
Risk Factors for Isolated Sphenoid Sinusitis after Endoscopic Endonasal Transsphenoidal Pituitary Surgery

 , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Surgical Treatment and Postoperative Regimen
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Risk Factors for Postoperative Sinusitis
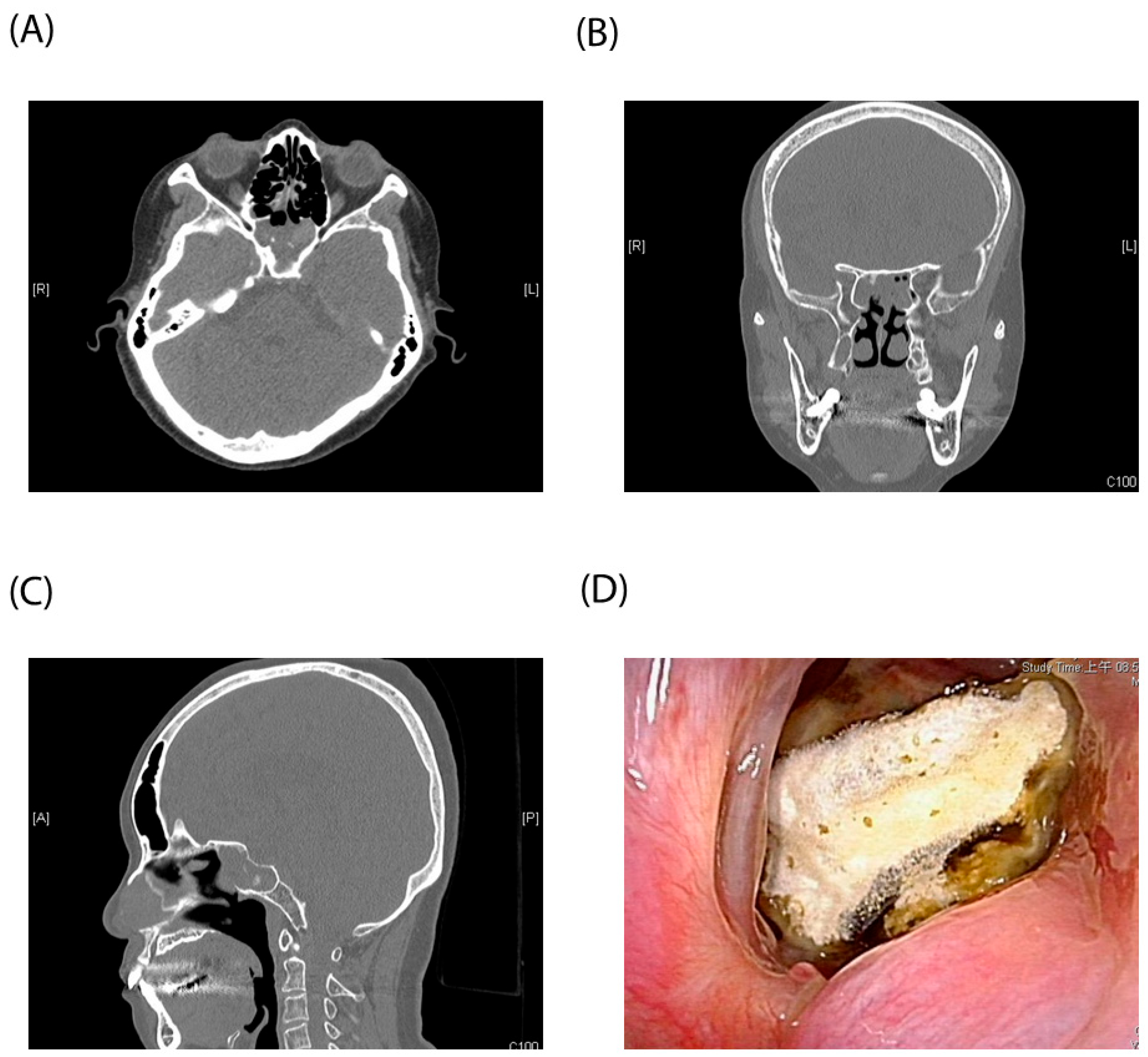
3.3. Case Illustration
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buchfelder, M. Treatment of pituitary tumors: Surgery. Endocrine 2005, 28, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Mortini, P.; Barzaghi, L.R.; Albano, L.; Panni, P.; Losa, M. Microsurgical therapy of pituitary adenomas. Endocrine 2018, 59, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Rolston, J.D.; Han, S.J.; Aghi, M.K. Nationwide shift from microscopic to endoscopic transsphenoidal pituitary surgery. Pituitary 2016, 19, 248–250. [Google Scholar] [CrossRef] [PubMed]
- Moeller, C.W.; Welch, K.C. Prevention and management of complications in sphenoidotomy. Otolaryngol. Clin. N. Am. 2010, 43, 839–854. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.W. Complications of sphenoid sinus surgery and transsphenoidal hypophysectomy. Oper. Tech. Otolaryngol. Head Neck Surg. 2003, 14, 219–220. [Google Scholar] [CrossRef]
- Batra, P.S.; Citardi, M.J.; Lanza, D.C. Isolated sphenoid sinusitis after transsphenoidal hypophysectomy. Am. J. Rhinol. 2005, 19, 185–189. [Google Scholar] [CrossRef]
- Lu, Y.J.; Chang, C.N.; Pai, P.C.; Wei, K.C.; Chuang, C.C. Isolated sphenoid sinusitis or mucocele: A potential complication of endonasal transsphenoidal surgery. J. Neurooncol. 2009, 91, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Cappabianca, P.; Cavallo, L.M.; Solari, D.; Stagno, V.; Esposito, F.; de Angelis, M. Endoscopic Endonasal Surgery for Pituitary Adenomas. World Neurosurg. 2014, 82, S3–S11. [Google Scholar] [CrossRef]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; Wiley: Hoboken, NJ, USA, 2013. [Google Scholar] [CrossRef]
- Mavromati, M.; Mavrakanas, T.; Jornayvaz, F.R.; Schaller, K.; Fitsiori, A.; Vargas, M.I.; Lobrinus, J.A.; Merkler, D.; Egervari, K.; Philippe, J.; et al. The impact of transsphenoidal surgery on pituitary function in patients with non-functioning macroadenomas. Endocrine 2023, 81, 340–348. [Google Scholar] [CrossRef]
- Daly, A.F.; Rixhon, M.; Adam, C.; Dempegioti, A.; Tichomirowa, M.A.; Beckers, A. High prevalence of pituitary adenomas: A cross-sectional study in the province of Liege, Belgium. J. Clin. Endocrinol. Metab. 2006, 91, 4769–4775. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, A.; Karavitaki, N.; Wass, J.A. Prevalence of pituitary adenomas: A community-based, cross-sectional study in Banbury (Oxfordshire, UK). Clin. Endocrinol. 