1. Introduction
Bruxism, which is defined as “repetitive jaw muscular activity characterized by the clenching or grinding of teeth and/or bracing or thrusting of the mandible,” leads to changes in masseter muscle morphology [
1]. These changes include inflammation and hypertrophy of the muscles, chronic local muscular contracture, and myofascial pain. Despite recent advances in the treatment and rehabilitation of bruxism and masseter muscle diseases, the question of an effective treatment or rehabilitation approach is still unanswered. Medical professionals are engaged in finding novel treatments, rehabilitation protocols, and techniques that could optimize rehabilitation time and advance healing. One of the most important underlying principles in a successful treatment is performing correct medical diagnosis and assessment [
2,
3,
4]. Ultrasonography (USG) is frequently used in the medical imaging of bruxism [
5]. USG has several advantages: it is portable, does not use ionizing radiation, is cost-effective, and provides instantaneous imaging [
6].
The field of medical imaging, including USG, has experienced significant advancements in recent years via the utilization of artificial intelligence (AI). This has facilitated the creation of an image analysis methodology that is data-driven and relies on models that are less biased compared to traditional approaches, which heavily rely on heuristic assumptions regarding the appearance of objects. Machine learning (ML) is a subdomain of AI wherein machines acquire the ability to do a particular job by focusing on the identification of patterns within existing data through mathematical analysis of accessible datasets via the utilization of algorithms, rather than relying on explicit programming with predetermined instructions [
7,
8]. These algorithms subsequently undergo self-training processes to learn from the data and provide predictions based on newly acquired information [
9,
10]. This has resulted in improved cost-effectiveness, time efficiency, less reliance on human expertise, and a reduction in medical errors [
4,
11,
12,
13] and has provided assistance in making precise diagnoses [
14,
15,
16].
Radiomics is an emerging field that focuses on the creation of relevant statistical models using a substantial quantity of high-dimensional extractable features derived from medical imaging data. These features may be used in conjunction with genomic or clinical data to enhance diagnostic, prognostic, and treatment monitoring processes [
17]. In radiomics, a statistical model is constructed using ML algorithms based on specific biological or clinical inquiries and any existing prior knowledge [
18,
19]. Radiomics platforms have the potential to discover unique imaging algorithms for quantifying radiographic features including intensity, shape, and texture that enable prognostic, predictive imaging modalities to be built [
19]. Moreover, log-linear regression (LOG) features can also be used for generating AI models using radiomics to improve predicted outcomes from a linear regression model [
20].
USG-based machine learning techniques have gained significant importance in medical diagnostics. However, investigations of USG-based machine learning models used in the prediction of bruxism treatments are scanty and have not generated a validated and established prediction model [
4].
Therefore, this study aimed to (1) develop a USG-based ML model to distinguish the masseter muscles in patients with bruxism compared to normal subjects and (2) predict the treatment outcome for pain reduction among bruxism patients from various treatment modalities, with validation of the predictive accuracy and clinical efficacy of learning model based on pre- and post-treatment USG images and clinical evaluations.
This study has two hypotheses; the first hypothesis of this study (H1) is that USG-based ML can distinguish the masseter muscles in patients with bruxism compared to normal subjects. The second hypothesis (H2) is that the treatment outcome for pain reduction among bruxism patients can be predicted via USG-based ML from various treatment modalities.
The primary hypothesis herein was that balance and functional mobility would improve following PFEs in patients with SCP.
2. Materials and Methods
The Research Ethics Committee of Gazi University (Reference no: 2022-321) approved this retrospective analysis of anonymous data and waived the requirement for informed consent. The protocol for the study was in accordance with the guidelines of the Declaration of Helsinki.
The retrospective data of patients were included if they were older than 18 years of age and had been diagnosed with bruxism. Exclusion criteria were the absence of more than two molar teeth; treatment with removable partial dentures; neurological, psychiatric, or systemic diseases; alcohol and/or drug addiction; ongoing dental or physical therapy; the use of an occlusal splint during assessment; pregnancy; active cancer; or planned surgical procedures. Patients were also excluded if they had problems with their molar teeth, such as pericoronitis or supraeruption, and if they had been treated for temporomandibular disorders in the previous three months.
The study population consisted of 102 participants who were admitted to Ankara University Faculty of Dentistry with reported teeth grinding during sleep. Bruxism was diagnosed through self-report and clinical examination. In addition to the patients’ self-reports, dental wear consistent with attrition and clinical signs and symptoms such as jaw muscle discomfort, fatigue, and/or pain upon palpation were evaluated. Neither polysomnography nor electromyography were used. The Fonseca Anamnestic Index was employed for self-reporting as employed by Cavallo et al. [
21] for the diagnosis of bruxism; it can also be used to diagnose temporomandibular joint dysfunction [
22]. The index can provide relevant information in a short period and can be understood easily, allowing patients to be categorized according to the severity of bruxism and/or temporomandibular joint disorder [
21,
22,
23,
24,
25,
26].
