Simple Summary
TNF-α inhibitors are widely prescribed immunosuppressive medications for multiple chronic inflammatory disorders. Chronic immunosuppression can lead to malignancy due to decreased immune surveillance, but TNF-α inhibitors have been found to be largely safe aside from the development of non-melanoma skin cancer. However, these studies all have short-term follow-up, rely on spontaneous reporting systems, and investigate a disease or drug subset. Previous meta-analyses similarly have investigated either interventional or observational studies only. Here, we reviewed over 17,000 abstracts with the most stringent inclusion criteria in the published literature to analyze 46 interventional studies and 10 observational studies for malignancy risk in patients exposed to TNF-α inhibitors. Using patient-level data, our findings for both interventional and observational studies found no statistically significant increased risk of malignancy but with poor quality of adverse event reporting. This is the most comprehensive and up-to-date meta-analysis and underscores the need for high-quality studies with a longer follow-up of these patients.
Abstract
Background/Objectives: Tumor necrosis factor-alpha inhibitors (TNF-I) are widely prescribed for chronic inflammatory conditions. Prior studies of TNF-I use and malignancy risk have not demonstrated consistent associations outside non-melanoma skin cancers. We performed an updated systematic review and meta-analysis of interventional and observational studies to investigate this potential relationship. Methods: We searched MEDLINE, EMBASE, CENTRAL Register, Cochrane Library, and Scopus for studies published between 1996 and 2020. Two observers independently extracted the data; differences were resolved by consensus. Candidate studies were classified as interventional or observational per study design. A random-effects meta-analysis estimated malignancy rate ratios (MRRs) for cancers in TNF-I-exposed patients. Forest plots used a standard rate scale, and funnel plots used a random-effects model to assess for publication bias. Results: 45 interventional studies contributing 22,652 patients and 10 observational studies contributing 34,866 patients met the meta-analysis inclusion criteria. The plurality of these studies focused on adalimumab for both interventional (38%) and observational (50%) studies. TNF-I exposure was not associated with overall cancer risk in interventional (RR = 1.04, 95% CI 0.71–1.51) or observational studies (RR = 1.42, 95% CI 0.72–2.79). In total, 9/45 (20%) interventional studies and 0/10 (0%) observational studies had adequate quality of adverse event reporting, and 52/55 (95%) had either industry or unknown funding sources. Conclusions: Our synthesis of published findings from interventional and observational studies had inconclusive evidence on TNF-I exposure and cancer risk. Given the small number of studies designed to investigate malignancy risk, the low number of studies with adequate adverse event reporting, and the high number of industry-funded studies, it suggests that higher quality prospective studies are warranted to investigate the risk of malignancy for patients on chronic TNF-I.
Keywords:
meta-analysis; cancer; TNF-alpha; adalimumab; infliximab; etanercept; certolizumab; golimumab 1. Introduction
Over the last two decades, tumor necrosis factor-alpha inhibitors (TNF-Is) have become standard therapies for chronic inflammatory disorders, with an ongoing expansion of indications and off-label applications [1]. Presently, five TNF-Is have been approved by the U.S. Food and Drug Administration (FDA) for the treatment of inflammatory conditions: Adalimumab (ADA) and golimumab (GLM) are fully humanized monoclonal tumor necrosis factor-alpha (TNF-α) IgG1 antibodies, infliximab (INX) is a mouse/human chimeric monoclonal TNF-α IgG1, certolizumab pegol (CTZ) is a PEGylated Fab’ fragment of a TNF-α monoclonal antibody, and etanercept (ETN) is a fusion protein of the human tumor necrosis factor receptor II extracellular domain and the IgG1 Fc region [2]. The wide-ranging and effective use of these medications is typified by the status of adalimumab—the most profitable drug worldwide for much of the past decade [3,4,5]. Though their structures and exact functions vary [6], these agents all inhibit the binding of soluble TNF-α to its receptor [2], inhibiting the downstream production of pro-inflammatory cytokines and chemokines, the upregulation of adhesion molecules, and the activation of peripheral blood mononuclear cells [1]. Concurrent with the roles of chronic inflammation in promoting carcinogenesis [7] and of immune activation in clearing malignant cells, it remains unclear whether TNF-α exerts tumorigenic or anti-neoplastic activity, or both depending on the host immunologic context [8,9,10].
Multiple groups have evaluated the relationship between TNF-I exposure and malignancies. The strongest data are those associating TNF-I use with non-melanoma skin cancers (NMSCs), for which institutional cohort studies [11], registry-based studies [12,13,14], and meta-analyses [15,16,17] have demonstrated an increased risk. Some reports have suggested a higher incidence of lymphomas in patients taking TNF-I [12,18,19,20,21]; however, these analyses were potentially confounded by associations with underlying disease states and other medication use [10,22], and their findings have largely been outweighed by several studies in diverse populations demonstrating no increased risk [23,24,25,26,27,28,29]. For patients with pre-existing malignancies, current clinical practice states that biologic therapy, such as that with TNF-I, is not absolutely contraindicated and must be approached on a case-by-case basis with the patient [30].
TNF-I use is frequently presumed to have no influence on the development of other malignancies, as demonstrated by the results of multiple clinical trials, registry-based studies, and meta-analyses conducted over the last decade [17,27,31,32,33,34,35]. However, these studies have key limitations—most clinical trials of TNF-I were primarily designed to assess drug efficacy, and many co-administered medications such as methotrexate and were not powered specifically to detect incident malignancies [36]. Studies drawing from administrative databases rely on spontaneous adverse event reporting and algorithms for identifying malignancies, which risks underestimating overall cancer incidence, false positives, and bias from the systematic misclassification of suspected cases [37]. Existing meta-analyses incorporate these limitations of primary studies and have been constrained in evaluating only specific subsets of approved TNF-I [17,38], single malignancy types [16], second malignancies [35] or specific inflammatory disease states [15,16,31,32,33,34,35,38]. These meta-analyses have been further restricted to include only investigator-controlled interventional studies [17,31,32,33,34] or observational registry-based analyses [27]. In parallel, data from the FDA Adverse Events Reporting System describe cancers associated with TNF-I use in excess of the subset reported in the scientific literature [39], suggesting a potentially unappreciated relationship.
Given the limitations of current meta-analyses, we sought to comprehensively evaluate associations between all approved TNF-Is and the development of malignancies. In this work, we systematically review contemporary interventional and observational studies and perform meta-analyses on these two groups of studies. To the extent of our knowledge, this is the broadest attempt to evaluate the relationship between TNF-I and incident malignancies to date.
2. Materials and Methods
2.1. Relevant Publication Search
We searched MEDLINE for studies published between January 1996 and January 2020 evaluating approved TNF-I using the medical subject headings (MeSH) “TNF-alpha Inhibitors”, “adalimumab”, “certolizumab”, “etanercept”, “golimumab”, “infliximab”, “safety”, “side effects”, “toxicity”, “neoplasms”, “cancer”, “malignan*”, “adverse”, “longitudinal studies”, “short term”, and “long term”. We also searched using keywords for TNF-I trade names. We searched ClinicalTrials.gov using the keywords “TNF-alpha Inhibitors” and each of the five individual drug names. We replicated this search process in EMBASE (Elsevier), the CENTRAL Register of Controlled Trials (Wiley), the Cochrane Library (Wiley), Scopus (Elsevier), and the gray literature sources. The full search strategy, using infliximab as an example, is reproduced in the Supplementary Methods.
2.2. Inclusion and Exclusion Criteria
Criteria for inclusion in the meta-analysis were as follows: (1) Clinical trials or population-based observational studies of TNF-I approved for use in the United States, Europe, or Asia. (2) Presence of a safety analysis delineated by individual TNF-I. (3) Use of a TNF-I in a systemically absorbed formulation, such as intravenous or subcutaneous. The two medications administered intravenously are INX (3 mg/kg every 8 weeks) and GLM (100 mg every 4 weeks after induction) are administered intravenously. The three medications administered subcutaneously are ADA (40 mg every other week), ETN (total of 50 mg weekly), and CTZ (total of 400 mg every 4 weeks after induction).
Exclusion criteria were as follows: (1) Non-experimental study design—practice updates, expert opinions, letters, abstracts, case series, or case reports. (2) Publication in a language other than English. (3) Studies conducted on non-human subjects. (4) Analyses focusing on a single non-malignancy adverse event (i.e., tuberculosis). (5) Studies not performed using primary data (i.e., insurance claims databases, meta-analyses). (6) Single-dose studies assessing immediate infusion side effects. (7) Trials in which experimental medications were co-administered with TNF-I. (8) TNF-I withdrawal studies. (9) Studies incorporating a crossover component between a TNF-I and another experimental drug.
