.B.; Ribeiro, M.V.; Athayde-Junior, L.; Voltarelli, J.C. Cherubism, gingival fibromatosis, epilepsy, and mental deficiency (Ramon syndrome) with juvenile rheumatoid arthritis. Am. J. Med. Genet. 1986, 25, 433–441. [Google Scholar] [CrossRef]
- Mehawej, C.; Hoischen, A.; Farah, R.A.; Marey, I.; David, M.; Stora, S.; Lachlan, K.; Brunner, H.G.; Mégarbané, A. Homozygous mutation in ELMO2 may cause Ramon syndrome. Clin. Genet. 2018, 93, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Harms, F.L.; Parthasarathy, P.; Zorndt, D.; Alawi, M.; Fuchs, S.; Halliday, B.J.; McKeown, C.; Sampaio, H.; Radhakrishnan, N.; Radhakrishnan, S.K.; et al. Biallelic loss-of-function variants in TBC1D2B cause a neurodevelopmental disorder with seizures and gingival overgrowth. Hum. Mutat. 2020, 41, 1645–1661. [Google Scholar] [CrossRef] [PubMed]
- Correia-Costa, G.R.; de Leeuw, N.; Pfundt, R.; Sgardioli, I.C.; Dos Santos, A.P.; de Lima Santos, M.; Gil-da-Silva-Lopes, V.L.; Vieira, T.P. Biallelic frameshift variant in the TBC1D2B gene in two siblings with progressive gingival overgrowth, fibrous dysplasia of face, and mental deterioration. Clin. Genet. 2022, 102, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Strzelec, K.; Dziedzic, A.; Łazarz-Bartyzel, K.; Grabiec, A.M.; Gutmajster, E.; Kaczmarzyk, T.; Plakwicz, P.; Gawron, K. Clinics and genetic background of hereditary gingival fibromatosis. Orphanet J. Rare Dis. 2021, 16, 492. [Google Scholar] [CrossRef] [PubMed]
- Gawron, K.; Łazarz-Bartyzel, K.; Potempa, J.; Chomyszyn-Gajewska, M. Gingival fibromatosis: Clinical, molecular and therapeutic issues. Orphanet J. Rare Dis. 2016, 11, 9. [Google Scholar] [CrossRef]
- Hart, T.C.; Pallos, D.; Bozzo, L.; Almeida, O.P.; Marazita, M.L.; O’Connell, J.R.; Cortelli, J.R. Evidence of genetic heterogeneity for hereditary gingival fibromatosis. J. Dent. Res. 2000, 79, 1758–1764. [Google Scholar] [CrossRef]
- Poulopoulos, A.; Kittas, D.; Sarigelou, A. Current concepts on gingival fibromatosis-related syndromes. J. Investig. Clin. Dent. 2011, 2, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Coletta, R.D.; Graner, E. Hereditary gingival fibromatosis: A systematic review. J. Periodontol. 2006, 77, 753–764. [Google Scholar] [CrossRef] [PubMed]
- Boutiou, E.; Ziogas, I.A.; Giannis, D.; Doufexi, A.E. Hereditary gingival fibromatosis in children: A systematic review of the literature. Clin. Oral Investig. 2021, 25, 3599–3607. [Google Scholar] [CrossRef] [PubMed]
- Chaurasia, A. Hereditary gingival fibromatosis. Natl. J. Maxillofac. Surg. 2014, 5, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Hart, T.C.; Zhang, Y.; Gorry, M.C.; Hart, P.S.; Cooper, M.; Marazita, M.L.; Marks, J.M.; Cortelli, J.R.; Pallos, D. A mutation in the SOS1 gene causes hereditary gingival fibromatosis type 1. Am. J. Hum. Genet. 2002, 70, 943–954. [Google Scholar] [CrossRef] [PubMed]