Out of 102 participants who applied to Ankara University Faculty of Dentistry, 78 participants were diagnosed with bruxism. When the remaining 24 participants were examined, it was determined that they did not actually have bruxism. Therefore, they were included in the control group.
2.1. Outcome Variables
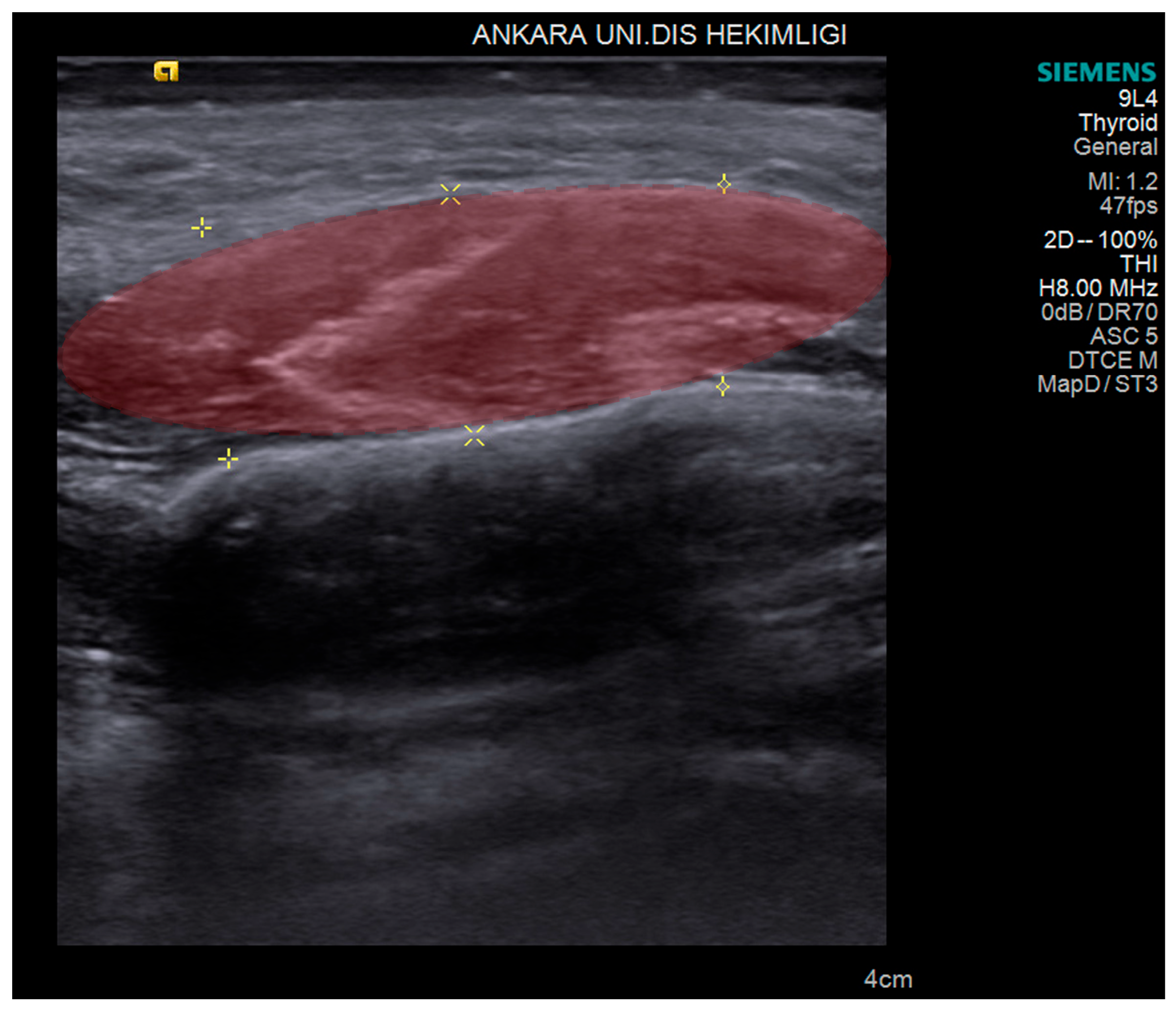
The primary outcome was to distinguish the masseter muscles of the bruxism patients from control subjects by generating an ML algorithm. The secondary outcome was to predict treatment outcomes for pain reduction among bruxism patients from various treatment modalities that were derived from pre- and post-treatment USG images and clinical evaluations. The USG image of masseter muscle thickness measurements before and after treatment are shown in
Figure 1.
