
Resistome Analysis of Klebsiella pneumoniae Complex from Residential Aged Care Facilities Demonstrates Intra-facility Clonal Spread of Multidrug-Resistant Isolates

 , , , ,
, , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Sampling
2.2. Isolation and Identification of K. pneumoniae
2.3. Antimicrobial Susceptibility Testing
2.4. Efflux Pump Inhibition Assays
2.5. Genomic DNA Isolation and Whole-Genome Sequencing
2.6. Bioinformatic and Statistical Analyses
2.7. Data Availability
2.8. Ethics Approval
3. Results
3.1. A Total of 147 K. pneumoniae Complex Isolates Were Identified
3.2. K. pneumoniae Complex Resistant to Ceftazidime, Ciprofloxacin and Trimethoprim-Sulfamethoxazole was Isolated
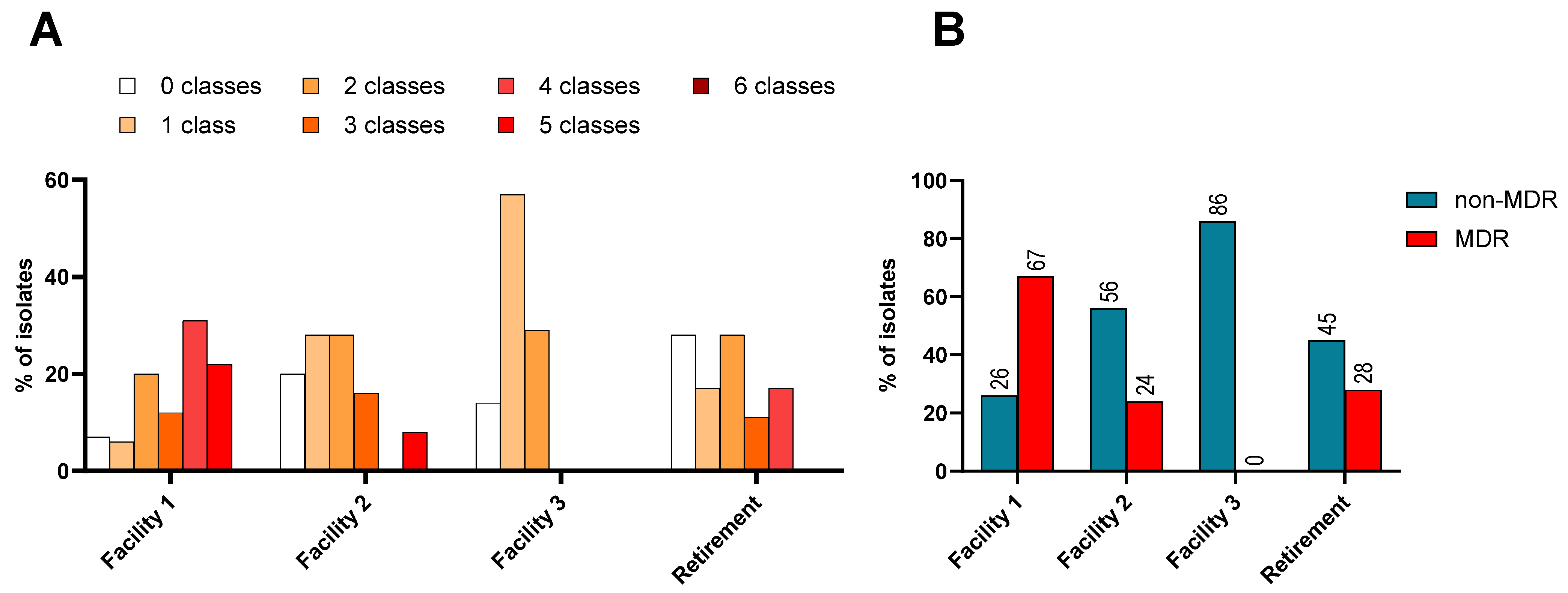
3.3. Multidrug Resistance (MDR) Was Prevalent within RACFs, Especially within Facility 1
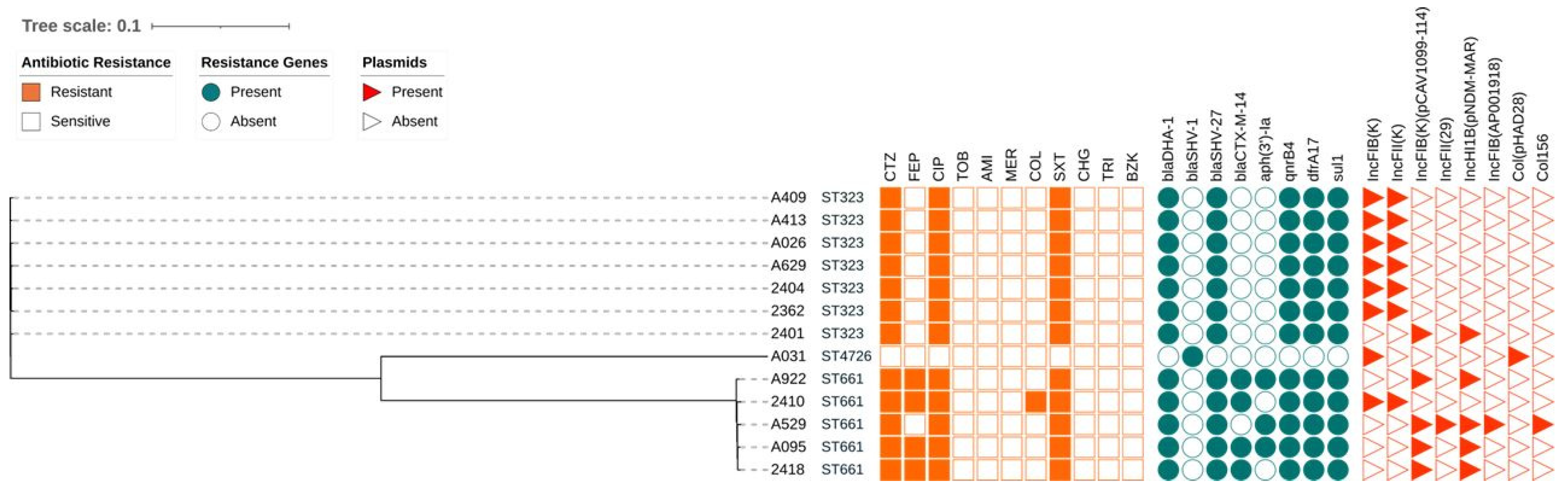
3.4. Resistome Analysis of a Subset of K. pneumoniae Complex Could Not Identify the Genomic Basis for the Cephalosporin or Colistin Resistance
3.5. Mutations in Genes Known to Confer Resistance to Antimicrobials
3.6. The Majority of the K. pneumoniae Complex Isolates were the MDR-Outbreak-Causing Sequence Type 323
3.7. Clonal Spread of K. pneumoniae within RACFs was Observed within Facility 1
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation (WHO). Antimicrobial Resistance Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 31 May 2022).