2.3. Data Extraction
Candidate studies were classified as interventional if prospectively assessing the effects of a TNF-I prescribed per experimental design, or observational if investigators played no role in dictating TNF-I administration. Studies were evaluated for TNF-I type, dosage and disease indication, study design, inclusion/exclusion criteria, sample size and duration of follow-up, patient demographics, incident malignancy cases, other adverse events, subject withdrawal rate, reported conflicts of interest, and funding sources. Two observers (C.D. plus R.G., N.P., D.I., E.L., or M.R.S.) independently extracted the data; differences were resolved by consensus.
2.4. Quality of Adverse Event and Risk of Bias Classification
We classified the adequacy of blinding as present if explicitly reported, “unknown” if not reported, or “not applicable” for single-arm studies. We scored drug safety reporting as “adequate”, “partially adequate”, or “inadequate” as described by Ioannidis and Lau [40]. Reports explicitly noting no adverse events were scored as “none”. Studies were classified as having “adequate” quality of adverse event reporting if they graded severity using a graduated toxicity scale and reported adverse event incidence in each study arm versus “partially adequate” if they failed to distinguish between moderate and severe toxicities or otherwise did not meet criteria for the “adequate” or “inadequate” categories. Studies were classified as “inadequate” if they did not detail the specific classes of adverse events, provided only generic statements, or omitted comment entirely. The quality of adverse event classifications for studies included in the meta-analyses are listed in Supplementary Table S1.
Risk of bias was assessed with the modified Cochrane analysis tool [41] for randomized studies and the ROBINS-I analysis tool for non-randomized studies [42]. Risk of bias assessments for included studies are detailed in Supplementary Table S2.
2.5. Statistical Analysis
For studies meeting criteria, we estimated malignancy rate ratios (MRRs) for the TNF-I-exposed vs. control groups with direct calculation. For studies evaluating multiple TNF-Is, each individual TNF-I-exposed group was analyzed separately against the control group. MRRs were estimated for overall (aggregate) malignancies excluding NMSC and for individual cancer subtypes [43]. In studies reporting no malignancies in either the TNF-I-exposed or control group, a continuity correction of 0.5 was applied to both groups. Studies reporting no malignancies in both groups were excluded from analysis. We used a random-effects meta-analysis model to account for potential heterogeneity between studies and to estimate pooled effects (95% confidence intervals) for rate ratios. The overall effect estimates are presented as a weighted mean of the study-specific estimates [44]. p values < 0.05 were considered statistically significant throughout the study and determined in a two-sided manner. Some studies involved multiple drugs and utilized shared unexposed controls, and there can be overlap between the contributed patient-years across multiple drug arms, from which dependencies can arise. In the cross-drug meta-analysis of the observational studies, we took such dependencies into account and used the rma.mv function in the metaphor package in R to model the non-independence structure induced by overlapping unexposed controls in the same study [45].
Forest plots were created using a standard rate scale to assess for publication bias. Studies with no incident malignancies other than NMSC were excluded from these plots. Study heterogeneity was evaluated using Cochran’s Q statistic and the statistic. was taken to represent moderate heterogeneity and to represent high heterogeneity.
Publication bias within studies was assessed with a funnel plot using a random-effects model. Rank correlation tests were used to assess for funnel plot asymmetry for the observational and interventional studies of each TNF-I and for observational and interventional studies aggregating all TNF-Is. Statistical analyses were carried out using R 4.0.2 (R Foundation, Vienna, Austria) and the metafor package [46].
3. Results
3.1. Search Results
We identified 16,150 candidate publications, yielding 55 unique studies for quantitative analysis (Figure 1). In total, 45/55 (82%) of the identified studies were interventional [47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91], and 10/55 (18%) were observational [25,92,93,94,95,96,97,98,99,100]. The PRISMA 2020 flowchart is included as Figure 1.
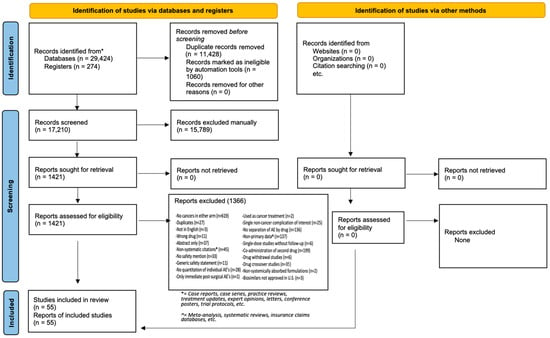
Figure 1.
PRISMA flow diagram (2020).
3.2. Interventional Study Results
The 45 interventional studies incorporated into the meta-analysis contributed a total of 22,652 patients with a median exposure of 41 weeks (IQR of 24–60 weeks) (Table 1). In total, seventeen of these studies reported on ADA (one study contained two separate randomized trials in the manuscript) [61], twelve on INX, four on ETN, six on CTZ, and seven on GLM. The median number of subjects exposed to a TNF-I was 360 (IQR of 216–634 patients). The median length of follow-up was 41 weeks (IQR of 24–64 weeks). These studies contributed a total of 146 malignancies over 15,120 patient-years of exposure to TNF-I: thirteen lymphomas, twelve breast cancers, twelve lung cancers, nine melanomas, eight colorectal cancers, five pancreatic cancers, four head and neck cancers, four ovarian cancers, three gastric cancers, three cervical cancers, two brain cancers, two renal cell carcinomas, two prostate cancers, two unspecified adenocarcinomas, one cholangiocarcinoma, one leukemia, one gastrointestinal carcinoid tumor, one bladder cancer, one testicular cancer, one endometrial cancer, and fifty-nine unspecified cancers (Supplementary Table S1). In total, 62 NMSCs were also recorded but not used in the meta-analysis.

Table 1.
Interventional and observational study characteristics of patients exposed to TNF-I.
There were 29 malignancies recorded over 4695 patient-years of placebo and/or non-TNF-I drug exposure: four breast cancers, three lymphomas, three prostate cancers, two cervical cancers, two lung cancers, one colorectal cancer, one esophageal cancer, one thyroid cancer, and twelve unspecified cancers (Supplementary Table S1). Nine NMSC were also recorded but not used in the meta-analysis.
The malignancy rate ratio for any malignancy was MRR 1.04 (95% CI 0.71–1.51) (Figure 2). For individual drugs, malignancy rate ratios were as follows: ADA (MRR 1.19, 95% CI 0.44–1.03), INX (MRR 1.35, 95% CI 0.67–2.72), ETN (MRR 0.80, 95% CI 0.22–2.88), CTZ (MRR 1.60, 95% CI 0.72–3.57), and GLM (MRR 1.49, 95% CI 0.59–3.77) (Figure 3A–E). Funnel plots did not demonstrate statistically significant asymmetry for overall TNF-I exposure or for any individual TNF-I exposure (Supplementary Figure S1).
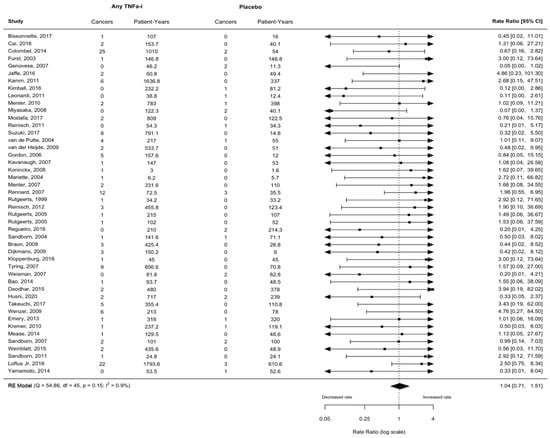
Figure 2.
Malignancy rate ratio in patients exposed to any TNF-I excluding NMSC in interventional studies [47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91].