2.2. USG Imaging
Two USG consoles, the ProSound Alpha 6 (Hitachi Aloka Medical Ltd., Tokyo, Japan) with a linear probe 5–13.3 MHz (UST-5413, Hitachi Aloka Medical Ltd., Tokyo, Japan) and the high-resolution ACUSON S 2000 ultrasound machine (Siemens, Munich, Germany) with a 4–9 MHz linear probe (9L4 Transducer), were used in this study. Extraoral scanning was performed with different frequency bandwidths. After adjusting the probe to the desired trajectory, images were obtained using both probes. Two ultrasonographers (C.E., K.O.) performed all USG scanning and interpretations. Both ultrasonographers were dentomaxillofacial radiologists with 10 and 5 years of experience in acquiring and interpreting USG. They were blinded to the bruxism or control status of the participants being examined.
During the USG procedure, the patient’s head was adjusted to the measured side. Imaging was performed by holding the probe perpendicular to the masseter muscles close to the level of the occlusal plane, approximately in the middle of the mediolateral distance of the ramus, taking care to keep the probe perpendicular to the ramus. The probe was moved in the anterior–posterior direction to produce transverse sections. The operators were free to position the probe when acquiring the images.
As USG scanning is a dynamic modality, we acquired USG images consecutively frame by frame to have as many images as possible from the anatomical region of both left and right masseter muscles, to be used later for both diagnosing and labeling. In total we obtained 623 USG images from 102 patients.
The entire masseter muscle image set was stored in the USG device for further analysis (
Figure 1). The ultrasonographers each conducted 2 separate USG sessions independently for all participants, at baseline and following 4 weeks of treatment for bruxism patients and at the same times for the control group.
2.3. USG Image Segmentation
The thickness of the masseter muscles was measured on the stored USG images by a single radiologist (C.E.) who was blinded to the clinical status of the patients. Volumes of interest (VOIs) were delineated manually by the radiologist (
Figure 1). All contours were then reviewed by the senior radiologist (K.O). If a discrepancy in volume measurement exceeded 5%, the senior radiologist decided on the contours and border of the masseter muscles.
All 623 images were preprocessed to make them suitable for the AI model. Preprocessing included resizing, cropping, padding, rotating, and augmenting the images to make them uniform, as well as reduction in noise and variation and the avoidance of overfitting. We created a standardization protocol by transforming the pixel values to make them compatible with the input range and distribution of the AI model. After this step-in total, 235 VOIs were delineated from 623 USG images for model creation.
2.4. Treatment Protocols of Patients
Patients with bruxism were treated in one of three protocols. (1) Manual therapy (MT) consisted of kneading, friction, intramuscular stretching, sliding, and ischemic compression on trigger points, applied on the masseter and temporalis muscles intra- and extraorally. Stretching exercises and cervical mobilization techniques were also performed. (2) In some patients, application of Kinesio Tape was combined with manual therapy (KTMT), in which web-cut strips of epidermis-dermis-fascia (EDF) KT were crossed over the masseter muscle area with 0–5% tension in the maximum stretched epidermis position. Kinesio Tape was applied immediately after MT and removed one day before the physiotherapy session, leaving it in place for at least 2 days [
27]. In the MT and KTMT treatments, each session lasted 30 min and was performed by a physiotherapist who had a Master Certification in manual therapy. (3) In the third protocol, Botulinum Toxin-A (BT-A) was injected into the masseter muscles for pain reduction and reduction in bruxism effects. All patients were informed of the possible side effects of the BT-A injection, and written signed consent forms were collected from them. For a dose of 1.0 U/0.1 mL, 100 U frozen dried BT-A (Botox, Allergan, Inc., Irvine, CA, USA) was diluted with 2 cc saline, and 30-gauge injectors were used for all the injections. The patients were positioned horizontally according to the Frankfurt horizontal plane. All injections were performed by the same clinician (N.B.). A dose of 25 U for each masseter muscle (total of 50 U for each patient) was injected. Only one session of application was performed. The 78 bruxism patients were classified into these 3 treatment subgroups: 20 in the MT subgroup, 19 in the KTMT subgroup, and 39 in the BT-A subgroup.