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J. Review on Antimicrobial Resistance. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. Wellcome Trust and HM Government. 2014. Available online: https://amr-review.org/sites/default/files/160525_Final%20paper_with%20cover.pdf (accessed on 1 March 2022).
- Dong, N.; Yang, X.; Chan, E.W.-C.; Zhang, R.; Chen, S. Klebsiella species: Taxonomy, hypervirulence and multidrug resistance. eBioMedicine 2022, 79, 103998. [Google Scholar] [CrossRef] [PubMed]
- Australian Group on Antimicrobial Resistance (AGAR). Antimicrobial Use and Resistance in Human Health in Australia (AURA) 2023 Fifth Australian Report on Antimicrobial Use and Resistance in Human Health; Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2021. Available online: https://www.safetyandquality.gov.au/sites/default/files/2023-11/aura_2023_fifth_australian_report_on_antimicrobial_use_and_resistance_in_human_health.pdf (accessed on 1 March 2024).
- Kareem, S.M.; Al-Kadmy, I.M.; Kazaal, S.S.; Mohammed Ali, A.N.; Aziz, S.N.; Makharita, R.R.; Algammal, A.M.; Al-Rejaie, S.; Behl, T.; Batiha, G.E.-S. Detection of gyrA and parC mutations and prevalence of plasmid-mediated quinolone resistance genes in Klebsiella pneumoniae. Infect. Drug Resist. 2021, 14, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.Y.; Nam, Y.S.; Lee, H.J. Prevalence of plasmid-mediated quinolone resistance genes among ciprofloxacin-nonsusceptible Escherichia coli and Klebsiella pneumoniae isolated from blood cultures in Korea. Can. J. Infect. Dis. Med. Microbiol. 2014, 25, 163–169. [Google Scholar] [CrossRef]
- Rocha, J.; Henriques, I.; Gomila, M.; Manaia, C.M. Common and distinctive genomic features of Klebsiella pneumoniae thriving in the natural environment or in clinical settings. Sci. Rep. 2022, 12, 10441. [Google Scholar] [CrossRef] [PubMed]
- Holt, K.E.; Wertheim, H.; Zadoks, R.N.; Baker, S.; Whitehouse, C.A.; Dance, D.; Jenney, A.; Connor, T.R.; Hsu, L.Y.; Severin, J.; et al. Genomic analysis of diversity, population structure, virulence, and antimicrobial resistance in Klebsiella pneumoniae, an urgent threat to public health. Proc. Natl. Acad. Sci. USA 2015, 112, E3574–E3581. [Google Scholar] [CrossRef] [PubMed]
- Bialek-Davenet, S.; Criscuolo, A.; Ailloud, F.; Passet, V.; Jones, L.; Delannoy-Vieillard, A.-S.; Garin, B.; Le Hello, S.; Arlet, G.; Nicolas-Chanoine, M.-H. Genomic definition of hypervirulent and multidrug-resistant Klebsiella pneumoniae clonal groups. Emerg. Infect. Dis. 2014, 20, 1812. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Chen, Q.; Shen, F.; Jiang, Y.; Wu, X.; Hua, X.; Fu, Y.; Yu, Y. Resistance Evolution of Hypervirulent Carbapenem-resistant Klebsiella pneumoniae ST11 during Treatment with Tigecycline and Polymyxin. Emerg. Microbes Infect. 2021, 10, 1129–1136. [Google Scholar] [CrossRef]
- Kaczmarek, F.M.; Dib-Hajj, F.; Shang, W.; Gootz, T.D. High-level carbapenem resistance in a Klebsiella pneumoniae clinical isolate is due to the combination of bla ACT-1 β-lactamase production, porin OmpK35/36 insertional inactivation, and down-regulation of the phosphate transport porin PhoE. Antimicrob. Agents Chemother. 2006, 50, 3396–3406. [Google Scholar] [CrossRef]
- Yu, Q.; Hu, Z.; Tian, B.; Li, Y.; Li, J.; Xu, H. Drug-resistant genes and virulence factors of carbepenem-resistant Klebsiella peumoniae. Chin. J. Clin. Infect. Dis. 2016, 6, 52–58. [Google Scholar]
- Wong, J.L.; Romano, M.; Kerry, L.E.; Kwong, H.-S.; Low, W.-W.; Brett, S.J.; Clements, A.; Beis, K.; Frankel, G. OmpK36-mediated carbapenem resistance attenuates ST258 Klebsiella pneumoniae in vivo. Nat. Commun. 2019, 10, 3957. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Jiang, X.; Wang, Y.; Li, G.; Tian, Y.; Liu, H.; Ai, F.; Ma, Y.; Wang, B.; Ruan, F.; et al. Contribution of β-Lactamases and Porin Proteins OmpK35 and OmpK36 to Carbapenem Resistance in Clinical Isolates of KPC-2-Producing Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2014, 58, 1214–1217. [Google Scholar] [CrossRef] [PubMed]
- Stuart, R.L.; Wilson, J.; Bellaard-Smith, E.; Brown, R.; Wright, L.; Vandergraaf, S.; Gillespie, E.E. Antibiotic use and misuse in residential aged care facilities. Intern. Med. J. 2012, 42, 1145–1149. [Google Scholar] [CrossRef] [PubMed]
- Raban, M.Z.; Gates, P.J.; Gasparini, C.; Westbrook, J.I. Temporal and regional trends of antibiotic use in long-term aged care facilities across 39 countries, 1985–2019: Systematic review and meta-analysis. PLoS ONE 2021, 16, e0256501. [Google Scholar] [CrossRef] [PubMed]
- Surveillance Outcome Programs Bloodstream Infections 2021 Report; Australian Group on Antimicrobial Resistance: East Perth, Australia, 2021.