2010, 72, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Chanson, P.; Raverot, G.; Castinetti, F.; Cortet-Rudelli, C.; Galland, F.; Salenave, S. Management of clinically non-functioning pituitary adenoma. Ann. Endocrinol. 2015, 76, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Buurman, H.; Saeger, W. Subclinical adenomas in postmortem pituitaries: Classification and correlations to clinical data. Eur. J. Endocrinol. 2006, 154, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Vieira, L.N.; Boguszewski, C.L.; Araújo, L.A.; Bronstein, M.D.; Miranda, P.A.; Musolino, N.R.; Naves, L.A.; Vilar, L.; Ribeiro-Oliveira, A.J.; Gadelha, M.R. A review on the diagnosis and treatment of patients with clinically nonfunctioning pituitary adenoma by the Neuroendocrinology Department of the Brazilian Society of Endocrinology and Metabolism. Arch. Endocrinol. Metab. 2016, 60, 374–390. [Google Scholar] [CrossRef] [PubMed]
- Freda, P.U.; Beckers, A.M.; Katznelson, L.; Molitch, M.E.; Montori, V.M.; Post, K.D.; Vance, M.L. Pituitary incidentaloma: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 894–904. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, H.; Ramm-Pettersen, J.; Josefsen, R.; Rønning, P.; Reinlie, S.; Meling, T.; Berg-Johnsen, J.; Bollerslev, J.; Helseth, E. Surgical complications after transsphenoidal microscopic and endoscopic surgery for pituitary adenoma: A consecutive series of 506 procedures. Acta Neurochir. 2014, 156, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.M.; Park, Y.K.; Ko, S.-W.; Han, K.; Ko, Y. Single-surgeon endoscopic endonasal transsphenoidal surgery for pituitary adenomas: Surgical outcomes and complications of 197 cases. J. Korean Skull Base Soc. 2022, 17, 75–85. [Google Scholar] [CrossRef]
- Abhinav, K.; Tyler, M.; Dale, O.T.; Mohyeldin, A.; Fernandez-Miranda, J.C.; Katznelson, L. Managing complications of endoscopic transsphenoidal surgery in pituitary adenomas. Expert Rev. Endocrinol. Metab. 2020, 15, 311–319. [Google Scholar] [CrossRef]
- Cheng, Y.; Xue, F.; Wang, T.Y.; Ji, J.F.; Chen, W.; Wang, Z.Y.; Xu, L.; Hang, C.H.; Liu, X.F. Analyses and treatments of postoperative nasal complications after endonasal transsphenoidal resection of pituitary neoplasms. Medicine 2017, 96, e6614. [Google Scholar] [CrossRef]
- Brook, I. Acute and chronic bacterial sinusitis. Infect. Dis. Clin. N. Am. 2007, 21, 427–448. [Google Scholar] [CrossRef] [PubMed]
- Turgut, S.; Ozcan, K.M.; Celikkanat, S.; Ozdem, C. Isolated sphenoid sinusitis. Rhinology 1997, 35, 132–135. [Google Scholar] [PubMed]
- Kumar, A.; Gupta, K.; Tyagi, A.K.; Varshney, S.; Kumar, N. Isolated Acute Sphenoid Fungal Sinusitis with Cavernous Sinus Thrombosis: Our Experience. Indian J. Otolaryngol. Head Neck Surg. 2022, 74, 987–993. [Google Scholar] [CrossRef]