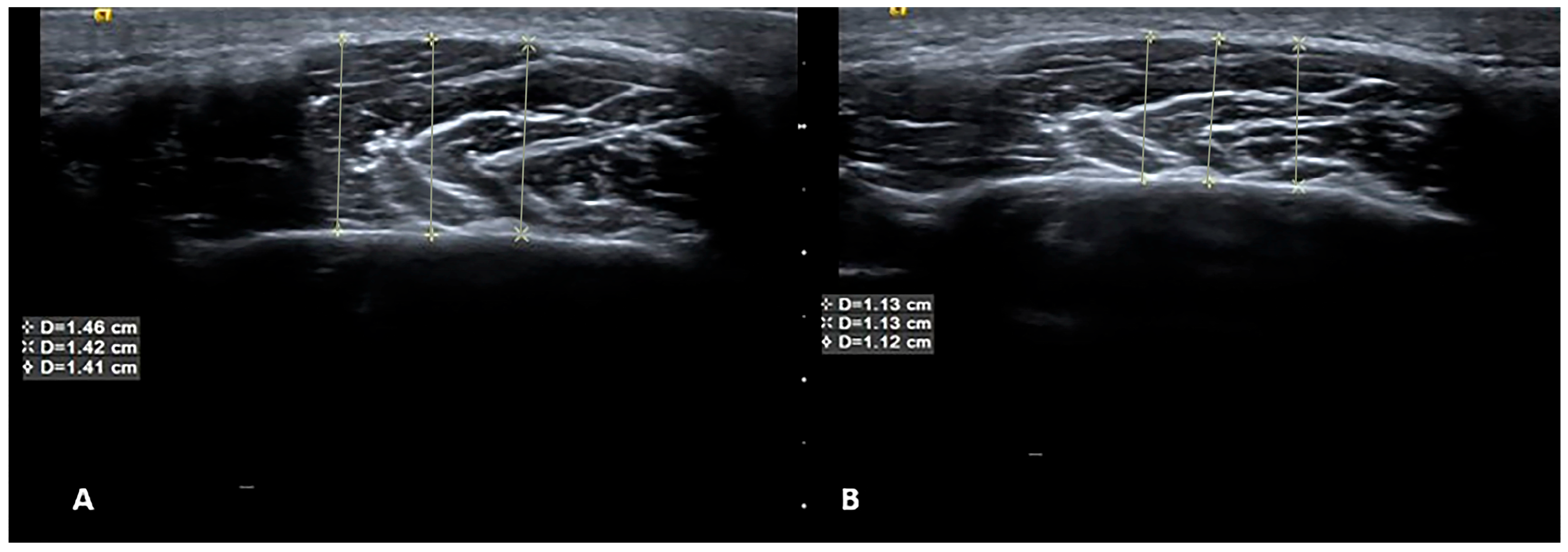
Age, sex, and body mass index were recorded for all participants in the patient and control groups. Maximum mouth opening, pain (visual analog score), pain on palpation, and sleep quality index (using the Pittsburg quality index) [
28] were also assessed with scales regarding the associated symptoms. Pain thresholds were evaluated using an algometer (Lafayette Model 01165A, Lafayette Instrument Company, Inc., Lafayette, IN, USA). Evaluations of all participants were performed at baseline and following 4 weeks of different physiotherapy applications and at the same times for the control group. USG images and clinical information were included in the analysis. An example of USG at baseline and 4 weeks after BT-A therapy is presented in
Figure 2.
2.5. Radiomics Evaluation
A radiomics platform (Huiying Medical Technology Co., Ltd., Beijing, China,
http://en.huiyihuiying.com/, accessed on 23 April 2024) was used to manage imaging data, clinical data, and subsequent radiomics statistical analysis. This platform is capable of extracting radiomics features from 2D and 3D images and binary masks on different imaging modalities. In this research, the training dataset and test dataset were separated by the random method with ratio 8:2, with 782 randomly sampled seeds.
2.6. Feature Extraction
In total, 2818 quantitative imaging features were extracted from USG images with the Radcloud platform (
http://radcloud.cn/, accessed on 23 April 2024) in 3 groups. Group 1 (first-order statistics) comprised descriptors that quantitatively describe the distribution of voxel intensities in the image using basic and commonly used metrics. Group 2 (shape- and size-based features) included three-dimensional characteristics reflecting the shape and size of the region. Group 3 (texture features) were calculated from gray level co-occurrence and gray level run-length texture matrices, which can quantify regional heterogeneity differences. Texture features containing gray level co-occurrence matrix (GLCM) and gray level size zone matrix (GLSZM) were used. Intensity and texture features can be calculated on the original image and derived images, obtained by applying several filters such as exponential, logarithm, square, square root, and wavelet (wavelet-LHL, wavelet-L, wave-let-HLL, wavelet-LLH, wavelet-HLH, wavelet- HHH, wavelet-HHL, wavelet-LLL). After image segmentation, the identified radiomics features were calculated and associated with features for masseter muscle identification and bruxism treatment prediction from USG images (
Table 1). The features complied with definitions established by the Imaging Biomarker Standardization Initiative (IBSI) [
29].