- Cowan, R.U.; Kishan, D.; Walton, A.L.; Sneath, E.; Cheah, T.; Butwilowsky, J.; Friedman, N.D. Cleaning, resistant bacteria, and antibiotic prescribing in residential aged care facilities. Am. J. Infect. Control 2016, 44, e19–e21. [Google Scholar] [CrossRef] [PubMed]
- Tronsmo, A.; Gjøen, T.; Sørum, H.; Godfroid, J.; Yazdankhah, S.P.; Jelmert, A.; Klein, J.; Okoli, A.S.; Ytrehus, B.; Skaar, I. Antimicrobial Resistance due to the Use of Biocides and Heavy Metals: A Literature Review; Norwegian Scientific Committee for Food Safety: Oslo, Norway, 2016. [Google Scholar]
- Mao, Y.-C.; Chang, C.-L.; Huang, Y.-C.; Su, L.-H.; Lee, C.-T. Laboratory investigation of a suspected outbreak caused by Providencia stuartii with intermediate resistance to imipenem at a long-term care facility. J. Microbiol. Immunol. Infect. 2018, 51, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Ingarfield, S.L.; Finn, J.C.; Jacobs, I.G.; Gibson, N.P.; Holman, C.D.; Jelinek, G.A.; Flicker, L. Use of emergency departments by older people from residential care: A population based study. Age Ageing 2009, 38, 314–318. [Google Scholar] [CrossRef] [PubMed]
- O’Fallon, E.; Kandel, R.; Schreiber, R.; D’Agata, E.M. Acquisition of multidrug-resistant gram-negative bacteria: Incidence and risk factors within a long-term care population. Infect. Control Hosp. Epidemiol. 2010, 31, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- Dowson, L.; Rajkhowa, A.; Buising, K.; Kong, D.C.; Stuart, R.L.; Thursky, K.; Bennett, N. The 2018 Aged Care National Antimicrobial Prescribing Survey: Results show room for improvement. Aust. Prescr. 2019, 42, 200–203. [Google Scholar] [CrossRef]
- Stuart, R.L.; Marshall, C.; Orr, E.; Bennett, N.; Athan, E.; Friedman, D.; Reilly, M.; Racrig, M.O. Survey of infection control and antimicrobial stewardship practices in Australian residential aged-care facilities. Intern. Med. J. 2015, 45, 576–580. [Google Scholar] [CrossRef]
- Mody, L.; Foxman, B.; Bradley, S.; McNamara, S.; Lansing, B.; Gibson, K.; Cassone, M.; Armbruster, C.; Mantey, J.; Min, L. Longitudinal assessment of multidrug-resistant organisms in newly admitted nursing facility patients: Implications for an evolving population. Clin. Infect. Dis. 2018, 67, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Kahvecioglu, D.; Ramiah, K.; McMaughan, D.; Garfinkel, S.; McSorley, V.E.; Nguyen, Q.N.; Yang, M.; Pugliese, C.; Mehr, D.; Phillips, C.D. Multidrug-resistant organism infections in US nursing homes: A national study of prevalence, onset, and transmission across care settings, October 1, 2010–December 31, 2011. Infect. Control Hosp. Epidemiol. 2014, 35, S48–S55. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Carbapenem-resistant Klebsiella pneumoniae associated with a long-term-care facility—West Virginia, 2009–2011. MMWR. Morb. Mortal. Wkly. Rep. 2011, 60, 1418–1420. [Google Scholar]
- Munoz-Price, L.S.; Hayden, M.K.; Lolans, K.; Won, S.; Calvert, K.; Lin, M.; Sterner, A.; Weinstein, R.A. Successful control of an outbreak of Klebsiella pneumoniae carbapenemase—Producing K. pneumoniae at a long-term acute care hospital. Infect. Control Hosp. Epidemiol. 2010, 31, 341–347. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing (EUCAST). Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 13.0; EUCAST: Växjö, Sweden, 2023. [Google Scholar]
- Wand, M.E.; Bock, L.J.; Bonney, L.C.; Sutton, J.M. Mechanisms of Increased Resistance to Chlorhexidine and Cross-Resistance to Colistin following Exposure of Klebsiella pneumoniae Clinical Isolates to Chlorhexidine. Antimicrob. Agents Chemother. 2017, 61, e01162-16. [Google Scholar] [CrossRef] [PubMed]
- Amsalu, A.; Sapula, S.A.; De Barros Lopes, M.; Hart, B.J.; Nguyen, A.H.; Drigo, B.; Turnidge, J.; Leong, L.E.; Venter, H. Efflux Pump-Driven Antibiotic and Biocide Cross-Resistance in Pseudomonas aeruginosa Isolated from Different Ecological Niches: A Case Study in the Development of Multidrug Resistance in Environmental Hotspots. Microorganisms 2020, 8, 1647. [Google Scholar] [CrossRef] [PubMed]
- Morrissey, I.; Oggioni, M.R.; Knight, D.; Curiao, T.; Coque, T.; Kalkanci, A.; Martinez, J.L.; Consortium, B. Evaluation of epidemiological cut-off values indicates that biocide resistant subpopulations are uncommon in natural isolates of clinically-relevant microorganisms. PLoS ONE 2014, 9, e86669. [Google Scholar] [CrossRef] [PubMed]
- Sundaramoorthy, N.S.; Suresh, P.; Selva Ganesan, S.; GaneshPrasad, A.; Nagarajan, S. Restoring colistin sensitivity in colistin-resistant E. coli: Combinatorial use of MarR inhibitor with efflux pump inhibitor. Sci. Rep. 2019, 9, 19845. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.-H.; Lo, C.-C.; Chou, M.-C.; Yeh, T.-H.; Chen, K.-L.; Liao, W.-Y.; Lo, H.-R. Synergistic Actions of Benzyl Isothiocyanate with Ethylenediaminetetraacetic Acid and Efflux Pump Inhibitor Phenylalanine-Arginine β-Naphthylamide against Multidrug-Resistant Escherichia coli. Microb. Drug Resist. 2020, 26, 468–474. [Google Scholar] [CrossRef]
- Venter, H.; Mowla, R.; Ohene-Agyei, T.; Ma, S. RND-type drug efflux pumps from Gram-negative bacteria: Molecular mechanism and inhibition. Front. Microbiol. 2015, 6, 377. [Google Scholar] [CrossRef]
- Quijada, N.M.; Rodríguez-Lázaro, D.; Eiros, J.M.; Hernández, M. TORMES: An automated pipeline for whole bacterial genome analysis. Bioinformatics 2019, 35, 4207–4212. [Google Scholar] [CrossRef] [PubMed]
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A flexible trimmer for Illumina sequence data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef] [PubMed]
- Cantu, V.A.; Sadural, J.; Edwards, R. PRINSEQ++, a multi-threaded tool for fast and efficient quality control and preprocessing of sequencing datasets. PeerJ Prepr. 2019, 7, e27553v27551. [Google Scholar]
- Joshi, N.A.; Fass, J.N. Sickle: A Sliding-Window, Adaptive, Quality-Based Trimming Tool for FastQ Files (Version 1.33) [Software]. Available online: https://github.com/najoshi/sickle (accessed on 1 January 2022).