- Bayram, Y.; White, J.J.; Elcioglu, N.; Cho, M.T.; Zadeh, N.; Gedikbasi, A.; Palanduz, S.; Ozturk, S.; Cefle, K.; Kasapcopur, O.; et al. REST Final-Exon-Truncating Mutations Cause Hereditary Gingival Fibromatosis. Am. J. Hum. Genet. 2017, 101, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Machado, R.A.; de Andrade, R.S.; Pêgo, S.P.B.; Krepischi, A.C.V.; Coletta, R.D.; Martelli-Júnior, H. New evidence of genetic heterogeneity causing hereditary gingival fibromatosis and ALK and CD36 as new candidate genes. J. Periodontol. 2023, 94, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Chen, D.; Huang, H.; Luo, N.; Chen, H.; Zhao, J.; Wang, Y.; Zhao, T.; Huang, S.; Ren, Y.; et al. A novel gene ZNF862 causes hereditary gingival fibromatosis. eLife 2022, 11, e66646. [Google Scholar] [CrossRef] [PubMed]
- Sume, S.S.; Kantarci, A.; Lee, A.; Hasturk, H.; Trackman, P.C. Epithelial to mesenchymal transition in gingival overgrowth. Am. J. Pathol. 2010, 177, 208–218. [Google Scholar] [CrossRef]
- Lee, J.M.; Dedhar, S.; Kalluri, R.; Thompson, E.W. The epithelial-mesenchymal transition: New insights in signaling, development, and disease. J. Cell Biol. 2006, 172, 973–981. [Google Scholar] [CrossRef]
- Yang, F.; Lu, J.; Yu, Y.; Gong, Y. Epithelial to mesenchymal transition in Cyclosporine A-induced rat gingival overgrowth. Arch. Oral Biol. 2017, 81, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Jumper, J.; Evans, R.; Pritzel, A.; Green, T.; Figurnov, M.; Ronneberger, O.; Tunyasuvunakool, K.; Bates, R.; Žídek, A.; Potapenko, A.; et al. Highly accurate protein structure prediction with AlphaFold. Nature 2021, 596, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Parkin, B.; Law, C. Axenfeld anomaly and retinal changes in Ramon syndrome: Follow-up of two sibs. Am. J. Med. Genet. 2001, 104, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Surej Kumar, L.K.; Deepa, D.S.; Dilna, S. Ramon Syndrome- A Rare Form of Cherubism. Ann. Maxillofac. Surg. 2019, 9, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Stenmark, H. Rab GTPases as coordinators of vesicle traffic. Nat. Rev. Mol. Cell Biol. 2009, 10, 513–525. [Google Scholar] [CrossRef] [PubMed]
- Wei, D.; Zhan, W.; Gao, Y.; Huang, L.; Gong, R.; Wang, W.; Zhang, R.; Wu, Y.; Gao, S.; Kang, T. RAB31 marks and controls an ESCRT-independent exosome pathway. Cell Res. 2021, 31, 157–177. [Google Scholar] [CrossRef] [PubMed]
- Margiotta, A.; Bucci, C. Coordination between Rac1 and Rab Proteins: Functional Implications in Health and Disease. Cells 2019, 8, 396. [Google Scholar] [CrossRef]
- Gillingham, A.K.; Bertram, J.; Begum, F.; Munro, S. In vivo identification of GTPase interactors by mitochondrial relocalization and proximity biotinylation. eLife 2019, 8, e45916. [Google Scholar] [CrossRef] [PubMed]
- Manshouri, R.; Coyaud, E.; Kundu, S.T.; Peng, D.H.; Stratton, S.A.; Alton, K.; Bajaj, R.; Fradette, J.J.; Minelli, R.; Peoples, M.D.; et al. ZEB1/NuRD complex suppresses TBC1D2b to stimulate E-cadherin internalization and promote metastasis in lung cancer. Nat. Commun. 2019, 10, 5125. [Google Scholar] [CrossRef]
- Zhang, W.; Liu, H.T. MAPK signal pathways in the regulation of cell proliferation in mammalian cells. Cell Res. 2002, 12, 9–18. [Google Scholar] [CrossRef]
