
Systematic Review and Meta-Analysis on Optimal Timing of Surgery for Acute Symptomatic Metastatic Spinal Cord Compression
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
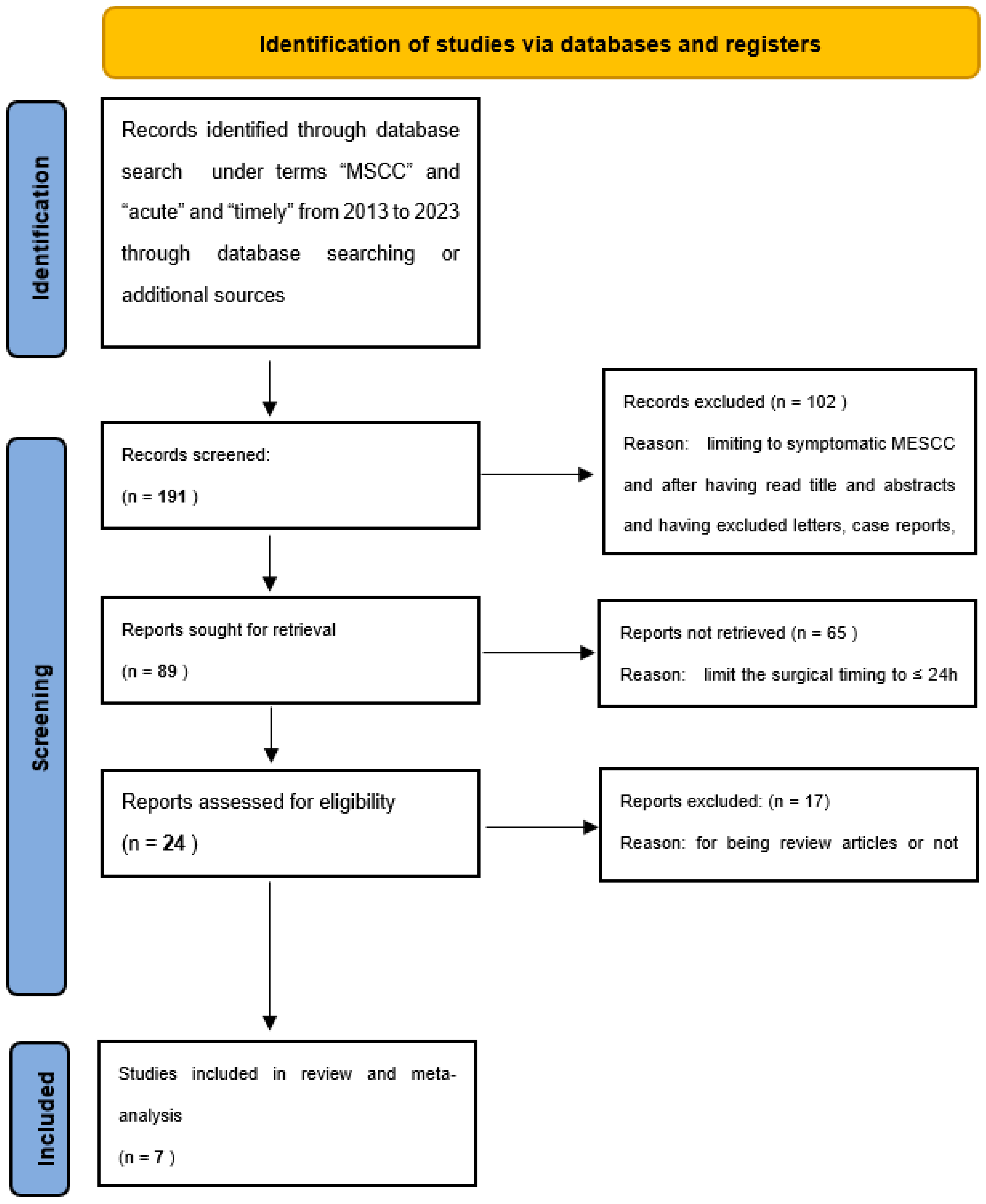
2.1. Meta-Analysis Study Selection Process
“What are the rates of improved outcomes and adverse events rates for different timing of palliative surgery for acute symptomatic MSCC?”