- Bankevich, A.; Nurk, S.; Antipov, D.; Gurevich, A.A.; Dvorkin, M.; Kulikov, A.S.; Lesin, V.M.; Nikolenko, S.I.; Pham, S.; Prjibelski, A.D. SPAdes: A new genome assembly algorithm and its applications to single-cell sequencing. J. Comput. Biol. 2012, 19, 455–477. [Google Scholar] [CrossRef] [PubMed]
- Seemann, T. Prokka: Rapid prokaryotic genome annotation. Bioinformatics 2014, 30, 2068–2069. [Google Scholar] [CrossRef] [PubMed]
- Bortolaia, V.; Kaas, R.S.; Ruppe, E.; Roberts, M.C.; Schwarz, S.; Cattoir, V.; Philippon, A.; Allesoe, R.L.; Rebelo, A.-R.; Florensa, A.F. ResFinder 4.0 for predictions of phenotypes from genotypes. J. Antimicrob. Chemother. 2020, 75, 3491–3500. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.K.; Padmanabhan, B.R.; Diene, S.M.; Lopez-Rojas, R.; Kempf, M.; Landraud, L.; Rolain, J.-M. ARG-ANNOT, a new bioinformatic tool to discover antibiotic resistance genes in bacterial genomes. Antimicrob. Agents Chemother. 2014, 58, 212–220. [Google Scholar] [CrossRef] [PubMed]
- McArthur, A.G.; Waglechner, N.; Nizam, F.; Yan, A.; Azad, M.A.; Baylay, A.J.; Bhullar, K.; Canova, M.J.; De Pascale, G.; Ejim, L. The comprehensive antibiotic resistance database. Antimicrob. Agents Chemother. 2013, 57, 3348–3357. [Google Scholar] [CrossRef] [PubMed]
- CSIphylogeny. Available online: https://cge.food.dtu.dk/services/CSIPhylogeny/ (accessed on 1 January 2022).
- Berglund, B.; Hoang, N.T.B.; Lundberg, L.; Le, N.K.; Tärnberg, M.; Nilsson, M.; Bornefall, E.; Khu, D.T.K.; Welander, J.; Le, H.T.; et al. Clonal spread of carbapenem-resistant Klebsiella pneumoniae among patients at admission and discharge at a Vietnamese neonatal intensive care unit. Antimicrob. Resist. Infect. Control 2021, 10, 162. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhu, S.; Wei, L.; Feng, Y.; Cai, L.; Dunn, S.; McNally, A.; Zong, Z. Arm race among closely-related carbapenem-resistant Klebsiella pneumoniae clones. ISME Commun. 2022, 2, 76. [Google Scholar] [CrossRef]
- Feng, Y.; Wei, L.; Zhu, S.; Qiao, F.; Zhang, X.; Kang, Y.; Cai, L.; Kang, M.; McNally, A.; Zong, Z. Handwashing sinks as the source of transmission of ST16 carbapenem-resistant Klebsiella pneumoniae, an international high-risk clone, in an intensive care unit. J. Hosp. Infect. 2020, 104, 492–496. [Google Scholar] [CrossRef]
- PlasmidFinder 2.1.1. Available online: https://bioweb.pasteur.fr/packages/pack@PlasmidFinder@2.1.1 (accessed on 1 January 2023).
- Letunic, I.; Bork, P. Interactive Tree Of Life (iTOL): An online tool for phylogenetic tree display and annotation. Bioinformatics 2007, 23, 127–128. [Google Scholar] [CrossRef]
- Swift, M.L. GraphPad prism, data analysis, and scientific graphing. J. Chem. Inf. Comput. Sci. 1997, 37, 411–412. [Google Scholar] [CrossRef]
- Kampf, G. Adaptive bacterial response to low level chlorhexidine exposure and its implications for hand hygiene. Microb. Cell 2019, 6, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhao, Y.; Xu, C.; Zhang, X.; Li, J.; Dong, G.; Cao, J.; Zhou, T. Chlorhexidine exposure of clinical Klebsiella pneumoniae strains leads to acquired resistance to this disinfectant and to colistin. Int. J. Antimicrob. Agents 2019, 53, 864–867. [Google Scholar] [CrossRef] [PubMed]
- Gorrie, C.L.; Mirceta, M.; Wick, R.R.; Judd, L.M.; Wyres, K.L.; Thomson, N.R.; Strugnell, R.A.; Pratt, N.F.; Garlick, J.S.; Watson, K.M.; et al. Antimicrobial-Resistant Klebsiella pneumoniae Carriage and Infection in Specialized Geriatric Care Wards Linked to Acquisition in the Referring Hospital. Clin. Infect. Dis. 2018, 67, 161–170. [Google Scholar] [CrossRef]
- Stuart, R.L.; Kotsanas, D.; Webb, B.; Vandergraaf, S.; Gillespie, E.E.; Hogg, G.G.; Korman, T.M. Prevalence of antimicrobial-resistant organisms in residential aged care facilities. Med. J. Aust. 2011, 195, 530–533. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, A.; Sonbol, F.; Elbanna, T.; El-Ekhnawy, E. Exposure to sublethal concentrations of benzalkonium chloride induces antimicrobial resistance and cellular changes in Klebsiellae pneumoniae clinical isolates. Microb. Drug Resist. 2019, 25, 631–638. [Google Scholar] [CrossRef]
- Srinivasan, V.B.; Rajamohan, G. KpnEF, a New Member of the Klebsiella pneumoniae Cell Envelope Stress Response Regulon, Is an SMR-Type Efflux Pump Involved in Broad-Spectrum Antimicrobial Resistance. Antimicrob. Agents Chemother. 2013, 57, 4449–4462. [Google Scholar] [CrossRef]
- Satlin, M.J.; Lewis, J.S.; Weinstein, M.P.; Patel, J.; Humphries, R.M.; Kahlmeter, G.; Giske, C.G.; Turnidge, J. Clinical and Laboratory Standards Institute and European Committee on Antimicrobial Susceptibility Testing Position Statements on Polymyxin B and Colistin Clinical Breakpoints. Clin. Infect. Dis. 2020, 71, e523–e529. [Google Scholar] [CrossRef]
- EUCAST. E.C.o.A.S.T. Colistin Guidance. 2022. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Guidance_documents/Colistin_guidance_2022.pdf (accessed on 11 February 2023).