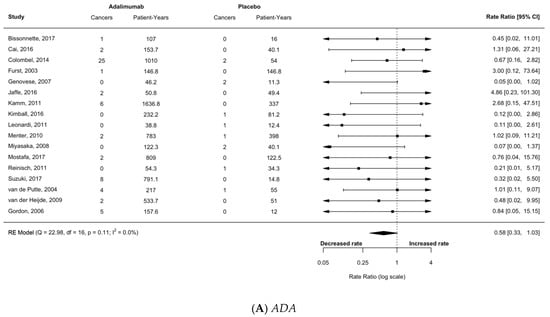
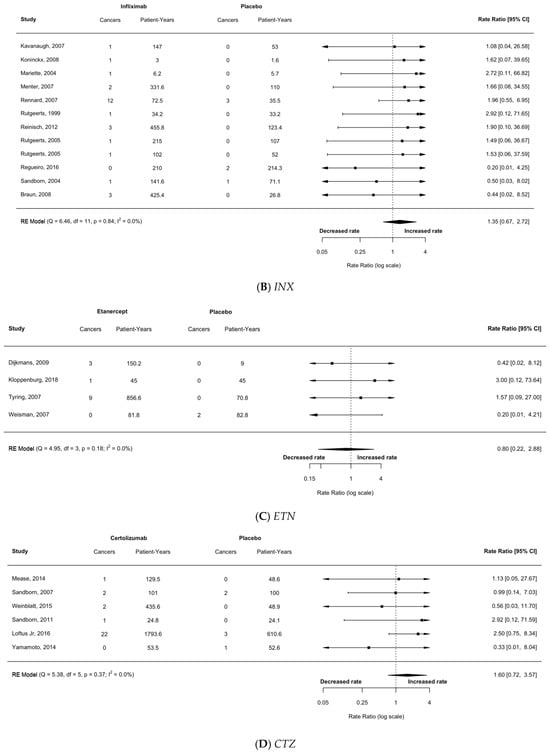
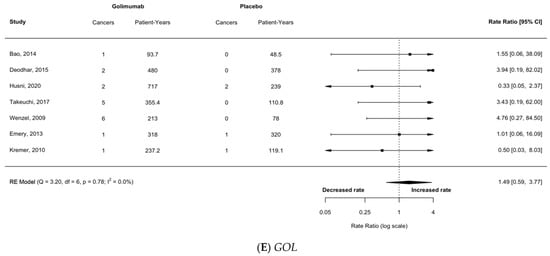
Figure 3.
Calculated malignancy rate ratio in patients exposed to any TNF-alpha inhibitor (TNF-I) using cancers excluding non-melanoma skin cancer (NMSC) in 45 interventional studies for (A) adalimumab (ADA); (B) infliximab (INX); (C) etanercept (ETN); (D) certolizumab (CTZ); (E) golimumab (GOL) [47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91].
In the interventional studies, only 9/45 (20%) had adequate quality of adverse event reporting according to the Ioannidis and Lau criteria, and 44/45 (98%) had either industry or unknown funding sources (Table 2). In total, 38/45 (84%) of the interventional studies had a low risk of bias due to high-quality randomization per the Cochrane criteria (Supplementary Table S2).
Table 2.
Quality of adverse event reporting (Ioannidis and Lau criteria) [33]: Interventional studies and observational studies.
3.3. Observational Study Results
The ten observational studies meeting the criteria for the meta-analysis contributed 34,866 patients with a median of 83 weeks of exposure (IQR 52–171 weeks) (Table 1). Five reported on ADA, five on INX, and five on ETN, with four of those studies reporting on more than one TNF-I. For these studies, the median number of patients exposed to a TNF-I was 1606 patients (IQR 433–3057 patients). The median length of follow-up was 82 weeks (IQR 54–171 weeks). There were 108 malignancies in 28,796 patient-years of TNF-I exposure: thirty-seven lymphomas, ten lung cancers, three head and neck cancers, three prostate cancers, two breast cancers, one esophageal cancer, one brain cancer, one colorectal cancer, one kidney cancer, and forty-nine unspecified cancers (Supplementary Table S1). There were also five NMSCs identified in the exposed subjects not included in analysis. There were 57 malignancies in 26,154 patient-years of placebo and/or non-TNF-I drug exposure: thirty-two lymphomas, five prostate cancers, two lung cancers, and eighteen unspecified cancers (Supplementary Table S1). One NMSC was also identified in these subjects and not included.
The malignancy rate ratio for any malignancy was MRR 1.42 (95% CI 0.72–2.79) (Figure 4). For individual drugs, the rate ratios were as follows: ADA (MRR 1.19, 95% CI 0.44–3.22), INX (MRR 1.69, 95% CI 0.83–3.44), and ETN (MRR 1.85, 95% CI 0.50–6.89) (Figure 5A–C). There were no observational studies of certolizumab or golimumab meeting the inclusion criteria. Funnel plots did not demonstrate statistically significant asymmetry for overall TNF-I exposure or for any individual TNF-I exposure (Supplementary Figure S2).
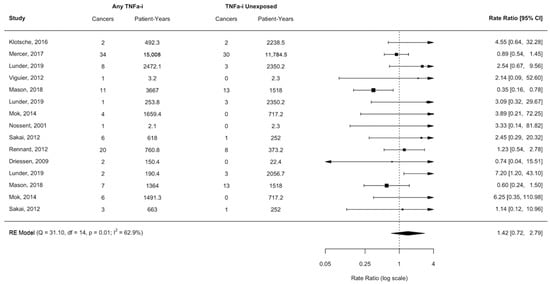
Figure 4.
Malignancy rate ratio in patients exposed to any TNF-I excluding NMSC in observational studies [25,92,93,94,95,96,97,98,99,100].
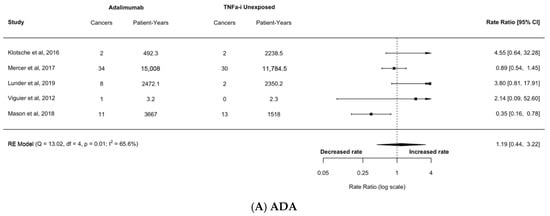
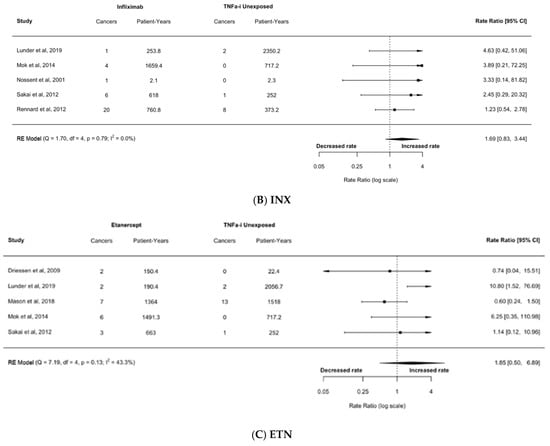
Figure 5.
Calculated malignancy rate ratio in patients exposed to any TNF-alpha inhibitor (TNF-I) using cancers excluding non-melanoma skin cancer (NMSC) in 10 observational studies for (A) adalimumab (ADA); (B) infliximab (INX); (C) etanercept (ETN) [25,92,93,94,95,96,97,98,99,100].
In the observational studies, 0/10 (0%) had adequate quality of adverse event reporting according to the Ioannidis and Lau criteria, and 8/10 (80%) had either industry or unknown funding sources (Table 2). In total, 2/10 (20%) of the observational studies were unlikely to have bias due to confounding, 10/10 (100%) were unlikely to have bias due to participant selection, 6/10 (60%) were unlikely to have bias due to the classification of interventions or deviation from intended interventions per the ROBINS-I criteria (Supplementary Table S2).
4. Discussion
We conducted a systematic review and meta-analyses of interventional and observational studies to evaluate the relationship between TNF-I exposure and the development of malignancies. This meta-analysis of 45 interventional studies did not demonstrate a statistically significant difference in cancer incidence for patients on a TNF-I (RR 1.04, 95% CI 0.71–1.51) (Figure 2). This meta-analysis of 10 observational studies also did not show a statistically increased risk of cancers in patients taking TNF-I (RR 1.42, 95% CI 0.72–2.79) (Figure 4) but did suggest a trend toward significance with both longer exposure to TNF-I and longer follow-up. This meta-analyses did not find differences in risk for patients taking specific TNF-I (Figure 3 and Figure 5), which is likely due to limited power when dividing the cohort up by individual drug exposure. Given its contemporary nature and scale, we believe the results presented here represent the broadest effort to date to define this relationship.
The most important finding of this study, however, is that the vast majority of the trials used to approve TNF-I indications, and the vast majority of long-term post-marketing studies, are inadequate in their quality of adverse event follow-up and have a significant risk for conflicts of interest and bias in reporting, with only 9 out of 55 studies (16.4%) demonstrating adequate adverse event reporting according to the Ioannidis and Lau criteria, only 3 out of 55 studies (5.5%) demonstrating clear non-industry funding, and only 40/55 (72.7%) demonstrating a low risk of bias per the Cochrane (interventional studies) and ROBINS-I (observational) criteria. Our meta-analysis is the first to report on these quality metrics for TNF-I studies and use the most stringent criteria for study inclusion. Many of the foundational efficacy randomized control trials were excluded due to the co-administration of drugs such as methotrexate or a trial design containing a drug crossover component. Another strength of our study is using patient-level data to collate and analyze individual and overall malignancy data.