- Adequate cohort assessment:
- -
- Age ≥ 18 years;
- -
- Patients with solid neoplasms with a known or unknown primary tumor;
- -
- Studies with contrast-enhanced spine magnetic resonance (MRI) and spine computer tomography (CT);
- -
- Patients with neurological impairment at admission (i.e., Frankel grade A to D and ASIA grade A to D);
- -
- Patients with >3 months of survival;
- -
- Decompressive/palliative surgery with or without posterior screw fixation.
- Outcome assessment:
- Adequate number of patients and timing:
- -
- Studies with patients with MSCC symptoms from 0 to 72 h.
- -
- Studies reporting outcomes based on timing of surgery from the beginning of symptoms as ≤24 h, >24 h, ≤48 h, and >48 h.
- -
- Minimum > 25 consecutive patients.
2.2. Evaluation of Methodological Quality for the Meta-Analysis
- Did the study include all or consecutive patients with adequate clinical follow-up?
- Was the outcome assessment objective and replicable?
- Was the sample size enough to draw valid statistical and clinical predictions?
2.3. Statistical Analysis
3. Results
Outcomes and Adverse Events
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DiSibio, G.; French, S.W. Metastatic Patterns of Cancers. Arch. Pathol. Lab. Med. 2008, 132, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Eleraky, M.; Papanastassiou, I.; Vrionis, F.D. Management of Metastatic Spine Disease. Curr. Opin. Support. Palliat. Care 2010, 4, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Maccauro, G.; Spinelli, M.S.; Mauro, S.; Perisano, C.; Graci, C.; Rosa, M.A. Physiopathology of Spine Metastasis. Int. J. Surg. Oncol. 2011, 2011, 107969. [Google Scholar] [CrossRef] [PubMed]
- Boussios, S.; Cooke, D.; Hayward, C.; Kanellos, F.S.; Tsiouris, A.K.; Chatziantoniou, A.A.; Zakynthinakis-Kyriakou, N.; Karathanasi, A. Metastatic Spinal Cord Compression: Unraveling the Diagnostic and Therapeutic Challenges. Anticancer. Res. 2018, 38, 4987–4997. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.S.; Patchell, R.A. Metastatic Epidural Spinal Cord Compression. Lancet Neurol. 2008, 7, 459–466. [Google Scholar] [CrossRef]
- Guzik, G. Analysis of Factors Delaying the Surgical Treatment of Patients with Neurological Deficits in the Course of Spinal Metastatic Disease. BMC Palliat. Care 2018, 17, 44. [Google Scholar] [CrossRef] [PubMed]
- Spratt, D.E.; Beeler, W.H.; de Moraes, F.Y.; Rhines, L.D.; Gemmete, J.J.; Chaudhary, N.; Shultz, D.B.; Smith, S.R.; Berlin, A.; Dahele, M.; et al. An Integrated Multidisciplinary Algorithm for the Management of Spinal Metastases: An International Spine Oncology Consortium Report. Lancet Oncol. 2017, 18, e720–e730. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Nadarajah, J.; Kumar, A.; Gamanagatti, S. Misery of Neurosurgeon: Gauzoma Causing Foreign Body Granuloma-Role of Radiologist. Asian J. Neurosurg. 2016, 11, 99–104. [Google Scholar] [CrossRef]