- Hammond, D.S.; Schooneveldt, J.M.; Nimmo, G.R.; Huygens, F.; Giffard, P.M. blaSHV Genes in Klebsiella pneumoniae: Different Allele Distributions Are Associated with Different Promoters within Individual Isolates. Antimicrob. Agents Chemother. 2005, 49, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Drieux, L.; Brossier, F.; Sougakoff, W.; Jarlier, V. Phenotypic detection of extended-spectrum β-lactamase production in Enterobacteriaceae: Review and bench guide. Clin. Microbiol. Infect. 2008, 14, 90–103. [Google Scholar] [CrossRef] [PubMed]
- Jacoby, G.A. AmpC β-lactamases. Clin. Microbiol. Rev. 2009, 22, 161–182. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Tian, L.; Li, G.; Qu, H.; Sun, J.; Liang, W.; Li, X.; Wang, X.; Deng, Z.; Liu, J.; et al. Emergence of the third-generation cephalosporin-resistant hypervirulent Klebsiella pneumoniae due to the acquisition of a self-transferable blaDHA-1-carrying plasmid by an ST23 strain. Virulence 2018, 9, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Pishtiwan, A.H.; Khadija, K.M. Prevalence of blaTEM, blaSHV, and blaCTX-M Genes among ESBL-Producing Klebsiella pneumoniae and Escherichia coli Isolated from Thalassemia Patients in Erbil, Iraq. Mediterr J Hematol Infect Dis 2019, 11, e2019041. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, I.; Chenouf, N.S.; Carvalho, J.A.; Castro, A.P.; Silva, V.; Capita, R.; Alonso-Calleja, C.; Enes Dapkevicius, M.L.N.; Igrejas, G.; Torres, C.; et al. Multidrug-resistant Klebsiella pneumoniae harboring extended spectrum β-lactamase encoding genes isolated from human septicemias. PLoS ONE 2021, 16, e0250525. [Google Scholar] [CrossRef] [PubMed]
- Damjanova, I.; Toth, A.; Paszti, J.; Hajbel-Vékony, G.; Jakab, M.; Berta, J.; Milch, H.; Füzi, M. Expansion and countrywide dissemination of ST11, ST15 and ST147 ciprofloxacin-resistant CTX-M-15-type β-lactamase-producing Klebsiella pneumoniae epidemic clones in Hungary in 2005—The new ‘MRSAs’? J. Antimicrob. Chemother. 2008, 62, 978–985. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, A.A.; Abdelaziz, N.A.; Amin, M.A.; Aziz, R.K. Novel blaCTX-M variants and genotype-phenotype correlations among clinical isolates of extended spectrum beta lactamase-producing Escherichia coli. Sci. Rep. 2019, 9, 4224. [Google Scholar] [CrossRef] [PubMed]
- Poirel, L.; Gniadkowski, M.; Nordmann, P. Biochemical analysis of the ceftazidime-hydrolysing extended-spectrum β-lactamase CTX-M-15 and of its structurally related β-lactamase CTX-M-3. J. Antimicrob. Chemother. 2002, 50, 1031–1034. [Google Scholar] [CrossRef]
- Williamson, D.A.; Roberts, S.A.; Smith, M.; Heffernan, H.; Tiong, A.; Pope, C.; Freeman, J.T. High rates of susceptibility to ceftazidime among globally prevalent CTX-M-producing Escherichia coli: Potential clinical implications of the revised CLSI interpretive criteria. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 821–824. [Google Scholar] [CrossRef]
- Stoesser, N.; Batty, E.M.; Eyre, D.W.; Morgan, M.; Wyllie, D.H.; Del Ojo Elias, C.; Johnson, J.R.; Walker, A.S.; Peto, T.E.A.; Crook, D.W. Predicting antimicrobial susceptibilities for Escherichia coli and Klebsiella pneumoniae isolates using whole genomic sequence data. J. Antimicrob. Chemother. 2013, 68, 2234–2244. [Google Scholar] [CrossRef] [PubMed]
- White, P.A.; McIver, C.J.; Deng, Y.-M.; Rawlinson, W.D. Characterisation of two new gene cassettes, aadA5 and dfrA17. FEMS Microbiol. Lett. 2000, 182, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.W.; Lim, J.; Kim, S.; Kim, J.; Kwon, G.C.; Koo, S.H. Characterization of trimethoprim-sulfamethoxazole resistance genes and their relatedness to class 1 integron and insertion sequence common region in gram-negative bacilli. J. Microbiol. Biotechnol. 2015, 25, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Lin, Y.; Wang, Z.; Hu, N.; Liu, Q.; Zhou, W.; Li, X.; Hu, L.; Guo, J.; Huang, X. Molecular mechanisms of colistin resistance in Klebsiella pneumoniae in a tertiary care teaching hospital. Front. Cell Infect. Microbiol. 2021, 11, 678. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Chiou, J.; Zeng, Z.; Liu, L.; Chen, X.; Zeng, L.; Chan, E.W.C.; Liu, J.-H.; Chen, S. Residues Distal to the Active Site Contribute to Enhanced Catalytic Activity of Variant and Hybrid β-Lactamases Derived from CTX-M-14 and CTX-M-15. Antimicrob. Agents Chemother. 2015, 59, 5976–5983. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Martínez, L.; Pascual, A.; Hernández-Allés, S.; Alvarez-Díaz, D.; Suárez, A.I.; Tran, J.; Benedí, V.J.; Jacoby, G.A. Roles of β-lactamases and porins in activities of carbapenems and cephalosporins against Klebsiella pneumoniae. Antimicrob. Agents Chemother. 1999, 43, 1669–1673. [Google Scholar] [CrossRef] [PubMed]
- Doménech-Sánchez, A.; Martínez-Martínez, L.; Hernández-Allés, S.; del Carmen Conejo, M.; Pascual, A.; Tomás, J.M.; Albertí, S.; Benedí, V.J. Role of Klebsiella pneumoniae OmpK35 porin in antimicrobial resistance. Antimicrob. Agents Chemother. 2003, 47, 3332–3335. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Allés, S.; Albertí, S.; Álvarez, D.; Doménech-Sánchez, A.; Martínez-Martínez, L.; Gil, J.; Tomás, J.M.; Benedí, V.J. Porin expression in clinical isolates of Klebsiella pneumoniae. Microbiology 1999, 145, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Ardanuy, C.; Liñares, J.; Domínguez, M.A.; Hernández-Allés, S.; Benedí, V.J.; Martínez-Martínez, L. Outer membrane profiles of clonally related Klebsiella pneumoniae isolates from clinical samples and activities of cephalosporins and carbapenems. Antimicrob. Agents Chemother. 1998, 42, 1636–1640. [Google Scholar] [CrossRef]