- Melchionna, R.; Trono, P.; Tocci, A.; Nisticò, P. Actin Cytoskeleton and Regulation of TGFβ Signaling: Exploring Their Links. Biomolecules 2021, 11, 336. [Google Scholar] [CrossRef] [PubMed]
- Bosco, E.E.; Mulloy, J.C.; Zheng, Y. Rac1 GTPase: A “Rac” of all trades. Cell Mol. Life Sci. 2009, 66, 370–374. [Google Scholar] [CrossRef]
- Ganesh, P.R. Immunoexpression of interleukin-6 in drug-induced gingival overgrowth patients. Contemp. Clin. Dent. 2016, 7, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Trackman, P.C.; Kantarci, A. Molecular and clinical aspects of drug-induced gingival overgrowth. J. Dent. Res. 2015, 94, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Leguit, R.J.; Raymakers, R.A.P.; Hebeda, K.M.; Goldschmeding, R. CCN2 (Cellular Communication Network factor 2) in the bone marrow microenvironment, normal and malignant hematopoiesis. J. Cell Commun. Signal 2021, 15, 25–56. [Google Scholar] [CrossRef] [PubMed]
- Saito, K.; Mori, S.; Tanda, N.; Sakamoto, S. Immunolocalizaiton of c-Myc and bcl-2 proto-oncogene products in gingival hyperplasia induced by nifedipine and phenytoin. J. Periodontol. 2000, 71, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Handajani, J.; Santoso, A.L.; Haniastuti, T.; Utoro, T.; Sosroseno, W. Effect of nifedipine on the expression of bcl-2 protein in rat gingiva. Clin. Oral Investig. 2003, 7, 56–58. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.P.; Chen, Y.T.; Fu, E.; Shen, E.C.; Wu, M.H.; Chen, Y.L.; Chiang, C.Y.; Chiu, H.C. Cyclosporine A enhances gingival β-catenin stability via Wnt signaling. J. Periodontol. 2015, 86, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.P.; Chen, Y.T.; Shieh, Y.S.; Chin, Y.T.; Huang, R.Y.; Yang, S.F.; Gau, C.H.; Fu, E. Cyclosporin-induced downregulation of the expression of E-cadherin during proliferation of edentulous gingival epithelium in rats. J. Periodontol. 2006, 77, 832–839. [Google Scholar] [CrossRef]
- Park, S.Y.; Jin, W.; Woo, J.R.; Shoelson, S.E. Crystal structures of human TBC1D1 and TBC1D4 (AS160) RabGTPase-activating protein (RabGAP) domains reveal critical elements for GLUT4 translocation. J. Biol. Chem. 2011, 286, 18130–18138. [Google Scholar] [CrossRef]
- Schulze, J.; Seitz, S.; Saito, H.; Schneebauer, M.; Marshall, R.P.; Baranowsky, A.; Busse, B.; Schilling, A.F.; Friedrich, F.W.; Albers, J.; et al. Negative regulation of bone formation by the transmembrane Wnt antagonist Kremen-2. PLoS ONE 2010, 5, e10309. [Google Scholar] [CrossRef]
- Mao, B.; Niehrs, C. Kremen2 modulates Dickkopf2 activity during Wnt/LRP6 signaling. Gene 2003, 302, 179–183. [Google Scholar] [CrossRef]
- Martínez-Gil, N.; Ugartondo, N.; Grinberg, D.; Balcells, S. Wnt Pathway Extracellular Components and Their Essential Roles in Bone Homeostasis. Genes 2022, 13, 138. [Google Scholar] [CrossRef]
- Chen, B.; Wang, S.Q.; Huang, J.; Xu, W.; Lv, H.; Nie, C.; Wang, J.; Zhao, H.; Liu, Y.; Li, J.; et al. Knockdown of Kremen2 Inhibits Tumor Growth and Migration in Gastric Cancer. Front. Oncol. 2020, 10, 534095. [Google Scholar] [CrossRef]