- Nater, A.; Chuang, J.; Liu, K.; Quraishi, N.A.; Pasku, D.; Wilson, J.R.; Fehlings, M.G. A Personalized Medicine Approach for the Management of Spinal Metastases with Cord Compression: Development of a Novel Clinical Prediction Model for Postoperative Survival and Quality of Life. World Neurosurg. 2020, 140, 654–663.e13. [Google Scholar] [CrossRef]
- Kuah, T.; Vellayappan, B.A.; Makmur, A.; Nair, S.; Song, J.; Tan, J.H.; Kumar, N.; Quek, S.T.; Hallinan, J.T.P.D. State-of-the-Art Imaging Techniques in Metastatic Spinal Cord Compression. Cancers 2022, 14, 3289. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, C.S.; Badhiwala, J.H.; Fehlings, M.G. “Time Is Spine”: The Importance of Early Intervention for Traumatic Spinal Cord Injury. Spinal Cord 2020, 58, 1037–1039. [Google Scholar] [CrossRef] [PubMed]
- Meyer, H.S.; Wagner, A.; Raufer, A.; Joerger, A.K.; Gempt, J.; Meyer, B. Surgery in Acute Metastatic Spinal Cord Compression: Timing and Functional Outcome. Cancers 2022, 14, 2249. [Google Scholar] [CrossRef]
- Younsi, A.; Riemann, L.; Ishak, B.; Scherer, M.; Unterberg, A.W.; Zweckberger, K. Feasibility of Salvage Decompressive Surgery for Pending Paralysis Due to Metastatic Spinal Cord Compression. Clin. Neurol. Neurosurg. 2021, 202, 106509. [Google Scholar] [CrossRef]
- Younsi, A.; Riemann, L.; Scherer, M.; Unterberg, A.; Zweckberger, K. Impact of Decompressive Laminectomy on the Functional Outcome of Patients with Metastatic Spinal Cord Compression and Neurological Impairment. Clin. Exp. Metastasis 2020, 37, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Tateiwa, D.; Oshima, K.; Nakai, T.; Imura, Y.; Tanaka, T.; Outani, H.; Tamiya, H.; Araki, N.; Naka, N. Clinical Outcomes and Significant Factors in the Survival Rate after Decompression Surgery for Patients Who Were Non-Ambulatory Due to Spinal Metastases. J. Orthop. Sci. 2019, 24, 347–352. [Google Scholar] [CrossRef]
- Lo, W.Y.; Yang, S.H. Metastatic Spinal Cord Compression (MSCC) Treated with Palliative Decompression: Surgical Timing and Survival Rate. PLoS ONE 2017, 12, e0190342. [Google Scholar] [CrossRef]
- Fan, Y.; Zhou, X.; Wang, H.; Jiang, P.; Cai, S.; Zhang, J.; Liu, Y. The Timing of Surgical Intervention in the Treatment of Complete Motor Paralysis in Patients with Spinal Metastasis. Eur. Spine J. 2016, 25, 4060–4066. [Google Scholar] [CrossRef]
- Quraishi, N.A.; Rajagopal, T.S.; Manoharan, S.R.; Elsayed, S.; Edwards, K.L.; Boszczyk, B.M. Effect of Timing of Surgery on Neurological Outcome and Survival in Metastatic Spinal Cord Compression. Eur. Spine J. 2013, 22, 1383–1388. [Google Scholar] [CrossRef]
- DerSimonian, R.; Kacker, R. Random-Effects Model for Meta-Analysis of Clinical Trials: An Update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Igoumenou, V.G.; Mavrogenis, A.F.; Angelini, A.; Baracco, R.; Benzakour, A.; Benzakour, T.; Bork, M.; Vazifehdan, F.; Nena, U.; Ruggieri, P. Complications of Spine Surgery for Metastasis. Eur. J. Orthop. Surg. Traumatol. Orthop. Traumatol. 2020, 30, 37–56. [Google Scholar] [CrossRef] [PubMed]