For feature extraction, dimensionality reduction and selection of task-specific features for best performance were performed. To reduce the redundant features, the feature selection methods included the variance threshold. SelectKBest and the least absolute shrinkage and selection operator (LASSO) were used for this purpose. With the variance threshold set at 0.8, eigenvalues of the variance smaller than 0.8 were removed. The SelectKBest method, which belongs to a single variable feature selection method, used the p-value to analyze the relationship between the features and the classification results; all features with p-values smaller than 0.05 were used. For the LASSO model, ‘L1 regularize’ was used as the cost function. The error value of the cross test was 5, and the maximum number of iterations was 1000.
2.7. Consensus Clustering
A consensus clustering was also used for clustering the radiomics features after extraction from the training sets. In this study, the range of a suitable amount of clusters was estimated. According to this range, the amount of clusters that produced the highest median cluster consensus compared to the other clusters was selected. The definition of cluster consensus was the average consensus among feature pairs that belong to the identical cluster.
Subsequent to clustering, integration of the chosen features with clinical variables was performed in order to construct a primary dataset with good stability and reliability. With regard to the other significant variables, the
p-value threshold was fixed at 0.05 [
30]. During the preliminary filtering stage, univariate analysis was employed for the purpose of filtering out multiple unconnected features, which allowed the optimal feature established via univariate analysis to be calculated.
2.8. Statistical and Machine Learning Analysis
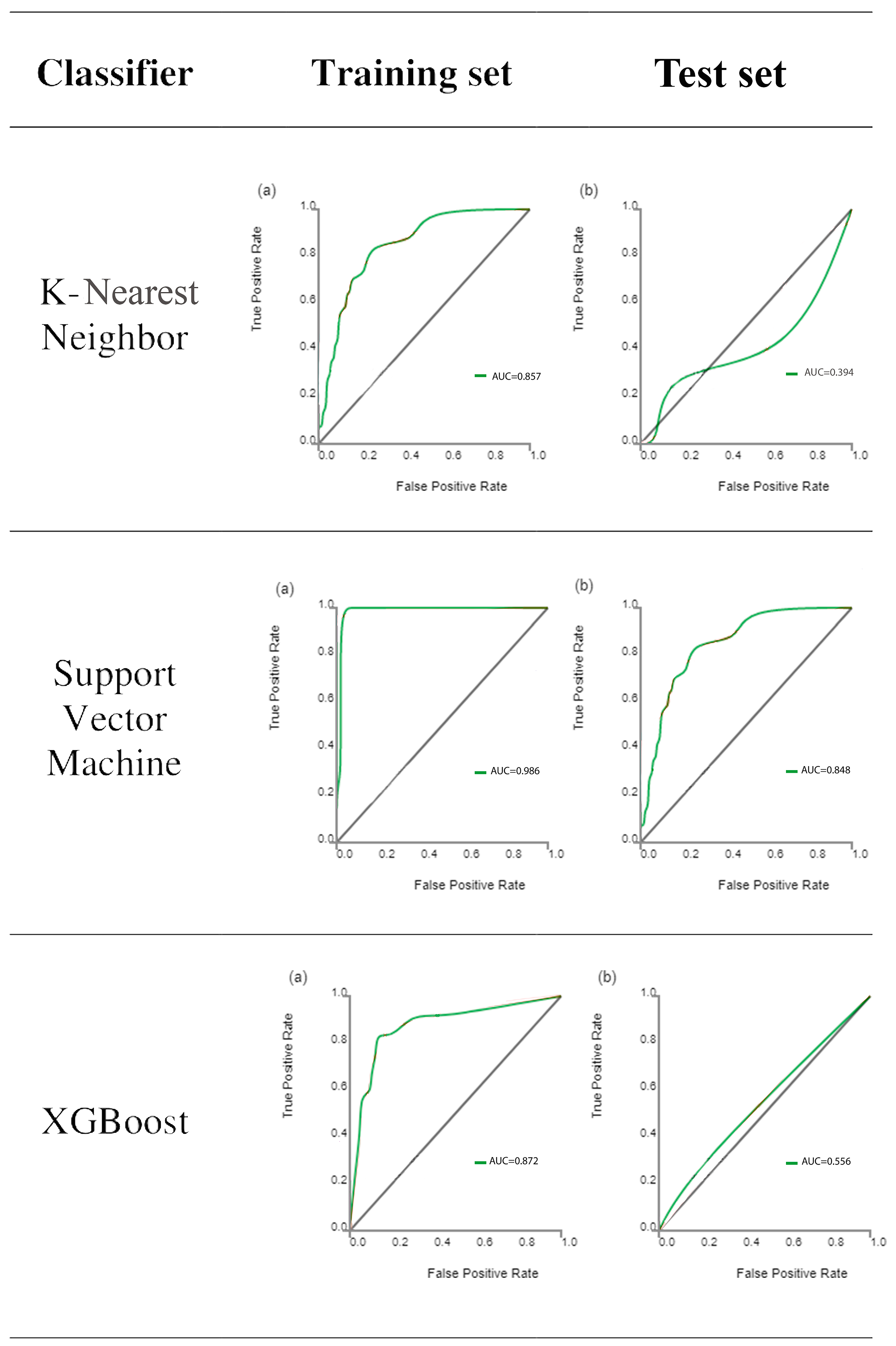
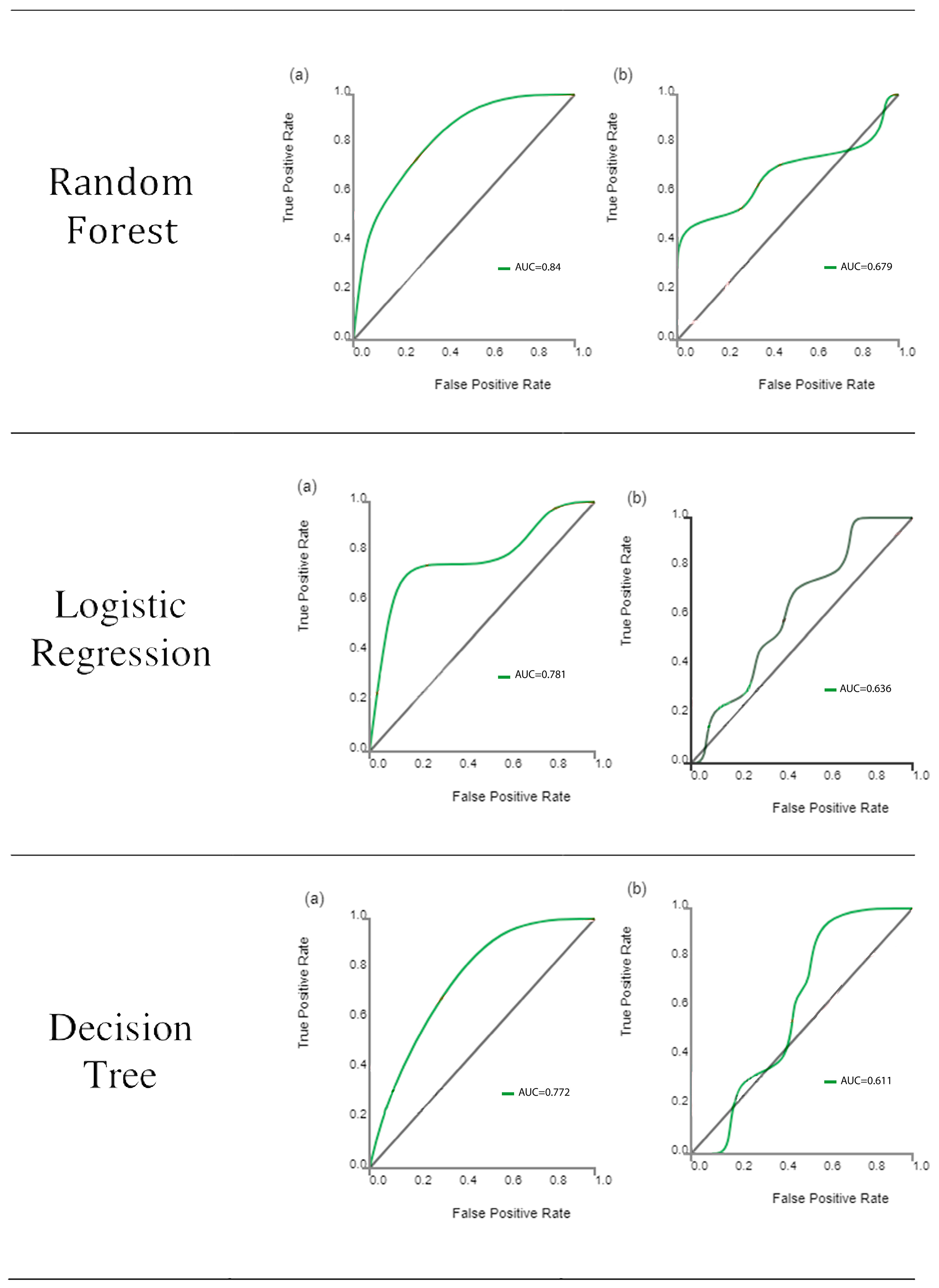
Computer-generated random numbers were used to assign 80% of the VOIs to the training dataset and 20% of VOIs to the test dataset. Based on the selected features, there are several supervised learning classifiers available for classification analysis, which creates models that attempt to separate or predict the data with respect to an outcome or phenotype (for instance, patient outcome or response). In this study, the radiomics-based models were constructed with 6 classifiers: k-Nearest Neighbor (KNN), Support Vector Machine (SVM), eXtreme Gradient Boosting (XGBoost), Random Forest (RF), Logistic Regression (LR), and Decision tree (DT). The test method was used to improve the effectiveness of the model. The best learning classifier was selected for testing the secondary outcome, defined as clinically reduced pain and bruxism conditions after treatment.