- Long, J.; Cong, F.; Wei, Y.; Liu, J.; Tang, W. Increased Kremen2 predicts worse prognosis in colon cancer. Pathol. Oncol. Res. 2023, 29, 1611082. [Google Scholar] [CrossRef] [PubMed]
- Deltas, C. Digenic inheritance and genetic modifiers. Clin. Genet. 2018, 93, 429–438. [Google Scholar] [CrossRef]
- Ueki, Y.; Tiziani, V.; Santanna, C.; Fukai, N.; Maulik, C.; Garfinkle, J.; Ninomiya, C.; doAmaral, C.; Peters, H.; Habal, M.; et al. Mutations in the gene encoding c-Abl-binding protein SH3BP2 cause cherubism. Nat. Genet. 2001, 28, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Reichenberger, E.J.; Levine, M.A.; Olsen, B.R.; Papadaki, M.E.; Lietman, S.A. The role of SH3BP2 in the pathophysiology of cherubism. Orphanet J. Rare Dis. 2012, 7, S5. [Google Scholar] [CrossRef] [PubMed]
- Teitelbaum, S.L. The osteoclast and its unique cytoskeleton. Ann. N. Y. Acad. Sci. 2011, 1240, 14–17. [Google Scholar] [CrossRef]
- Croke, M.; Ross, F.P.; Korhonen, M.; Williams, D.A.; Zou, W.; Teitelbaum, S.L. Rac deletion in osteoclasts causes severe osteopetrosis. J. Cell Sci. 2011, 124, 3811–3821. [Google Scholar] [CrossRef]
- Boyce, B.F.; Xiu, Y.; Li, J.; Xing, L.; Yao, Z. NF-κB-Mediated Regulation of Osteoclastogenesis. Endocrinol. Metab. 2015, 30, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Colón-Ramos, D.A. Synapse formation in developing neural circuits. Curr. Top. Dev. Biol. 2009, 87, 53–79. [Google Scholar] [CrossRef]
- Iroegbu, J.D.; Ijomone, O.K.; Femi-Akinlosotu, O.M.; Ijomone, O.M. ERK/MAPK signalling in the developing brain: Perturbations and consequences. Neurosci. Biobehav. Rev. 2021, 131, 792–805. [Google Scholar] [CrossRef] [PubMed]
- Redman, R.S.; Ward, C.C.; Patterson, R.H. Focus of epithelial dysplasia arising in hereditary gingival fibromatosis. J. Periodontol. 1985, 56, 158–162. [Google Scholar] [CrossRef]
- Kantarci, A.; Nseir, Z.; Kim, Y.S.; Sume, S.S.; Trackman, P.C. Loss of basement membrane integrity in human gingival overgrowth. J. Dent. Res. 2011, 90, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.P. Gingival Abnormalities of Genetic Origin: A Preliminary Communication with Special Reference to Hereditary Generalized Gingival Fibromatosis. J. Dent. Res. 1966, 45, 597–612. [Google Scholar] [CrossRef]
- Becker, W.; Collings, C.K.; Zimmerman, E.R.; De la Rosa, M.; Singdahlsen, D. Hereditary gingival fibromatosis. Oral Surg. Oral Med. Oral Pathol. 1967, 24, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Cuestas-Carnero, R.; Bornancini, C.A. Hereditary generalized gingival fibromatosis associated with hypertrichosis: Report of five cases in one family. J. Oral Maxillofac. Surg. 1988, 46, 415–420. [Google Scholar] [CrossRef]
- Gawron, K.; Łazarz-Bartyzel, K.; Kowalska, A.; Bereta, G.; Nowakowska, Z.; Plakwicz, P.; Potempa, J.; Fertala, A.; Chomyszyn-Gajewska, M. Fibroblasts from recurrent fibrotic overgrowths reveal high rate of proliferation in vitro-findings from the study of hereditary and idiopathic gingival fibromatosis. Connect. Tissue Res. 2019, 60, 29–39. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Families | Patients | Phenotypes | Clinical Findings | Variants | Prediction/Ranking |