- Esperança-Martins, M.; Roque, D.; Barroso, T.; Abrunhosa-Branquinho, A.; Belo, D.; Simas, N.; Costa, L. Multidisciplinary Approach to Spinal Metastases and Metastatic Spinal Cord Compression-A New Integrative Flowchart for Patient Management. Cancers 2023, 15, 1796. [Google Scholar] [CrossRef] [PubMed]
- Schiff, D.; O’Neill, B.P.; Suman, V.J. Spinal Epidural Metastasis as the Initial Manifestation of Malignancy: Clinical Features and Diagnostic Approach. Neurology 1997, 49, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Douglas, S.; Huttenlocher, S.; Bajrovic, A.; Rudat, V.; Schild, S.E.; Rades, D. Prognostic Factors for Different Outcomes in Patients with Metastatic Spinal Cord Compression from Cancer of Unknown Primary. BMC Cancer 2012, 12, 261. [Google Scholar] [CrossRef]
- Compagnone, D.; Cecchinato, R.; Pezzi, A.; Langella, F.; Damilano, M.; Redaelli, A.; Vanni, D.; Lamartina, C.; Berjano, P.; Boriani, S. Diagnostic Approach and Differences between Spinal Infections and Tumors. Diagnostics 2023, 13, 2737. [Google Scholar] [CrossRef] [PubMed]
- George, R.; Jeba, J.; Ramkumar, G.; Chacko, A.G.; Leng, M.; Tharyan, P. Interventions for the Treatment of Metastatic Extradural Spinal Cord Compression in Adults. Cochrane Database Syst. Rev. 2015, 9, CD006716. [Google Scholar] [CrossRef]
- Patchell, R.A.; Tibbs, P.A.; Regine, W.F.; Payne, R.; Saris, S.; Kryscio, R.J.; Mohiuddin, M.; Young, B. Direct Decompressive Surgical Resection in the Treatment of Spinal Cord Compression Caused by Metastatic Cancer: A Randomised Trial. Lancet 2005, 366, 643–648. [Google Scholar] [CrossRef]


{kind=link}
| Risk of Bias Domains | ||||||
|---|---|---|---|---|---|---|
| Study | D1 | D2 | D3 | D4 | D5 | Overall |
| Meyer H et al., 2022 [13] |  | | | | |  |
| Younsi A et al., 2021 [14] | | | |  | | |
| Younsi A et al., 2020 [15] | | | | | | |
| Tateiwa D et al., 2019 [16] | | | | | | |
| Lo WY et al., 2017 [17] | | | | | | |
| Fan Y et al., 2016 [18] | | | | | | |
| Quraishi NA et al., 2013 [19] | | | | | | |
| Title | Author, Year | Journal | Recruitment | Country | Design | Cohort | Outcomes Scale | Numbers of Patients | Timing |
|---|---|---|---|---|---|---|---|---|---|
| Surgery in Acute Metastatic Spinal Cord Compression: Timing and Functional Outcome [13] | Meyer H et al., 2022 | Cancers | 2007–2019 | Germany | Retro | Acute symptomatic MSCC, solid tumors, palliative surgery | ASIA score | 46 | ≤24 h |
| Feasibility of salvage decompressive surgery for pending paralysis due to metastatic spinal cord compression [14] | Younsi A et al., 2021 | Clinical Neurology and Neurosurgery | 2004–2014 | Germany | Retro | Acute symptomatic MSCC, solid tumors, palliative surgery | FRANKEL score | 28 | ≤24 h |
| Impact of decompressive laminectomy on the functional outcome of patients with metastatic spinal cord compression and neurological impairment [15] | Younsi A et al., 2020 | Clinical & Experimental Metastasis | 2004–2014 | Germany | Retro | Acute symptomatic MSCC, solid tumors, palliative surgery | FRANKEL score | 101 | ≤48 h; >24 h |