- Moss, W.J.; Finegersh, A.; Jafari, A.; Panuganti, B.; Coffey, C.S.; DeConde, A.; Husseman, J. Isolated sphenoid sinus opacifications: A systematic review and meta-analysis. Int. Forum Allergy Rhinol. 2017, 7, 1201–1206. [Google Scholar] [CrossRef]
- Sethi, D.S. Isolated sphenoid lesions: Diagnosis and management. Otolaryngol. Head Neck Surg. 1999, 120, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Yap, H.J.; Ramli, R.R.; Yeoh, Z.X.; Sachlin, I.S. Series of isolated sphenoid disease: Often neglected but perilous. SAGE Open Med. Case Rep. 2022, 10, 2050313X221097757. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.J.; Lee, H.; Oh, J.; Chang, J.H. Isolated Fungal Sphenoid Sinusitis after Endonasal Transsphenoidal Approach. Ear Nose Throat J. 2022, 101, NP238–NP239. [Google Scholar] [CrossRef]
- Sajko, T.; Gnjidić, Ž.; Sesar, N.; Malenica, M. Sphenoid sinus aspergilloma in trans-sphenoidal surgery for pituitary adenomas. Acta Neurochir. 2015, 157, 1345–1351; discussion 1351. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Lee, E.J. Endoscopic Findings of Fungal Ball in the Mucocele after Endonasal Transsphenoidal Surgery. Ear Nose Throat J. 2021, 100, NP169–NP170. [Google Scholar] [CrossRef]
- Fleseriu, M.; Karavitaki, N. Non-functioning pituitary adenomas, not all the same and certainly not boring! Pituitary 2018, 21, 109–110. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Sinusitis (n = 17) | No Sinusitis (n = 186) | p Value |
|---|---|---|---|
| Male | 6 | 97 | 0.184 |
| Age | 55.1 (41–69.2) | 53.5 (39.7–67.3) | 0.649 |
| DM | 4 (23.5) | 32 (17.2) | 0.514 |
| Smoking | 0 (0) | 1 (5.3) | 1.000 |
| Nonfunctioning pituitary adenoma | 9 (52.9) | 53 (28.5) | 0.037 * |
| Nasoseptal flap preparation | 4 (23.5) | 54 (29.0) | 0.343 |
| Preoperative cortisol level | 5.4 (1.6–9.4) | 8.7 (7.4–9.7) | 0.024 * |
| Postoperative cortisol level | 4.3 (2.1–7.3) | 7.4 (6.8–8.4) | 0.014 * |
| WBC (×103) | 7.4 (6.8–8.5) | 6.6 (6.3–6.9) | 0.223 |
| Eosinophil count | 110.5 (95.2–177.9) | 122 (99.7–136.3) | 0.611 |
| Tumor size (longest diameter, mm) | 14.8 (12.6–20.2) | 15.3 (13.9–24.3) | 0.462 |
| Variables | Coefficient | Odds Ratio | 95% CI | p Value |
|---|---|---|---|---|
| Nonfunctioning pituitary adenoma | 1.310 | 3.71 | 1.09–12.58 | 0.036 * |
| Postoperative cortisol level | −0.194 | 0.82 | 0.69–0.99 | 0.035 * |
| Preoperative cortisol level | - | - | 0.062 |
| Age/Gender | Pit-NET Type | Nasal Symptoms | Endoscopic Findings | Follow-Up Duration to Sinusitis (M) | Operation for Sinusitis | DM | Smoking | |
|---|---|---|---|---|---|---|---|---|
| Case 1 | 37/F | Nonfunctioning pit-NET | Foul odor and clear rhinorrhea | Mucopus over sphenoid sinus ostium | 1 | N | 1 | 0 |
| Case 2 | 63/F | Nonfunctioning pit-NET | None | Mucopus over sphenoid sinus ostium | 1 | N | 1 | 0 |
| Case 3 | 49/F | Nonfunctioning pit-NET | Purulent rhinorrhea | Mucopus over sphenoid sinus ostium | 3 | N | 0 | 0 |