The results of our meta-analyses are consistent with the antecedent literature and the findings of several prior meta-analyses, which did not demonstrate an effect of TNF-I use on the development of malignancies other than NMSC [15,17,30,31,32,33,34]. Several factors complicate the interpretation of these results. Most interventional studies of TNF-I were designed and powered to determine drug efficacy and rarely have follow-up greater than one year—as evidenced by the median length of follow-up of 41 weeks (IQR of 24–64 weeks) in our meta-analysis of the interventional studies. This may be an insufficient length of observation to define a difference in long-term cancer rates. The meta-analysis of observational studies incorporated datasets with a longer median follow-up of 82 weeks (IQR of 54–171 weeks) and indicated an increased risk of malignancies with TNF-I exposure, although not a statistically significant one. The meta-analyses of observational studies are challenging due to issues of publication bias and study and patient-level heterogeneity [27]. This was reflected in our quality of adverse events and risk of bias assessments (Table 2 and Supplementary Table S2) and could have potentially influenced our results despite attempts to restrict heterogeneity. Furthermore, few observational studies included in the meta-analysis directly compared a TNF-I to a placebo, with the comparator group usually being an anti-rheumatic medication other than a TNF-I (Table 1). Furthermore, there is no consensus in the literature as to what would be a biologically plausible timeframe post-drug exposure for malignancy development, which led to our decision to use 6 months post-exposure as a cutoff for biologic plausibility.
Our meta-analysis is also the first to our knowledge to employ this time-dependent follow-up analysis for drug exposure, which allowed us to meaningfully stratify patient cohorts into a model with significantly higher statistical power.
5. Conclusions
Our systematic review and meta-analyses of interventional and observational studies showed evidence of a relationship between TNF-I use and reported malignancies without reaching conventional thresholds for statistical significance. There were only a small number of high-quality studies with adequate adverse event reporting and an even smaller subset of those designed to investigate malignancy risk. These findings warrant further investigations over longer timeframes and the continued examination of the relationship between chronic inflammation, TNF-α signaling, and tumorigenesis.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers17030390/s1, Methods S1: PubMed MEDLINE Search Strategy; Figure S1: Random-effect funnel plots of interventional studies for (A) all TNF-I; (B) adalimumab (ADA); (C) infliximab (INX); (D) etanercept (ETN); (E) certolizumab (CTZ); (F) golimumab (GOL); Figure S2: Random-effect funnel plots of observational studies for (A) all TNF-I; (B) adalimumab (ADA); (C) infliximab (INX); (D) etanercept (ETN). Table S1: Malignancy Incidence of Interventional and Observational Studies of Patients Exposed to TNF-I; Table S2: Risk of bias assessments: (A) Cochrane (randomized) and (B) ROBINS-I (non-randomized).
Author Contributions
(CRediT author statement): C.B.D.: Conceptualization, Methodology, Validation, Formal Analysis, Investigation, Data Curation, Writing—Original Draft, Writing—Review and Editing; J.M.R.: Investigation, Data Curation, Writing—Review and Editing; D.I.: Validation, Investigation, Data Curation, Writing—Review and Editing; J.N.: Investigation, Data Curation; Y.J.: Methodology, Validation, Formal Analysis; X.M.: Methodology, Validation, Formal Analysis; C.Y.: Investigation, Data Curation; V.K.: Investigation, Data Curation; R.G.: Investigation, Data Curation; N.P.: Investigation, Data Curation, Writing—Review and Editing; E.L.: Investigation, Data Curation; M.R.S.: Investigation, Data Curation; T.M.: Methodology, Validation, Formal Analysis; J.S.W.: Methodology, Validation, Formal Analysis, Writing—Review and Editing; L.K.: Methodology, Validation, Formal Analysis, Writing—Review and Editing; H.Z.: Methodology, Validation, Formal Analysis, Writing—Review and Editing; M.B.: Methodology, Investigation; P.S.: Methodology, Investigation; E.M.S.: Conceptualization, Supervision, Project Administration, Funding Acquisition; S.D.K.: Conceptualization, Methodology, Validation, Resources, Supervision, Project Administration, Funding Acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Polsky Urologic Cancer Institute and the Department of Urology at Northwestern University Feinberg School of Medicine. The funder did not play a role in the design of this study; the collection, analysis, and interpretation of the data; the writing of the manuscript; and the decision to submit the manuscript for publication.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The dataset supporting the conclusions of this article is available in the GitHub repository, https://github.com/conordriscoll/TNF-Alpha-Meta-Analysis.git (accessed on 15 July 2020).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ADA | Adalimumab |
| AS | Ankylosing spondylitis |
| CD | Crohn’s disease |
| COPD | Chronic obstructive pulmonary disease |
| CTZ | Certolizumab |
| DMARD | Disease-modifying anti-rheumatic drug(s) |
| ETN | Etanercept |
| FAERS | [United States] Food and Drug Administration Adverse Events Reporting System |
| FDA | [United States] Food and Drug Administration |
| GBM | Glioblastoma multiforme |
| GLM | Golimumab |
| HL | Hodgkin’s Lymphoma(s) |
| HR | Hazard ratio(s) |
| HS | Hidradenitis suppurativa |
| INX | Infliximab |
| IQR | Interquartile range |
| IRB | Institutional Review Board |
| JIA | Juvenile idiopathic arthritis |
| MeSH | [National Library of Medicine] Medical subject heading(s) |
| MTX | Methotrexate |
| NHL | Non-Hodgkin’s Lymphoma(s) |
| NMSC | Non-melanoma skin cancer(s) |
| OA | Osteoarthritis |
| PS | Psoriasis |
| PSA | Psoriatic arthritis |
| RA | Rheumatoid arthritis |
| RR | Rate ratio(s) |
| SCC | Squamous cell carcinoma |
| SD | Standard deviation(s) |
| SPA | Spondyloarthropathy/spondyloarthropathies |
| SS | Sjogren’s syndrome |
| TNF-α | Tumor necrosis factor-alpha |
| TNF-i | Tumor necrosis factor-alpha inhibitor(s) |
| TNF-R | Tumor necrosis factor receptor |
| UC | Ulcerative colitis |
| 95% CI | 95% confidence interval |
References
- Gerriets, V.; Goyal, A.; Khaddour, K.; Tumor Necrosis Factor Inhibitors. Stat Pearls. Available online: https://www.ncbi.nlm.nih.gov/books/NBK482425/ (accessed on 9 May 2022).
- Mitoma, H.; Horiuchi, T.; Tsukamoto, H.; Ueda, N. Molecular Mechanisms of Action of Anti-TNF-α Agents—Comparison Among Therapeutic TNF-α Antagonists. Cytokine 2018, 101, 56–63. [Google Scholar] [CrossRef]
- Urquhart, L. Top Companies and Drugs by Sales in 2021. Nature Reviews Drug Discovery. Available online: https://www.nature.com/articles/d41573-022-00047-9 (accessed on 10 May 2022).
- Urquhart, L. Top Companies and Drugs by Sales in 2017. Nature Reviews Drug Discovery. Available online: https://www.nature.com/articles/d41573-022-00047-9 (accessed on 10 May 2022).
- Urquhart, L. Top Companies and Drugs by Sales in 2020. Nature Reviews Drug Discovery. Available online: https://www.nature.com/articles/d41573-022-00047-9 (accessed on 10 May 2022).