In order to calculate outcome measures, the ML classifiers must indicate if the USG image has texture features representing bruxism or control. The outcomes’ measures were based on the interpretation of the texture features as disease or control compared to the actual known status of the patient. To assess the predictive performance, the area under curve (AUC) generated through receiver operating characteristic (ROC) analysis was used both in training and test datasets. The scale that was used to interpret the ability of the classifier to discriminate between two conditions designated AUC values of 0.5–0.7 as poor discrimination, 0.7–0.8 as acceptable discrimination, 0.8–0.9 as excellent discrimination, and >0.9 as outstanding discrimination [
30]. Sensitivity and specificity values were also calculated. In addition, four other indicators were calculated to evaluate the performance of the classifiers in this study: precision (P) = true positives/(true positives + false positives), recall (R) = true positives/(true positives + false negatives), F1 = 2 * (precision * recall)/(precision + recall), and support, which was defined as the number of samples of the true response that lies in each class of target values.
Statistical differences between the predictive radiomics features of the models were tested using the Mann–Whitney U test in relation to outcomes for pain reduction. Statistical analyses were performed using IBM SPSS Statistics package 21.0 (IBM Corp. Released 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY, USA: IBM Corp). A p-value was considered to be statistically significant if less than 0.05.
4. Discussion
In this study, we aimed to develop a predictive model for the outcome of bruxism treatments using USG-based machine learning techniques. The findings of this study showed that the presence of bruxism can be detected via a USG-based machine learning technique. Furthermore, the outcome of pain reduction can also be predicted via combined ML models. After a series of steps involving dimensionality reduction and feature selection, a set of six optimal radiomics features were identified for the machine learning model. The selected features were derived from both first-order statistics and shape-based descriptors. The machine learning classifiers demonstrated reasonable performance in differentiating between bruxism patients’ masseter muscles and those of normal subjects, as indicated by the AUC values. However, it is important to note that the AUC values varied between the training and test datasets, indicating the need for further validation and improvement. Moreover, we evaluated the predictive performance of our models for all patients, including the secondary outcome of pain reduction. The best learning classifier (SVM) was selected for this evaluation, and the combined features (clinical and radiomics) were used. The results showed associations between poor outcomes for pain reduction and factors such as age and specific treatment procedures, as identified by the clinical and radiomic models. These findings highlight the potential of combining clinical and radiomic features in predicting treatment outcomes and assessing pain reduction in bruxism patients.
Bruxism, which is very common in society, causes serious problems affecting the maxillofacial region such as maxillofacial pain, limitation in mouth opening, and decreased function in the temporomandibular joint. Since bruxism causes different problems in different regions, especially the results mentioned, bruxism patients should be approached in a multidisciplinary manner. Therefore, bruxism patients should be examined multidisciplinarily by psychiatrists, dentists, and physiotherapists [
24,
25]. In bruxism patients, the treatment is directed to the agent and the symptom. Bruxism can cause masticatory muscle hypertrophy, particularly in the masseter muscle. Manual therapy, Kinesio Tape, and BT-A are muscle-oriented treatments used in the treatment of bruxism [
21,
26].
Ultrasound can be used to evaluate masseter muscle volume, size, hypertrophy, and stiffness in patients with bruxism. In our study, ultrasound images before and after bruxism treatment were evaluated. Additionally, the ultrasonographic evaluation of the effect of some therapy methods on masseter muscle and blood flow in patients with bruxism, supports the potential benefits of physical interventions in managing bruxism symptoms [
3]. These findings align with our study’s focus on predicting treatment outcomes and suggest that interventions can have positive effects on muscle parameters. With the findings of our study, the evaluation of the success of treatment methods for bruxism patients are not only based on subjective or quantitative concepts but can now also be confirmed with ultrasound images and radiomics. This will provide motivation for the patient and objective treatment prediction for the physician.