|---|---|---|---|---|---|
| 1 | 1 (Female) | Ramon Syndrome | Gingival fibromatosis, cherubism-like lesions, a persistent open anterior fontanelle, focal epilepsy, left eye amblyopia | TBC1D2B variant NM_144572.2; NP_653173.1 c.1879_1880del p.Glu627LysfsTer61 chr 15-78305554-TTC-T Novel | MutationTaster: Disease causing Prob = 1 PolyPhen-2: N/A SIFT: Damaging; score = 0.858 CADD: N/A DANN: N/A Varsome: N/A |
| 2 | 2 (Male) | Hereditary gingival fibromatosis | Gingival fibromatosis | TBC1D2B variant NM_144572.2; NP_653173.1 c.2471A>G p.Tyr824Cys chr 15-78295750-T-C rs199928887 MAF = 0.00001301 KREMEN2 variant NM_172229.3; NP_757384.1 c.892C>T p.Arg298Cys chr 16-3017162-C-T Novel | MutationTaster: Disease causing Prob = 0.999153978449563 PolyPhen-2: Probably damaging; score = 0.999 SIFT: Damaging; score = 0.01 CADD score = 22.8 DANN score = 0.9935 Varsome: Uncertain Significance MutationTaster: Disease causing Prob = 0.876965507429932 PolyPhen-2: Probably damaging; score = 0.994 SIFT: Tolerated; score = 0.18 CADD score = 23.5 1 DANN score = 0.9981 2 Varsome: Uncertain significance |
| 3 (Male) | Hereditary gingival fibromatosis | Gingival fibromatosis, epithelial dysplasia, dense mandibular bone | |||
| 4 (Male) | Hereditary gingival fibromatosis | Gingival fibromatosis, dense mandibular bone |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kularbkaew, T.; Thongmak, T.; Sandeth, P.; Daroontum, T.; Durward, C.S.; Vittayakittipong, P.; Duke, P.; Iamaroon, A.; Kintarak, S.; Intachai, W.; et al. Genetic Variants in the TBC1D2B Gene Are Associated with Ramon Syndrome and Hereditary Gingival Fibromatosis. Int. J. Mol. Sci. 2024, 25, 8867. https://doi.org/10.3390/ijms25168867
Kularbkaew T, Thongmak T, Sandeth P, Daroontum T, Durward CS, Vittayakittipong P, Duke P, Iamaroon A, Kintarak S, Intachai W, et al. Genetic Variants in the TBC1D2B Gene Are Associated with Ramon Syndrome and Hereditary Gingival Fibromatosis. International Journal of Molecular Sciences. 2024; 25(16):8867. https://doi.org/10.3390/ijms25168867
Chicago/Turabian StyleKularbkaew, Thatphicha, Tipaporn Thongmak, Phan Sandeth, Teerada Daroontum, Callum S. Durward, Pichai Vittayakittipong, Paul Duke, Anak Iamaroon, Sompid Kintarak, Worrachet Intachai, and et al. 2024. "Genetic Variants in the TBC1D2B Gene Are Associated with Ramon Syndrome and Hereditary Gingival Fibromatosis" International Journal of Molecular Sciences 25, no. 16: 8867. https://doi.org/10.3390/ijms25168867
APA StyleKularbkaew, T., Thongmak, T., Sandeth, P., Daroontum, T., Durward, C. S., Vittayakittipong, P., Duke, P., Iamaroon, A., Kintarak, S., Intachai, W., Ngamphiw, C., Tongsima, S., Jatooratthawichot, P., Cox, T. C., Ketudat Cairns, J. R., & Kantaputra, P. (2024). Genetic Variants in the TBC1D2B Gene Are Associated with Ramon Syndrome and Hereditary Gingival Fibromatosis. International Journal of Molecular Sciences, 25(16), 8867. https://doi.org/10.3390/ijms25168867