- Goel, N.; Stephens, S. Certolizumab pegol. MAbs 2010, 2, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.A.; Weiner, A.B.; Catalona, W.J.; Li, E.V.; Schaeffer, E.M.; Hanauer, S.B.; Strong, S.; Burns, J.; Hussain, M.H.A.; Kundu, S.D. Inflammatory Bowel Disease and the Risk of Prostate Cancer. Eur. Urol. 2019, 75, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F. Tumour necrosis factor and cancer. Nat. Rev. Cancer 2009, 9, 361–371. [Google Scholar] [CrossRef]
- Montfort, A.; Colacios, C.; Levade, T.; Andrieu-Abadie, N.; Meyer, N.; Ségui, B. The TNF Paradox in Cancer Progression and Immunotherapy. Front. Immunol. 2019, 10, 1818. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.Y.; Wolchok, J.D.; Bass, A.R. TNF in the era of immune checkpoint inhibitors: Friend or foe? Nat. Rev. Rheumatol. 2021, 17, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Scott, F.I.; Mamtani, R.; Brensinger, C.M.; Haynes, K.; Chiesa-Fuxench, Z.C.; Zhang, J.; Chen, L.; Xie, F.; Yun, H.; Osterman, M.T.; et al. Risk of Nonmelanoma Skin Cancer Associated with the Use of Immunosuppressant and Biologic Agents in Patients with a History of Autoimmune Disease and Nonmelanoma Skin Cancer. JAMA Dermatol. 2016, 152, 164–172. [Google Scholar] [CrossRef]
- D’Arcy, M.E.; Beachler, D.C.; Pfeiffer, R.M.; Curtis, J.R.; Mariette, X.; Seror, R.; Mahale, P.; Rivera, D.R.; Yanik, E.L.; Engels, E.A. Tumor Necrosis Factor Inhibitors and the Risk of Cancer among Older Americans with Rheumatoid Arthritis. Cancer Epidemiol. Biomark. Prev. 2021, 30, 2059–2067. [Google Scholar] [CrossRef]
- Wolfe, F.; Michaud, K. Biologic treatment of rheumatoid arthritis and the risk of malignancy: Analyses from a large US observational study. Arthritis Rheum. 2007, 56, 2886–2895. [Google Scholar] [CrossRef]
- Amari, W.; Zeringue, A.L.; McDonald, J.R.; Caplan, L.; Eisen, S.A.; Ranganathan, P. Risk of non-melanoma skin cancer in a national cohort of veterans with rheumatoid arthritis. Rheumatology 2011, 50, 1431–1439. [Google Scholar] [CrossRef] [PubMed]
- Peleva, E.; Exton, L.S.; Kelley, K.; Kleyn, C.E.; Mason, K.J.; Smith, C.H. Risk of cancer in patients with psoriasis on biological therapies: A systematic review. Br. J. Dermatol. 2018, 178, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.L.; Yin, W.J.; Zhou, L.Y.; Zhou, G.; Liu, K.; Hu, C.; Zuo, X.C.; Wang, Y.F. Risk of non-melanoma skin cancer for rheumatoid arthritis patients receiving TNF antagonist: A systematic review and meta-analysis. Clin. Rheumatol. 2020, 39, 769–778. [Google Scholar] [CrossRef]
- Askling, J.; Fahrbach, K.; Nordstrom, B.; Ross, S.; Schmid, C.H.; Symmons, D. Cancer risk with tumor necrosis factor alpha (TNF) inhibitors: Meta-analysis of randomized controlled trials of adalimumab, etanercept, and infliximab using patient level data. Pharmacoepidemiol. Drug Saf. 2011, 20, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Diak, P.; Siegel, J.; La Grenade, L.; Choi, L.; Lemery, S.; McMahon, A. Tumor necrosis factor alpha blockers and malignancy in children: Forty-eight cases reported to the Food and Drug Administration. Arthritis Rheum. 2010, 62, 2517–2524. [Google Scholar] [CrossRef] [PubMed]
- Lemaitre, M.; Kirchgesner, J.; Rudnichi, A.; Carrat, F.; Zureik, M.; Carbonnel, F.; Dray-Spira, R. Association Between Use of Thiopurines or Tumor Necrosis Factor Antagonists Alone or in Combination and Risk of Lymphoma in Patients With Inflammatory Bowel Disease. JAMA 2017, 318, 1679–1686. [Google Scholar] [CrossRef] [PubMed]
- Deepak, P.; Sifuentes, H.; Sherid, M.; Stobaugh, D.; Sadozai, Y.; Ehrenpreis, E.D. T-cell non-Hodgkin’s lymphomas reported to the FDA AERS with tumor necrosis factor-alpha (TNF-α) inhibitors: Results of the REFURBISH study. Am. J. Gastroenterol. 2013, 108, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Calip, G.S.; Patel, P.R.; Adimadhyam, S.; Xing, S.; Wu, Z.; Sweiss, K.; Schumock, G.T.; Lee, T.A.; Chiu, B.C. Tumor necrosis factor-alpha inhibitors and risk of non-Hodgkin lymphoma in a cohort of adults with rheumatologic conditions. Int. J. Cancer 2018, 143, 1062–1071. [Google Scholar] [CrossRef]
- Baecklund, E.; Iliadou, A.; Askling, J.; Ekbom, A.; Backlin, C.; Granath, F.; Catrina, A.I.; Rosenquist, R.; Feltelius, N.; Sundström, C.; et al. Association of chronic inflammation, not its treatment, with increased lymphoma risk in rheumatoid arthritis. Arthritis Rheum. 2006, 54, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Hellgren, K.; Dreyer, L.; Arkema, E.V.; Glintborg, B.; Jacobsson, L.T.; Kristensen, L.E.; Feltelius, N.; Hetland, M.L.; Askling, J.; ARTIS Study Group, For the DANBIO Study Group. Cancer risk in patients with spondyloarthritis treated with TNF inhibitors: A collaborative study from the ARTIS and DANBIO registers. Ann. Rheum. Dis. 2017, 76, 105–111. [Google Scholar] [CrossRef]
- Mariette, X.; Tubach, F.; Bagheri, H.; Bardet, M.; Berthelot, J.M.; Gaudin, P.; Heresbach, D.; Martin, A.; Schaeverbeke, T.; Salmon, D.; et al. Lymphoma in patients treated with anti-TNF: Results of the 3-year prospective French RATIO registry. Ann. Rheum. Dis. 2010, 69, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Mercer, L.K.; Galloway, J.B.; Lunt, M.; Davies, R.; Low, A.L.; Dixon, W.G.; Watson, K.D.; BSRBR Control Centre Consortium; Symmons, D.P.; Hyrich, K.L. Risk of lymphoma in patients exposed to antitumour necrosis factor therapy: Results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis. Ann. Rheum. Dis. 2017, 76, 497–503. [Google Scholar] [CrossRef]
- Dreyer, L.; Mellemkjær, L.; Andersen, A.R.; Bennett, P.; Poulsen, U.E.; Juulsgaard Ellingsen, T.; Hansen, T.H.; Jensen, D.V.; Linde, L.; Lindegaard, H.M.; et al. Incidences of overall and site specific cancers in TNFα inhibitor treated patients with rheumatoid arthritis and other arthritides—a follow-up study from the DANBIO Registry. Ann. Rheum. Dis. 2013, 72, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Mariette, X.; Matucci-Cerinic, M.; Pavelka, K.; Taylor, P.; van Vollenhoven, R.; Heatley, R.; Walsh, C.; Lawson, R.; Reynolds, A.; Emery, P. Malignancies associated with tumour necrosis factor inhibitors in registries and prospective observational studies: A systematic review and meta-analysis. Ann. Rheum. Dis. 2011, 70, 1895–1904. [Google Scholar] [CrossRef] [PubMed]
- Nyboe Andersen, N.; Pasternak, B.; Basit, S.; Andersson, M.; Svanström, H.; Caspersen, S.; Munkholm, P.; Hviid, A.; Jess, T. Association between tumor necrosis factor-α antagonists and risk of cancer in patients with inflammatory bowel disease. JAMA 2014, 311, 2406–2413. [Google Scholar] [CrossRef]