In this study, the muscles of bruxism patients before and after treatment were evaluated with radiomics. There are very few radiomic studies in bruxism in the literature yet. Although the publications using radiomic features are increasing day by day in the literature, there is no consensus on which of these radiomic features are reproducible [
32]. The findings of the present study will provide valuable insights into the future opportunities of muscle ultrasound in various clinical contexts and for other populations. Images are transformed to look for correlations that may identify a useful radiographic phenotype before, during, or after treatment [
33,
34]. The most common use of ultrasound-based radiomic studies is to differentiate between benign and malignant tumors. There are many radiomic studies used for this purpose in structures such as breast and liver, especially in thyroid tissue [
35,
36,
37]. There are many radiomic studies evaluating tumoral lesions in the literature, including a study by Lee et al., in which they aimed to distinguish triple-negative breast cancer from fibroadenoma using tissue analysis, and another by Zhang et al., in which they extracted radiomic features from 2064 pathologically confirmed B-mode and elastography images of thyroid nodules [
38,
39].
This review provides valuable insights into the present state and future opportunities of muscle ultrasound. It highlights the diverse applications of ultrasound imaging in assessing muscle morphology, architecture, and function [
40]. Incorporating the knowledge and advancements discussed in this review can further enhance the interpretation and application of ultrasound-based machine learning techniques in our study. In the context of muscle segmentation, deep learning (DL) and atlas-based models have shown promise in medical image analysis. Studies like (Chen et al.) [
41] and (Keser et al.) [
42] utilized DL approaches for fast auto-segmentation of masticatory muscles on head and neck CT images and masseter muscle segmentation on ultrasonography, respectively. These approaches can contribute to improving the accuracy and reliability of muscle segmentation in our predictive model, thereby enhancing its overall performance.
Studies using ultrasound radiomic modeling in the field of health have been frequently seen in the literature recently. It is noteworthy that there are studies on cancer in general. A study on bruxism has not been conducted, to the best of our knowledge. Although not directly related to bruxism, the study by Saleh et al. on a DL localization method for measuring abdominal muscle dimensions in ultrasound images is relevant to our research [
43]. Their DL approach for muscle segmentation in ultrasound images can enhance the accuracy and efficiency of our predictive model, as precise delineation of muscle boundaries is essential for accurate measurements and analysis. In a study by Qin et al. [
44] in which they developed B-mode ultrasound radiomic models to identify the origin of primary tumors in metastatic liver disease with satisfactory AUC values reflected in the training and test sets, a total of 5936 features were extracted, and 40, 6, and 14 optimal features were sequentially identified for the development of radiomic models for groups 1, 2, and 3, respectively, with training set AUC values of 0.938, 0.974, and 0.768 and testing set AUC values of 0.767, 0.768, and 0.750. These values are close to our study. Qin et al. emphasized that B-mode ultrasound radiomic models can be effective additional tools to identify the source of hepatic metastatic lesions [
44]. In the literature, there are also ultrasound-based radiomic studies examining the texture and content of the tissues, as well as the differentiation of benign malignant tumoral lesions. For example, there are many studies evaluating liver fibrosis [
45,
46,
47].
Overall, our study highlights the potential of USG-based machine learning models in predicting the outcome of bruxism treatments. The identified radiomic features, along with clinical factors, can contribute to a comprehensive assessment of treatment outcomes. It is important to note that these findings are based on the specific dataset and methodology employed in this study, and further research is needed to validate and generalize these results.
Nonetheless, the current study has some limitations. The major limitations of this study are its retrospective design and limited number of study population. Additionally, the study population was restricted to a single institution. With larger cohorts, those results might be stronger. The size of AI training datasets is critical for machine learning projects. To define the optimal amount of data you need, you have to consider a lot of factors, including project type, algorithm and model complexity, error margin, and input diversity. In this study, we aimed to apply the 10 times rule. In our study, there were nine clinical parameters plus USG, making a total of 10 parameters. Out of these 10 clinical parameters, our aim was to construct an ML algorithm to predict the outcome variables according to the 10-times rule. This rule means that the amount of input data (i.e., the number of examples) should be ten times more than the number of degrees of freedom a model has. Usually, degrees of freedom mean parameters in the dataset. Therefore, our AI training set should be at least 100 patients or images. Our clinical dataset consists of 102 patients. This is thought to be enough to construct an algorithm for prediction. Nevertheless, it should be stated that the more data, the better it is for ML studies.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}