- Castanheira, M.; Mendes, R.E.; Sader, H.S. Low Frequency of Ceftazidime-Avibactam Resistance among Enterobacteriaceae Isolates Carrying blaKPC Collected in U.S. Hospitals from 2012 to 2015. Antimicrob. Agents Chemother. 2017, 61, e02369-16. [Google Scholar] [CrossRef]
- Tsai, Y.-K.; Fung, C.-P.; Lin, J.-C.; Chen, J.-H.; Chang, F.-Y.; Chen, T.-L.; Siu, L.K. Klebsiella pneumoniae outer membrane porins OmpK35 and OmpK36 play roles in both antimicrobial resistance and virulence. Antimicrob. Agents Chemother. 2011, 55, 1485–1493. [Google Scholar] [CrossRef] [PubMed]
- Ni, R.T.; Onishi, M.; Mizusawa, M.; Kitagawa, R.; Kishino, T.; Matsubara, F.; Tsuchiya, T.; Kuroda, T.; Ogawa, W. The role of RND-type efflux pumps in multidrug-resistant mutants of Klebsiella pneumoniae. Sci. Rep. 2020, 10, 10876. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, W.; Onishi, M.; Ni, R.; Tsuchiya, T.; Kuroda, T. Functional study of the novel multidrug efflux pump KexD from Klebsiella pneumoniae. Gene 2012, 498, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Geraci, D.; Bonura, C.; Giuffrè, M.; Saporito, L.; Graziano, G.; Aleo, A.; Fasciana, T.; Di Bernardo, F.; Stampone, T.; Palma, D. Is the monoclonal spread of the ST258, KPC-3-producing clone being replaced in southern Italy by the dissemination of multiple clones of carbapenem-nonsusceptible, KPC-3-producing Klebsiella pneumoniae? Clin. Microbiol. Infect. 2015, 21, e15–e17. [Google Scholar] [CrossRef] [PubMed]
- Wyres, K.L.; Lam, M.M.C.; Holt, K.E. Population genomics of Klebsiella pneumoniae. Nat. Rev. Microbiol. 2020, 18, 344–359. [Google Scholar] [CrossRef] [PubMed]
- Henson, S.P.; Boinett, C.J.; Ellington, M.J.; Kagia, N.; Mwarumba, S.; Nyongesa, S.; Mturi, N.; Kariuki, S.; Scott, J.A.G.; Thomson, N.R. Molecular epidemiology of Klebsiella pneumoniae invasive infections over a decade at Kilifi County Hospital in Kenya. Int. J. Med. Microbiol. 2017, 307, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.; Phan, H.T.T.; Findlay, J.; Stoesser, N.; Pankhurst, L.; Navickaite, I.; De Maio, N.; Eyre, D.W.; Toogood, G.; Orsi, N.M.; et al. Covert dissemination of carbapenemase-producing Klebsiella pneumoniae (KPC) in a successfully controlled outbreak: Long- and short-read whole-genome sequencing demonstrate multiple genetic modes of transmission. J. Antimicrob. Chemother. 2017, 72, 3025–3034. [Google Scholar] [CrossRef] [PubMed]
- Toledano-Tableros, J.E.; Gayosso-Vázquez, C.; Jarillo-Quijada, M.D.; Fernández-Vázquez, J.L.; Morfin-Otero, R.; Rodríguez-Noriega, E.; Giono-Cerezo, S.; Gutkind, G.; Di Conza, J.; Santos-Preciado, J.I. Dissemination of bla NDM–1 Gene among Several Klebsiella pneumoniae Sequence Types in Mexico Associated with Horizontal Transfer Mediated by IncF-Like Plasmids. Front. Microbiol. 2021, 12, 611274. [Google Scholar] [CrossRef] [PubMed]
- Gorrie, C.L.; Mirčeta, M.; Wick, R.R.; Judd, L.M.; Lam, M.M.; Gomi, R.; Abbott, I.J.; Thomson, N.R.; Strugnell, R.A.; Pratt, N.F. Genomic dissection of Klebsiella pneumoniae infections in hospital patients reveals insights into an opportunistic pathogen. Nat. Commun. 2022, 13, 3017. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, X.; Torres, V.V.L.; Liu, H.; Rocker, A.; Zhang, Y.; Wang, J.; Chen, L.; Bi, W.; Lin, J. An outbreak of carbapenem-resistant and hypervirulent Klebsiella pneumoniae in an intensive care unit of a major teaching hospital in Wenzhou, China. Front. Public Health 2019, 7, 229. [Google Scholar] [CrossRef]
- Emeraud, C.; Figueiredo, S.; Bonnin, R.A.; Khecharem, M.; Ouzani, S.; Leblanc, P.-E.; Jousset, A.B.; Fortineau, N.; Duranteau, J.; Dortet, L. Outbreak of CTX-M-15 Extended-Spectrum β-Lactamase-Producing Klebsiella pneumoniae ST394 in a French Intensive Care Unit Dedicated to COVID-19. Pathogens 2021, 10, 1426. [Google Scholar] [CrossRef] [PubMed]
- Marsh, J.W.; Mustapha, M.M.; Griffith, M.P.; Evans, D.R.; Ezeonwuka, C.; Pasculle, A.W.; Shutt, K.A.; Sundermann, A.; Ayres, A.M.; Shields, R.K. Evolution of outbreak-causing carbapenem-resistant Klebsiella pneumoniae ST258 at a tertiary care hospital over 8 years. mBio 2019, 10, e01945-19. [Google Scholar] [CrossRef] [PubMed]
- Arteaga-Livias, K.; Pinzas-Acosta, K.; Perez-Abad, L.; Panduro-Correa, V.; Rabaan, A.A.; Pecho-Silva, S.; Dámaso-Mata, B. A multidrug-resistant Klebsiella pneumoniae outbreak in a Peruvian hospital: Another threat from the COVID-19 pandemic. Infect. Control Hosp. Epidemiol. 2022, 43, 267–268. [Google Scholar] [CrossRef] [PubMed]
- Rosello, A.; Hayward, A.C.; Hopkins, S.; Horner, C.; Ironmonger, D.; Hawkey, P.M.; Deeny, S.R. Impact of long-term care facility residence on the antibiotic resistance of urinary tract Escherichia coli and Klebsiella. J. Antimicrob. Chemother. 2017, 72, 1184–1192. [Google Scholar] [CrossRef] [PubMed]