- Askling, J.; Baecklund, E.; Granath, F.; Geborek, P.; Fored, M.; Backlin, C.; Bertilsson, L.; Cöster, L.; Jacobsson, L.T.; Lindblad, S.; et al. Anti-tumour necrosis factor therapy in rheumatoid arthritis and risk of malignant lymphomas: Relative risks and time trends in the Swedish Biologics Register. Ann. Rheum. Dis. 2009, 68, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Denaro, N.; Nazzaro, G.; Murgia, G.; Scarfì, F.; Cauchi, C.; Carrera, C.G.; Cattaneo, A.; Solinas, C.; Scartozzi, M.; Marzano, A.V.; et al. A Multidisciplinary Approach to Patients with Psoriasis and a History of Malignancies or On-Treatment for Solid Tumors: A Narrative Literature Review. Int. J. Mol. Sci. 2023, 24, 17540. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hou, L.Q.; Jiang, G.X.; Chen, Y.F.; Yang, X.M.; Meng, L.; Xue, M.; Liu, X.G.; Chen, X.C.; Li, X. The Comparative Safety of TNF Inhibitors in Ankylosing Spondylitis-a Meta-Analysis Update of 14 Randomized Controlled Trials. Clin. Rev. Allergy Immunol. 2018, 54, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Moulis, G.; Sommet, A.; Béné, J.; Montastruc, F.; Sailler, L.; Montastruc, J.L.; Lapeyre-Mestre, M. Cancer risk of anti-TNF-α at recommended doses in adult rheumatoid arthritis: A meta-analysis with intention to treat and per protocol analyses. PLoS ONE 2012, 7, e48991. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.J.; Peyrin-Biroulet, L.; Ford, A.C. Systematic review with meta-analysis: Malignancies with anti-tumour necrosis factor-α therapy in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2014, 39, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Dommasch, E.D.; Abuabara, K.; Shin, D.B.; Nguyen, J.; Troxel, A.B.; Gelfand, J.M. The risk of infection and malignancy with tumor necrosis factor antagonists in adults with psoriatic disease: A systematic review and meta-analysis of randomized controlled trials. J. Am. Acad. Dermatol. 2011, 64, 1035–1050. [Google Scholar] [CrossRef]
- Wetzman, A.; Lukas, C.; Gaujoux-Viala, C.; Mamtani, R.; Barnetche, T.; Combe, B.; Morel, J.; Szafors, P. Risk of Cancer After Initiation of Targeted Therapies in Patients With Rheumatoid Arthritis and a Prior Cancer: Systematic Review With Meta-Analysis. Arthritis Care Res. 2023, 75, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, G.R.; Rutgeerts, P.; Sandborn, W.J.; Sands, B.E.; Diamond, R.H.; Blank, M.; Montello, J.; Tang, L.; Cornillie, F.; Colombel, J.F. A pooled analysis of infections, malignancy, and mortality in infliximab- and immunomodulator-treated adult patients with inflammatory bowel disease. Am. J. Gastroenterol. 2012, 107, 1051–1063. [Google Scholar] [CrossRef] [PubMed]
- Haynes, K.; Beukelman, T.; Curtis, J.R.; Newcomb, C.; Herrinton, L.J.; Graham, D.J.; Solomon, D.H.; Griffin, M.R.; Chen, L.; Liu, L.; et al. Tumor necrosis factor α inhibitor therapy and cancer risk in chronic immune-mediated diseases. Arthritis Rheum. 2013, 65, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Bongartz, T.; Sutton, A.J.; Sweeting, M.J.; Buchan, I.; Matteson, E.L.; Montori, V. Anti-TNF antibody therapy in rheumatoid arthritis and the risk of serious infections and malignancies: Systematic review and meta-analysis of rare harmful effects in randomized controlled trials. JAMA 2006, 295, 2275–2285. [Google Scholar] [CrossRef] [PubMed]
- FDA Adverse Event Reporting System (FAERS) Public Dashboard. 2021. Available online: https://www.fda.gov/drugs/questions-and-answers-fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-public-dashboard (accessed on 3 May 2022).
- Ioannidis, J.P.; Lau, J. Completeness of safety reporting in randomized trials: An evaluation of 7 medical areas. JAMA 2001, 285, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, 14898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials. 2015, 45, 139–145. [Google Scholar] [CrossRef]
- Normand, S.L. Meta-analysis: Formulating, evaluating, combining, and reporting. Stat. Med. 1999, 18, 321–359. [Google Scholar] [CrossRef]
- Schober, P.; Vetter, T.R. Repeated Measures Designs and Analysis of Longitudinal Data: If at First You Do Not Succeed-Try, Try Again. Anesth. Analg. 2018, 127, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W. Conducting Meta-Analyses in R. with the metafor Package. J. Stat. Soft. 2010, 36, 3. [Google Scholar] [CrossRef]
- Bissonnette, R.; Harel, F.; Krueger, J.G.; Guertin, M.C.; Chabot-Blanchet, M.; Gonzalez, J.; Maari, C.; Delorme, I.; Lynde, C.W.; Tardif, J.C. TNF-α Antagonist and Vascular Inflammation in Patients with Psoriasis Vulgaris: A Randomized Placebo-Controlled Study. J. Investig. Dermatol. 2017, 137, 1638–1645. [Google Scholar] [CrossRef]
- Cai, L.; Gu, J.; Zheng, J.; Zheng, M.; Wang, G.; Xi, L.Y.; Hao, F.; Liu, X.M.; Sun, Q.N.; Wang, Y.; et al. Efficacy and safety of adalimumab in Chinese patients with moderate-to-severe plaque psoriasis: Results from a phase 3, randomized, placebo-controlled, double-blind study. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Colombel, J.F.; Sandborn, W.J.; Ghosh, S.; Wolf, D.C.; Panaccione, R.; Feagan, B.; Reinisch, W.; Robinson, A.M.; Lazar, A.; Kron, M.; et al. Four-year maintenance treatment with adalimumab in patients with moderately to severely active ulcerative colitis: Data from ULTRA 1, 2, and 3. Am. J. Gastroenterol. 2014, 109, 1771–1780. [Google Scholar] [CrossRef] [PubMed]
- Furst, D.E.; Schiff, M.H.; Fleischmann, R.M.; Strand, V.; Birbara, C.A.; Compagnone, D.; Fischkoff, S.A.; Chartash, E.K. Adalimumab, a fully human anti tumor necrosis factor-alpha monoclonal antibody, and concomitant standard antirheumatic therapy for the treatment of rheumatoid arthritis: Results of STAR (Safety Trial of Adalimumab in Rheumatoid Arthritis). J. Rheumatol. 2003, 30, 2563–2567. [Google Scholar] [PubMed]
- Genovese, M.C.; Mease, P.J.; Thomson, G.T.; Kivitz, A.J.; Perdok, R.J.; Weinberg, M.A.; Medich, J.; Sasso, E.H.; M02-570 Study Group. Safety and efficacy of adalimumab in treatment of patients with psoriatic arthritis who had failed disease modifying antirheumatic drug therapy. J. Rheumatol. 2007, 34, 1040–1050. [Google Scholar] [PubMed]
- Jaffe, G.J.; Dick, A.D.; Brézin, A.P.; Nguyen, Q.D.; Thorne, J.E.; Kestelyn, P.; Barisani-Asenbauer, T.; Franco, P.; Heiligenhaus, A.; Scales, D.; et al. Adalimumab in Patients with Active Noninfectious Uveitis. N. Engl. J. Med. 2016, 375, 932–943. [Google Scholar] [CrossRef]
- Kamm, M.A.; Hanauer, S.B.; Panaccione, R.; Colombel, J.F.; Sandborn, W.J.; Pollack, P.F.; Zhou, Q.; Robinson, A.M. Adalimumab sustains steroid-free remission after 3 years of therapy for Crohn’s disease. Aliment. Pharmacol. Ther. 2011, 34, 306–317. [Google Scholar] [CrossRef] [PubMed]
- Kimball, A.B.; Okun, M.M.; Williams, D.A.; Gottlieb, A.B.; Papp, K.A.; Zouboulis, C.C.; Armstrong, A.W.; Kerdel, F.; Gold, M.H.; Forman, S.B.; et al. Two Phase 3 Trials of Adalimumab for Hidradenitis Suppurativa. N. Engl. J. Med. 2016, 375, 422–434. [Google Scholar] [CrossRef]