| Clinical outcomes and significant factors in the survival rate after decompression surgery for patients who were non-ambulatory due to spinal metastases [16] | Tateiwa D et al., 2019 | Journal of Orthopedic Science | 2011–2016 | Japan | Retro | Acute symptomatic MSCC, solid tumors, palliative surgery | FRANKEL score | 31 | ≤48 h; >48 h |
| Metastatic spinal cord compression (MSCC) treated with palliative decompression: Surgical timing and survival rate [17] | Lo WY et al., 2017 | Plos One | 2012–2016 | Taiwan | Retro | Acute symptomatic MSCC, solid tumors, palliative surgery | FRANKEL score | 52 | ≤48 h; >48 h |
| The timing of surgical intervention in the treatment of complete motor paralysis in patients with spinal metastasis [18] | Fan Y et al., 2016 | Eur Spine J | 2007–2014 | China | Retro | Acute symptomatic MSCC, solid tumors, palliative surgery | FRANKEL score | 33 | ≤48 h; >48 h |
| Effect of timing of surgery on neurological outcome and survival in metastatic spinal cord compression [19] | Quraishi NA et al., 2013 | Eur Spine J | 2005–2010 | United Kingdom | Retro | Acute symptomatic MSCC, solid tumors, palliative surgery | FRANKEL score | 166 | ≤24 h ≤48 h; >48 h |
| Overall | ≤24 h | >24 h | ≤48 h | >48 h | |
|---|---|---|---|---|---|
| Patient N° | 538 | 270 | 212 | 222 | 197 |
| IMPROVED NEUROLOGICAL DEFICIT % (95% CI) | 56.4 (35.0–77.6) | 41.3 (20.4–63.6) | 32.2 (12.4–55.8) | 83.0 (59.0–98.2) | 36.8 (12.2–65.4) |
| COMPLICATIONS % (95% CI) | 19.8 (5.1–40.3) | 25.5 (15.9–36.3) | 28.6 (19.5–38.8) | 21.0 (1.8–51.4) | 28.6 (19.5–38.8) |
| WOUND DEHISCENCE/DISCITIS % (95% CI) | 6.5 (1.2–15.0) | 7.1 (1.9–10.0) | 9.6 (1.8–21.2) | 7.9 (0.5–20.8) | 16.1 (9.3–24.3) |
| EPIDURAL HEMATOMA % (95% CI) | 1.2 (0.0–3.5) | 3.6 (0.6–17.7) | / | 1.7 (0.0–5.5) | 0.0 (0.0–3.6) |
| REOPERATION % (95% CI) | 1.4 (0.0–4.4) | / | / | 1.8 (0.0–5.4) | / |
| 30 days MORTALITY % (95% CI) | 0.1 (0.0–0.9) | / | 0.1 (0.0–21.5) | 0.1 (0.0–3.0) | / |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bresolin, N.; Sartori, L.; Drago, G.; Pastorello, G.; Gallinaro, P.; Del Verme, J.; Zanata, R.; Giordan, E. Systematic Review and Meta-Analysis on Optimal Timing of Surgery for Acute Symptomatic Metastatic Spinal Cord Compression. Medicina 2024, 60, 631. https://doi.org/10.3390/medicina60040631
Bresolin N, Sartori L, Drago G, Pastorello G, Gallinaro P, Del Verme J, Zanata R, Giordan E. Systematic Review and Meta-Analysis on Optimal Timing of Surgery for Acute Symptomatic Metastatic Spinal Cord Compression. Medicina. 2024; 60(4):631. https://doi.org/10.3390/medicina60040631
Chicago/Turabian StyleBresolin, Nicola, Luca Sartori, Giacomo Drago, Giulia Pastorello, Paolo Gallinaro, Jacopo Del Verme, Roberto Zanata, and Enrico Giordan. 2024. "Systematic Review and Meta-Analysis on Optimal Timing of Surgery for Acute Symptomatic Metastatic Spinal Cord Compression" Medicina 60, no. 4: 631. https://doi.org/10.3390/medicina60040631