- Ulstad, C.R.; Solheim, M.; Berg, S.; Lindbæk, M.; Dahle, U.R.; Wester, A.L. Carriage of ESBL/AmpC-producing or ciprofloxacin non-susceptible Escherichia coli and Klebsiella spp. in healthy people in Norway. Antimicrob. Resist. Infect. Control 2016, 5, 57. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.-P.; Wang, J.-T.; Chang, S.-C.; Chang, F.-Y.; Fung, C.-P.; Chuang, Y.-C.; Chen, Y.-S.; Shiau, Y.-R.; Tan, M.-C.; Wang, H.-Y. The antimicrobial susceptibility of Klebsiella pneumoniae from community settings in Taiwan, a trend analysis. Sci. Rep. 2016, 6, 36280. [Google Scholar] [CrossRef] [PubMed]
- Andriatahina, T.; Randrianirina, F.; Hariniana, E.R.; Talarmin, A.; Raobijaona, H.; Buisson, Y.; Richard, V. High prevalence of fecal carriage of extended-spectrum β-lactamase-producing Escherichia coli and Klebsiella pneumoniae in a pediatric unit in Madagascar. BMC Infect. Dis. 2010, 10, 204. [Google Scholar] [CrossRef]
- Sapula, S.A.; Amsalu, A.; Whittall, J.J.; Hart, B.J.; Siderius, N.L.; Nguyen, L.; Gerber, C.; Turnidge, J.; Venter, H. The scope of antimicrobial resistance in Residential Aged Care Facilities determined through analysis of Escherichia coli and the total wastewater resistome. mSpectrum, 2023; 11, e00731-23. [Google Scholar]
- Mulder, M.; Kiefte-de Jong, J.C.; Goessens, W.H.F.; de Visser, H.; Hofman, A.; Stricker, B.H.; Verbon, A. Risk factors for resistance to ciprofloxacin in community-acquired urinary tract infections due to Escherichia coli in an elderly population. J. Antimicrob. Chemother. 2016, 72, 281–289. [Google Scholar] [CrossRef]
- Tran, J.H.; Jacoby, G.A. Mechanism of plasmid-mediated quinolone resistance. Proc. Natl. Acad. Sci. USA 2002, 99, 5638–5642. [Google Scholar] [CrossRef]
- Jacoby, G.A.; Strahilevitz, J.; Hooper, D.C. Plasmid-mediated quinolone resistance. Plasmids Biol. Impact Biotechnol. Discov. 2015, 475–503. [Google Scholar] [CrossRef]
- Rodríguez-Martínez, J.M.; Cano, M.E.; Velasco, C.; Martínez-Martínez, L.; Pascual, A. Plasmid-mediated quinolone resistance: An update. J. Infect. Chemother. 2011, 17, 149–182. [Google Scholar] [CrossRef] [PubMed]
- Agyepong, N.; Govinden, U.; Owusu-Ofori, A.; Amoako, D.G.; Allam, M.; Janice, J.; Pedersen, T.; Sundsfjord, A.; Essack, S. Genomic characterization of multidrug-resistant ESBL-producing Klebsiella pneumoniae isolated from a Ghanaian teaching hospital. Int. J. Infect. Dis. 2019, 85, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Mbelle, N.M.; Feldman, C.; Sekyere, J.O.; Maningi, N.E.; Modipane, L.; Essack, S.Y. Pathogenomics and evolutionary epidemiology of multi-drug resistant clinical Klebsiella pneumoniae isolated from Pretoria, South Africa. Sci. Rep. 2020, 10, 1232. [Google Scholar] [CrossRef] [PubMed]
- Quan, J.; Li, X.; Chen, Y.; Jiang, Y.; Zhou, Z.; Zhang, H.; Sun, L.; Ruan, Z.; Feng, Y.; Akova, M. Prevalence of mcr-1 in Escherichia coli and Klebsiella pneumoniae recovered from bloodstream infections in China: A multicentre longitudinal study. Lancet Infect. Dis. 2017, 17, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, Y.; Zhou, Y.; Li, J.; Yin, W.; Wang, S.; Zhang, S.; Shen, J.; Shen, Z.; Wang, Y. Emergence of a novel mobile colistin resistance gene, mcr-8, in NDM-producing Klebsiella pneumoniae. Emerg. Microbes Infect. 2018, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-Q.; Li, Y.-X.; Lei, C.-W.; Zhang, A.-Y.; Wang, H.-N. Novel plasmid-mediated colistin resistance gene mcr-7.1 in Klebsiella pneumoniae. J. Antimicrob. Chemother. 2018, 73, 1791–1795. [Google Scholar] [CrossRef]
- Ah, Y.-M.; Kim, A.-J.; Lee, J.-Y. Colistin resistance in Klebsiella pneumoniae. Int. J. Antimicrob. Agents 2014, 44, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Elias, R.; Duarte, A.; Perdigão, J. A molecular perspective on colistin and Klebsiella pneumoniae: Mode of action, resistance genetics, and phenotypic susceptibility. Diagnostics 2021, 11, 1165. [Google Scholar] [CrossRef]
- Miro, E.; Rossen, J.W.; Chlebowicz, M.A.; Harmsen, D.; Brisse, S.; Passet, V.; Navarro, F.; Friedrich, A.W.; García-Cobos, S. Core/whole genome multilocus sequence typing and core genome SNP-based typing of OXA-48-producing Klebsiella pneumoniae clinical isolates from Spain. Front. Microbiol. 2020, 10, 2961. [Google Scholar] [CrossRef]
- Popa, L.I.; Gheorghe, I.; Barbu, I.C.; Surleac, M.; Paraschiv, S.; Măruţescu, L.; Popa, M.; Pîrcălăbioru, G.G.; Talapan, D.; Niţă, M. Multidrug resistant Klebsiella pneumoniae ST101 clone survival chain from inpatients to hospital effluent after chlorine treatment. Front. Microbiol. 2021, 11, 610296. [Google Scholar] [CrossRef]
- Pérez-Vázquez, M.; Oteo, J.; García-Cobos, S.; Aracil, B.; Harris, S.R.; Ortega, A.; Fontanals, D.; Hernández, J.M.; Solís, S.; Campos, J. Phylogeny, resistome and mobile genetic elements of emergent OXA-48 and OXA-245 Klebsiella pneumoniae clones circulating in Spain. J. Antimicrob. Chemother. 2016, 71, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Oteo, J.; Pérez-Vázquez, M.; Bautista, V.; Ortega, A.; Zamarrón, P.; Saez, D.; Fernández-Romero, S.; Lara, N.; Ramiro, R.; Aracil, B. The spread of KPC-producing Enterobacteriaceae in Spain: WGS analysis of the emerging high-risk clones of Klebsiella pneumoniae ST11/KPC-2, ST101/KPC-2 and ST512/KPC-3. J. Antimicrob. Chemother. 2016, 71, 3392–3399. [Google Scholar] [CrossRef] [PubMed]