- Leonardi, C.; Langley, R.G.; Papp, K.; Tyring, S.K.; Wasel, N.; Vender, R.; Unnebrink, K.; Gupta, S.R.; Valdecantos, W.C.; Bagel, J. Adalimumab for treatment of moderate to severe chronic plaque psoriasis of the hands and feet: Efficacy and safety results from REACH, a randomized, placebo-controlled, double-blind trial. Arch. Dermatol. 2011, 147, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Menter, A.; Gordon, K.B.; Leonardi, C.L.; Gu, Y.; Goldblum, O.M. Efficacy and safety of adalimumab across subgroups of patients with moderate to severe psoriasis. J. Am. Acad. Dermatol. 2010, 63, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Miyasaka, N.; CHANGE Study Investigators. Clinical investigation in highly disease-affected rheumatoid arthritis patients in Japan with adalimumab applying standard and general evaluation: The CHANGE study. Mod. Rheumatol. 2008, 18, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, N.M.; Nader, A.M.; Noertersheuser, P.; Okun, M.; Awni, W.M. Impact of immunogenicity on pharmacokinetics, efficacy and safety of adalimumab in adult patients with moderate to severe chronic plaque psoriasis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Reinisch, W.; Sandborn, W.J.; Hommes, D.W.; D’Haens, G.; Hanauer, S.; Schreiber, S.; Panaccione, R.; Fedorak, R.N.; Tighe, M.B.; Huang, B.; et al. Adalimumab for induction of clinical remission in moderately to severely active ulcerative colitis: Results of a randomised controlled trial. Gut 2011, 60, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Motoya, S.; Hanai, H.; Hibi, T.; Nakamura, S.; Lazar, A.; Robinson, A.M.; Skup, M.; Mostafa, N.M.; Huang, B.; et al. Four-year maintenance treatment with adalimumab in Japanese patients with moderately to severely active ulcerative colitis. J. Gastroenterol. 2017, 52, 1031–1040. [Google Scholar] [CrossRef]
- van de Putte, L.B.; Atkins, C.; Malaise, M.; Sany, J.; Russell, A.S.; van Riel, P.L.; Settas, L.; Bijlsma, J.W.; Todesco, S.; Dougados, M.; et al. Efficacy and safety of adalimumab as monotherapy in patients with rheumatoid arthritis for whom previous disease modifying antirheumatic drug treatment has failed. Ann. Rheum. Dis. 2004, 63, 508–516. [Google Scholar] [CrossRef]
- van der Heijde, D.; Schiff, M.H.; Sieper, J.; Kivitz, A.J.; Wong, R.L.; Kupper, H.; Dijkmans, B.A.; Mease, P.J.; Davis, J.C., Jr.; ATLAS Study Group. Adalimumab effectiveness for the treatment of ankylosing spondylitis is maintained for up to 2 years: Long-term results from the ATLAS trial. Ann. Rheum. Dis. 2009, 68, 922–929. [Google Scholar] [CrossRef]
- Gordon, K.B.; Langley, R.G.; Leonardi, C.; Toth, D.; Menter, M.A.; Kang, S.; Heffernan, M.; Miller, B.; Hamlin, R.; Lim, L.; et al. Clinical response to adalimumab treatment in patients with moderate to severe psoriasis: Double-blind, randomized controlled trial and open-label extension study. J. Am. Acad. Dermatol. 2006, 55, 598–606. [Google Scholar] [CrossRef]
- Kavanaugh, A.; Krueger, G.G.; Beutler, A.; Guzzo, C.; Zhou, B.; Dooley, L.T.; Mease, P.J.; Gladman, D.D.; de Vlam, K.; Geusens, P.P.; et al. Infliximab maintains a high degree of clinical response in patients with active psoriatic arthritis through 1 year of treatment: Results from the IMPACT 2 trial. Ann. Rheum. Dis. 2007, 66, 498–505. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Koninckx, P.R.; Craessaerts, M.; Timmerman, D.; Cornillie, F.; Kennedy, S. Anti-TNF-alpha treatment for deep endometriosis-associated pain: A randomized placebo-controlled trial. Hum. Reprod. 2008, 23, 2017–2023. [Google Scholar] [CrossRef]
- Mariette, X.; Ravaud, P.; Steinfeld, S.; Baron, G.; Goetz, J.; Hachulla, E.; Combe, B.; Puéchal, X.; Pennec, Y.; Sauvezie, B.; et al. Inefficacy of infliximab in primary Sjögren’s syndrome: Results of the randomized, controlled Trial of Remicade in Primary Sjögren’s Syndrome (TRIPSS). Arthritis Rheum. 2004, 50, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Menter, A.; Feldman, S.R.; Weinstein, G.D.; Papp, K.; Evans, R.; Guzzo, C.; Li, S.; Dooley, L.T.; Arnold, C.; Gottlieb, A.B. A randomized comparison of continuous vs. intermittent infliximab maintenance regimens over 1 year in the treatment of moderate-to-severe plaque psoriasis. J. Am. Acad. Dermatol. 2007, 56, e1–e15. [Google Scholar] [CrossRef]
- Rennard, S.I.; Fogarty, C.; Kelsen, S.; Long, W.; Ramsdell, J.; Allison, J.; Mahler, D.; Saadeh, C.; Siler, T.; Snell, P.; et al. The safety and efficacy of infliximab in moderate to severe chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2007, 175, 926–934. [Google Scholar] [CrossRef]
- Rutgeerts, P.; D’Haens, G.; Targan, S.; Vasiliauskas, E.; Hanauer, S.B.; Present, D.H.; Mayer, L.; Van Hogezand, R.A.; Braakman, T.; DeWoody, K.L.; et al. Efficacy and safety of retreatment with anti-tumor necrosis factor antibody (infliximab) to maintain remission in Crohn’s disease. Gastroenterology 1999, 117, 761–769. [Google Scholar] [CrossRef]
- Reinisch, W.; Sandborn, W.J.; Rutgeerts, P.; Feagan, B.G.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; de Villiers, W.J.; Blank, M.; Lang, Y.; et al. Long-term infliximab maintenance therapy for ulcerative colitis: The ACT-1 and -2 extension studies. Inflamm. Bowel Dis. 2012, 18, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Rutgeerts, P.; Sandborn, W.J.; Feagan, B.G.; Reinisch, W.; Olson, A.; Johanns, J.; Travers, S.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N. Engl. J. Med. 2005, 353, 2462–2476. [Google Scholar] [CrossRef]
- Regueiro, M.; Feagan, B.G.; Zou, B.; Johanns, J.; Blank, M.A.; Chevrier, M.; Plevy, S.; Popp, J.; Cornillie, F.J.; Lukas, M.; et al. Infliximab Reduces Endoscopic, but Not Clinical, Recurrence of Crohn’s Disease After Ileocolonic Resection. Gastroenterology 2016, 150, 1568–1578. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; Feagan, B.G.; Radford-Smith, G.; Kovacs, A.; Enns, R.; Innes, A.; Patel, J. CDP571, a humanised monoclonal antibody to tumour necrosis factor alpha, for moderate to severe Crohn’s disease: A randomised, double blind, placebo controlled trial. Gut 2004, 53, 1485–1493. [Google Scholar] [CrossRef]
- Braun, J.; Deodhar, A.; Dijkmans, B.; Geusens, P.; Sieper, J.; Williamson, P.; Xu, W.; Visvanathan, S.; Baker, D.; Goldstein, N.; et al. Ankylosing Spondylitis Study for the Evaluation of Recombinant Infliximab Therapy Study Group. Efficacy and safety of infliximab in patients with ankylosing spondylitis over a two-year period. Arthritis Rheum. 2008, 59, 1270–1278. [Google Scholar] [CrossRef]
- Dijkmans, B.; Emery, P.; Hakala, M.; Leirisalo-Repo, M.; Mola, E.M.; Paolozzi, L.; Salvarani, C.; Sanmarti, R.; Sibilia, J.; Sieper, J.; et al. Etanercept in the longterm treatment of patients with ankylosing spondylitis. J. Rheumatol. 2009, 36, 1256–1264. [Google Scholar] [CrossRef]
- Kloppenburg, M.; Ramonda, R.; Bobacz, K.; Kwok, W.Y.; Elewaut, D.; Huizinga, T.W.J.; Kroon, F.P.B.; Punzi, L.; Smolen, J.S.; Vander Cruyssen, B.; et al. Etanercept in patients with inflammatory hand osteoarthritis (EHOA): A multicentre, randomised, double-blind, placebo-controlled trial. Ann. Rheum. Dis. 2018, 77, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- Tyring, S.; Gordon, K.B.; Poulin, Y.; Langley, R.G.; Gottlieb, A.B.; Dunn, M.; Jahreis, A. Long-term safety and efficacy of 50 mg of etanercept twice weekly in patients with psoriasis. Arch. Dermatol. 2007, 143, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Weisman, M.H.; Paulus, H.E.; Burch, F.X.; Kivitz, A.J.; Fierer, J.; Dunn, M.; Kerr, D.R.; Tsuji, W.; Baumgartner, S.W. A placebo-controlled, randomized, double-blinded study evaluating the safety of etanercept in patients with rheumatoid arthritis and concomitant comorbid diseases. Rheumatology 2007, 46, 1122–1125. [Google Scholar] [CrossRef] [PubMed]
- Bao, C.; Huang, F.; Khan, M.A.; Fei, K.; Wu, Z.; Han, C.; Hsia, E.C. Safety and efficacy of golimumab in Chinese patients with active ankylosing spondylitis: 1-year results of a multicentre, randomized, double-blind, placebo-controlled phase III trial. Rheumatology 2014, 53, 1654–1663. [Google Scholar] [CrossRef]