| Case 4 | 58/M | Nonfunctioning pit-NET | Headache | Mucopus over sphenoid sinus ostium | 1 | N | 0 | 0 |
| Case 5 | 77/F | Functioning pit-NET | Right nasal obstruction | Mucopus over sphenoid sinus ostium | 1 | N | 0 | 0 |
| Case 6 | 39/F | Nonfunctioning pit-NET | Purulent rhinorrhea and post nasal dripping | Mucopus over sphenoid sinus ostium | 1 | N | 0 | 0 |
| Case 7 | 76/F | Nonfunctioning pit-NET | Blood-tinged sputum | Fungal ball over sphenoid sinus ostium | 2 | Y | 0 | 0 |
| Case 8 | 29/M | Functioning pit-NET | None | Fungal ball over sphenoid sinus ostium | 2 | N | 0 | 0 |
| Case 9 | 49/F | Functioning pit-NET | Nasal obstruction | NA (due to COVID pandemic) | 0.5 | N | 1 | 0 |
| Case 10 | 40/M | Nonfunctioning pit-NET | Purulent rhinorrhea | Polypoid change with mucopus over sphenoid sinus ostium | 1 | N | 0 | 0 |
| Case 11 | 74/F | Functioning pit-NET | None | Mucopus over sphenoid sinus ostium | 0.5 | Y | 0 | 0 |
| Case 12 | 54/M | Functioning pit-NET | Blood-tinged sputum | Fungal hyphae over sphenoid ostium | 1 | N | 0 | 0 |
| Case 13 | 68/F | Functioning pit-NET | None | Mucopus over sphenoid sinus ostium | 0.5 | N | 0 | 0 |
| Case 14 | 58/M | Nonfunctioning pit-NET | Foul odor | Stenosis of sphenoidotomy with mucopus | 2 | N | 0 | 0 |
| Case 15 | 53/F | Functioning pit-NET | Right periorbital pain and hyposmia | Right synechia and mucopus over sphenoid ostium | 1 | N | 0 | 0 |
| Case 16 | 50/F | Nonfunctioning pit-NET | Sputum and cough | Mucopus over sphenoid sinus ostium | 3 | N | 1 | 0 |
| Case 17 | 63/M | Functioning odd pit-NET | Purulent rhinorrhea | NA (due to COVID pandemic) | 1.5 | N | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.-C.; Tsao, Y.-N.; Chuang, C.-C.; Li, C.-Y.; Lee, T.-J.; Fu, C.-H.; Wei, K.-C.; Huang, C.-C. Risk Factors for Isolated Sphenoid Sinusitis after Endoscopic Endonasal Transsphenoidal Pituitary Surgery. Diagnostics 2024, 14, 758. https://doi.org/10.3390/diagnostics14070758
Chang Y-C, Tsao Y-N, Chuang C-C, Li C-Y, Lee T-J, Fu C-H, Wei K-C, Huang C-C. Risk Factors for Isolated Sphenoid Sinusitis after Endoscopic Endonasal Transsphenoidal Pituitary Surgery. Diagnostics. 2024; 14(7):758. https://doi.org/10.3390/diagnostics14070758
Chicago/Turabian StyleChang, Yun-Chen, Yu-Ning Tsao, Chi-Cheng Chuang, Cheng-Yu Li, Ta-Jen Lee, Chia-Hsiang Fu, Kuo-Chen Wei, and Chi-Che Huang. 2024. "Risk Factors for Isolated Sphenoid Sinusitis after Endoscopic Endonasal Transsphenoidal Pituitary Surgery" Diagnostics 14, no. 7: 758. https://doi.org/10.3390/diagnostics14070758
APA StyleChang, Y.-C., Tsao, Y.-N., Chuang, C.-C., Li, C.-Y., Lee, T.-J., Fu, C.-H., Wei, K.-C., & Huang, C.-C. (2024). Risk Factors for Isolated Sphenoid Sinusitis after Endoscopic Endonasal Transsphenoidal Pituitary Surgery. Diagnostics, 14(7), 758. https://doi.org/10.3390/diagnostics14070758