- Kotsanas, D.; Wijesooriya, W.; Korman, T.M.; Gillespie, E.E.; Wright, L.; Snook, K.; Williams, N.; Bell, J.M.; Li, H.Y.; Stuart, R.L. “Down the drain”: Carbapenem-resistant bacteria in intensive care unit patients and handwashing sinks. Med. J. Aust. 2013, 198, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Starlander, G.; Melhus, Å. Minor outbreak of extended-spectrum β-lactamase-producing Klebsiella pneumoniae in an intensive care unit due to a contaminated sink. J. Hosp. Infect. 2012, 82, 122–124. [Google Scholar] [CrossRef]
- Decraene, V.; Phan, H.; George, R.; Wyllie, D.; Akinremi, O.; Aiken, Z.; Cleary, P.; Dodgson, A.; Pankhurst, L.; Crook, D. A large, refractory nosocomial outbreak of Klebsiella pneumoniae carbapenemase-producing Escherichia coli demonstrates carbapenemase gene outbreaks involving sink sites require novel approaches to infection control. Antimicrob. Agents Chemother. 2018, 62, e01689-18. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Accession: | Isolate: | Accession: | Isolate: |
|---|---|---|---|
| SAMN33942927 | A031 | SAMN33942935 | 2401 |
| SAMN33942928 | A026 | SAMN33942936 | 2404 |
| SAMN33942929 | A095 | SAMN33942937 | 2410 |
| SAMN33942930 | A529 | SAMN33942938 | 2418 |
| SAMN33942931 | A629 | SAMN33942939 | A922 |
| SAMN33942932 | A413 | SAMN33942940 | 2362 |
| SAMN33942933 | A409 |
| Sample Type | |||||
|---|---|---|---|---|---|
| K. pneumoniae Complex Isolates n (%) | Faecal n (%) | Urine n (%) | Facility Swab n (%) | Wastewater n (%) | |
| Facility 1 | 97 (66) | 46 (47) | 0 (0) | 4 (4) | 47 (48) |
| Facility 2 | 25 (17) | 16 (64) | 0 (0) | 0 (0) | 9 (36) |
| Facility 3 | 7 (5) | 5 (71) | 2 (29) | 0 (0) | 0 (0) |
| Retirement | 18 (12) | 15 (83) | 0 (0) | 0 (0) | 3 (17) |
| Total: | 147 (100) | 82 (56) | 2 (1) | 4 (2) | 59 (40) |
| MIC (mg/L) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial | <0.125 | 0.125 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | 16 | 32 | 64 | >64 | % Resistant |
| Ceftazidime | 3 | 1 | 5 | 19 | 23 | 18 | 11 | 4 | 0 | 4 | 2 | 57 | 46 |
| Cefepime | 32 | 3 | 12 | 33 | 21 | 15 | 8 | 3 | 1 | 3 | 1 | 15 | 16 |
| Ciprofloxacin | 13 | 5 | 8 | 19 | 9 | 17 | 26 | 24 | 7 | 4 | 7 | 8 | 69 |
| Tobramycin | 0 | 0 | 6 | 43 | 62 | 21 | 3 | 1 | 3 | 4 | 3 | 1 | 10 |
| Amikacin | 0 | 0 | 3 | 4 | 15 | 72 | 36 | 9 | 6 | 1 | 0 | 1 | 5 |
| Meropenem | 31 | 0 | 6 | 13 | 35 | 46 | 14 | 2 | 0 | 0 | 0 | 0 | 0 |
| Colistin | 0 | 0 | 3 | 11 | 41 | 90 | 1 | 0 | 0 | 1 | 0 | 0 | 1 |
| <0.125 | 0.125 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | >8 | |||||
| Trimethoprim sulfamethoxazole | 2 | 8 | 16 | 14 | 13 | 16 | 9 | 7 | 62 | 47 | |||
| MIC (mg/L) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antimicrobial | ≤0.125 | 0.125 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | 16 | 32 | 64 | >64 | % Tolerant | |
| Biocide | CHG | 2 | 0 | 1 | 0 | 5 | 8 | 33 | 41 | 32 | 21 | 2 | 2 | 1 |
| TRI | 5 | 1 | 7 | 14 | 20 | 33 | 27 | 26 | 5 | 0 | 1 | 8 | 46 | |
| BZK | 0 | 0 | 0 | 0 | 4 | 2 | 0 | 1 | 21 | 88 | 27 | 4 | 21 | |
| MIC (mg/L) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CTZ | FEP | CIP | TOB | AMI | MER | COL | SXT | |||
| EUCAST Breakpoint | >4 | >4 | >0.5 | >2 | >8 | >8 | >2 | >4 | ||
| Isolate | ST | Source | ||||||||
| A031 | 4726 | Faecal | 2 | 0.125 | 0.25 | 0.25 | 0.25 | <0.125 | 1 | 4 |
| A922 | 661 | Wastewater | 32 | 8 | 2 | 1 | 1 | 1 | 2 | >8 |
| A026 | 323 | Faecal | 64 | 1 | 2 | 1 | 1 | 4 | 2 | >8 |
| A095 | 661 | Faecal | >64 | 32 | 4 | 2 | 2 | 1 | 2 | >8 |
| A409 | 323 | Facility | >64 | 1 | 2 | 0.25 | 0.25 | 2 | 1 | >8 |
| A413 | 323 | Facility | 64 | 1 | 4 | 1 | 1 | 2 | 2 | >8 |
| A529 | 661 | Facility | 32 | 0.5 | 1 | 1 | 1 | 1 | 2 | >8 |
| A629 | 323 | Faecal | 64 | 1 | 4 | 0.5 | 0.5 | 1 | 2 | >8 |
| 2362 | 323 | Wastewater | >64 | 0.5 | 4 | 0.5 | 0.5 | 2 | 2 | >8 |
| 2401 | 323 | Faecal | 64 | 1 | 4 | 0.5 | 0.5 | 2 | 2 | >8 |
| 2404 | 323 | Faecal | 64 | 1 | 4 | 1 | 1 | 4 | 2 | >8 |
| 2410 | 661 | Faecal | >64 | 64 | 8 | 0.25 | 0.25 | <0.125 | 32 | >8 |
| 2418 | 661 | Faecal | >64 | 64 | 8 | 1 | 1 | 1 | 2 | >8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blaikie, J.M.; Sapula, S.A.; Siderius, N.L.; Hart, B.J.; Amsalu, A.; Leong, L.E.X.; Warner, M.S.; Venter, H. Resistome Analysis of Klebsiella pneumoniae Complex from Residential Aged Care Facilities Demonstrates Intra-facility Clonal Spread of Multidrug-Resistant Isolates. Microorganisms 2024, 12, 751. https://doi.org/10.3390/microorganisms12040751
Blaikie JM, Sapula SA, Siderius NL, Hart BJ, Amsalu A, Leong LEX, Warner MS, Venter H. Resistome Analysis of Klebsiella pneumoniae Complex from Residential Aged Care Facilities Demonstrates Intra-facility Clonal Spread of Multidrug-Resistant Isolates. Microorganisms. 2024; 12(4):751. https://doi.org/10.3390/microorganisms12040751
Chicago/Turabian StyleBlaikie, Jack M., Sylvia A. Sapula, Naomi L. Siderius, Bradley J. Hart, Anteneh Amsalu, Lex E.X. Leong, Morgyn S. Warner, and Henrietta Venter. 2024. "Resistome Analysis of Klebsiella pneumoniae Complex from Residential Aged Care Facilities Demonstrates Intra-facility Clonal Spread of Multidrug-Resistant Isolates" Microorganisms 12, no. 4: 751. https://doi.org/10.3390/microorganisms12040751
APA StyleBlaikie, J. M., Sapula, S. A., Siderius, N. L., Hart, B. J., Amsalu, A., Leong, L. E. X., Warner, M. S., & Venter, H. (2024). Resistome Analysis of Klebsiella pneumoniae Complex from Residential Aged Care Facilities Demonstrates Intra-facility Clonal Spread of Multidrug-Resistant Isolates. Microorganisms, 12(4), 751. https://doi.org/10.3390/microorganisms12040751