- Deodhar, A.; Braun, J.; Inman, R.D.; van der Heijde, D.; Zhou, Y.; Xu, S.; Han, C.; Hsu, B. Golimumab administered subcutaneously every 4 weeks in ankylosing spondylitis: 5-year results of the GO-RAISE study. Ann. Rheum. Dis. 2015, 74, 757–761. [Google Scholar] [CrossRef] [PubMed]
- Husni, M.E.; Kavanaugh, A.; Murphy, F.; Rekalov, D.; Harrison, D.D.; Kim, L.; Lo, K.H.; Leu, J.H.; Hsia, E.C. Efficacy and Safety of Intravenous Golimumab Through One Year in Patients With Active Psoriatic Arthritis. Arthritis Care Res. 2020, 72, 806–813. [Google Scholar] [CrossRef]
- Takeuchi, T.; Harigai, M.; Tanaka, Y.; Yamanaka, H.; Ishiguro, N.; Yamamoto, K.; Miyasaka, N.; Koike, T.; Ukyo, Y.; Ishii, Y.; et al. Clinical efficacy, radiographic, and safety results of golimumab monotherapy in Japanese patients with active rheumatoid arthritis despite prior therapy with disease-modifying antirheumatic drugs: Final results of the GO-MONO trial through week 120. Mod. Rheumatol. 2018, 28, 770–779. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, S.E.; Barnes, P.J.; Bleecker, E.R.; Bousquet, J.; Busse, W.; Dahlén, S.E.; Holgate, S.T.; Meyers, D.A.; Rabe, K.F.; Antczak, A.; et al. A randomized, double-blind, placebo-controlled study of tumor necrosis factor-alpha blockade in severe persistent asthma. Am. J. Respir. Crit. Care Med. 2009, 179, 549–558. [Google Scholar] [CrossRef]
- Emery, P.; Fleischmann, R.M.; Doyle, M.K.; Strusberg, I.; Durez, P.; Nash, P.; Amante, E.; Churchill, M.; Park, W.; Pons-Estel, B.; et al. Golimumab, a human anti–tumor necrosis factor monoclonal antibody, injected subcutaneously every 4 weeks in patients with active rheumatoid arthritis who had never taken methotrexate: 1-year and 2-year clinical, radiologic, and physical function findings of a phase III, multicenter, randomized, double-blind, placebo-controlled study. Arthritis Care Res. 2013, 65, 1732–1742. [Google Scholar] [CrossRef]
- Kremer, J.; Ritchlin, C.; Mendelsohn, A.; Baker, D.; Kim, L.; Xu, Z.; Han, J.; Taylor, P. Golimumab, a new human anti-tumor necrosis factor alpha antibody, administered intravenously in patients with active rheumatoid arthritis: Forty-eight-week efficacy and safety results of a phase III randomized, double-blind, placebo-controlled study. Arthritis Rheum. 2010, 62, 917–928. [Google Scholar] [CrossRef]
- Mease, P.J.; Fleischmann, R.; Deodhar, A.A.; Wollenhaupt, J.; Khraishi, M.; Kielar, D.; Woltering, F.; Stach, C.; Hoepken, B.; Arledge, T.; et al. Effect of certolizumab pegol on signs and symptoms in patients with psoriatic arthritis: 24-week results of a Phase 3 double-blind randomised placebo-controlled study (RAPID-PsA). Ann. Rheum. Dis. 2014, 73, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; Feagan, B.G.; Stoinov, S.; Honiball, P.J.; Rutgeerts, P.; Mason, D.; Bloomfield, R.; Schreiber, S.; PRECISE 1 Study Investigators. Certolizumab pegol for the treatment of Crohn’s disease. N. Engl. J. Med. 2007, 357, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Weinblatt, M.E.; Fleischmann, R.; van Vollenhoven, R.F.; Emery, P.; Huizinga, T.W.; Cutolo, M.; van der Heijde, D.; Duncan, B.; Davies, O.; Luijtens, K.; et al. Twenty-eight-week results from the REALISTIC phase IIIb randomized trial: Efficacy, safety and predictability of response to certolizumab pegol in a diverse rheumatoid arthritis population. Arthritis Res. Ther. 2015, 17, 325. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sandborn, W.J.; Schreiber, S.; Feagan, B.G.; Rutgeerts, P.; Younes, Z.H.; Bloomfield, R.; Coteur, G.; Guzman, J.P.; D’Haens, G.R. Certolizumab pegol for active Crohn’s disease: A placebo-controlled, randomized trial. Clin. Gastroenterol. Hepatol. 2011, 9, 670–678.e3. [Google Scholar] [CrossRef]
- Loftus, E.V., Jr.; Colombel, J.F.; Schreiber, S.; Randall, C.W.; Regueiro, M.; Ali, T.; Arendt, C.; Coarse, J.; Spearman, M.; Kosutic, G. Safety of Long-term Treatment With Certolizumab Pegol in Patients With Crohn’s Disease, Based on a Pooled Analysis of Data From Clinical Trials. Clin. Gastroenterol. Hepatol. 2016, 14, 1753–1762. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Takeuchi, T.; Yamanaka, H.; Ishiguro, N.; Tanaka, Y.; Eguchi, K.; Watanabe, A.; Origasa, H.; Iwai, K.; Sakamaki, Y.; et al. Efficacy and safety of certolizumab pegol without methotrexate co-administration in Japanese patients with active rheumatoid arthritis: The HIKARI randomized, placebo-controlled trial. Mod. Rheumatol. 2014, 24, 552–560. [Google Scholar] [CrossRef]
- Klotsche, J.; Niewerth, M.; Haas, J.P.; Huppertz, H.I.; Zink, A.; Horneff, G.; Minden, K. Long-term safety of etanercept and adalimumab compared to methotrexate in patients with juvenile idiopathic arthritis (JIA). Ann. Rheum. Dis. 2016, 75, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Lunder, T.; Zorko, M.S.; Kolar, N.K.; Suhodolcan, A.B.; Marovt, M.; Leskovec, N.K.; Marko, P.B. Drug survival of biological therapy is showing class effect: Updated results from Slovenian National Registry of psoriasis. Int. J. Dermatol. 2019, 58, 631–641. [Google Scholar] [CrossRef] [PubMed]
- Viguier, M.; Pagès, C.; Aubin, F.; Delaporte, E.; Descamps, V.; Lok, C.; Beylot-Barry, M.; Séneschal, J.; Dubertret, L.; Morand, J.J.; et al. Efficacy and safety of biologics in erythrodermic psoriasis: A multicentre, retrospective study. Br. J. Dermatol. 2012, 167, 417–423. [Google Scholar] [CrossRef]
- Mason, K.J.; Barker, J.N.W.N.; Smith, C.H.; Hampton, P.J.; Lunt, M.; McElhone, K.; Warren, R.B.; Yiu, Z.Z.N.; Griffiths, C.E.M.; Burden, A.D.; et al. Comparison of Drug Discontinuation, Effectiveness, and Safety Between Clinical Trial Eligible and Ineligible Patients in BADBIR. JAMA Dermatol. 2018, 154, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Mok, C.C.; Chan, K.Y.; Lee, K.L.; Tam, L.S.; Lee, K.W.; Hong Kong Society of Rheumatology. Factors associated with withdrawal of the anti-TNFα biologics in the treatment of rheumatic diseases: Data from the Hong Kong Biologics Registry. Int. J. Rheum. Dis. 2014, 17 (Suppl. S3), 1–8. [Google Scholar] [CrossRef] [PubMed]
- Nossent, H.C.; Bakland, G.; Aslaksen, H.K.; Olsen, G.; Nordvåg, B.Y. Efficacy of methylprednisolone pulse therapy versus infliximab in the treatment of severe flares of chronic polyarthritis. Scand. J. Rheumatol. 2001, 30, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Sakai, R.; Tanaka, M.; Nanki, T.; Watanabe, K.; Yamazaki, H.; Koike, R.; Nagasawa, H.; Amano, K.; Saito, K.; Tanaka, Y.; et al. Drug retention rates and relevant risk factors for drug discontinuation due to adverse events in rheumatoid arthritis patients receiving anticytokine therapy with different target molecules. Ann. Rheum. Dis. 2012, 71, 1820–1826. [Google Scholar] [CrossRef] [PubMed]
- Rennard, S.I.; Flavin, S.K.; Agarwal, P.K.; Lo, K.H.; Barnathan, E.S. Long-term safety study of infliximab in moderate-to-severe chronic obstructive pulmonary disease. Respir. Med. 2013, 107, 424–432. [Google Scholar] [CrossRef]
- Driessen, R.J.; Boezeman, J.B.; van de Kerkhof, P.C.; de Jong, E.M. Three-year registry data on biological treatment for psoriasis: The influence of patient characteristics on treatment outcome. Br. J. Dermatol. 2009, 160, 670–675. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).