Abstract
Background: This is the first ethnobotanical study focused on medicinal plants traditionally recommended by traditional healers (THs) of Eastern Morocco. In this work, we documented the medicinal plants recommended by THs and highlighted the value and importance of medicinal plants recommended by specialist healers. Methods: A quali-quantitative ethnobotanical method has been performed, snowball sampling and structured interviews were used to evaluate the traditional plant knowledge by traditional healers in the study area. Species identification was performed and verified from the African Plant Database and Plant List. Two Relative Cultural Importance indices were used for this analysis “Informant Consensus Factor (ICF) and Frequency of Citation (FC)”. Results: A total of 135 plants were inventoried in our surveys. These species belong to 64 families and were reported to be used to treat 23 different categories of ailments. The botanical profile of the plants listed is dominated by LAMIACEAE’s Family with 12 species, followed by FABACEAE (11 species) and ASTERACEAE (10 species). In the category of the digestive system, nutrition problems and nervous system problems seem to be the predominant diseases treated. The Informant Consensus Factor (ICF) results indicated that cancer and gastrointestinal disorders had a higher concordance among informants (ICF = 0.60 and 0.58 respectively). Conclusion: Our results, showed that the Traditional healers, in Eastern Morocco, hold impressive knowledge related to the use of medicinal plants. This observation is reflected in the high number of medicinal plants recommended for the medication of the population. Furthermore, the consistency of healers in this area of study is justified by the ICF values.
1. Introduction
It is impossible to embark upon the subject of medical tradition in Morocco without first briefly recalling the main Arab medical thought and “know-how” of Muslim communities regarding traditional medicine [1].
Belonging to the Arab world, Moroccan people have a long habit of the use of traditional medicinal and aromatic plants for medical purposes. Since time immemorial, Moroccan people have gathered plant and animal resources for their needs. Historically, Moroccan society had a wealthy pharmacopeia that dates back to 711 AD (92nd year of the Hegira). Islamic influence began in Morocco in the seventh century A.D. Arab conquerors converted the indigenous Berber population to Islam which was marked by the expansion of Moslem influence during the golden age of Arab Science “750–1258 C.E”. The Moroccan pharmacopeia was further developed and enriched by other knowledge brought in by various ethnic groups that migrated to Morocco from many areas, including the Arabs from the Middle East, the Andalusians, Jews from Europe, and the Blacks from Sudan, Senegal, and Niger. According to several distinguished authors such as Ibn El-Baithar (1877–1883) [1], who synthesized all medicinal drugs used by the Arabs up to the 13th century. Different works of literature confirm the progression of the knowledge of the Arab civilization through North Africa and the South of Spain [1,2].
So, Moroccan folk medicine is composite and complex. It is based on Arab-Islamic medicine but also hosts the elements of Greek medicine, Indian, Chinese, European, and black Africa since Morocco has been a major stopover and the crossroads of goods and cultures in Southern Europe, the Middle East, Central Asia, and Black Africa. Currently, in Morocco, several medical systems co-exist and give rise to a plural offer of therapeutic resources. Moroccan folk medicine in Morocco is a multidisciplinary and multispectral field.
According to Bellakhdar J. [3] and Claisse R. [4], Moroccan traditional healers are classed into three groups
- -
- The fuqaha (singular: fqîh), tolba (singular: tâleb) or tobba (singular: tabîb), and the healers of all kinds (kuwway or cautery installer, hajjam or barber phlebotomist, jabbar or bonestter, mul ssnan or tooth puller, qabla or traditional birth attendant…)
- -
- The apothecaries who divide themselves into two very distinct guilds ‘aṭṭârin (singular: ‘aṭṭâr) and the ‘aššabin (singular: ‘aššab). ‘aṭṭârin represents what could be called the apothecary grocers, traders of spices, aromatics, and medicinal drugs expensive and imported from distant lands. The ‘aššabin are the herbalists proper or merchants of medicinal and aromatic plants whose range, more diverse, has a large number of medicinal and magical drugs (roots, dried plants, seeds, bark, minerals, animal products) or confections, crammed together with various ingredients used in magic.
Our objectives in this work are to assist in the assessment of indigenous plant knowledge among traditional healers in Eastern Morocco. From this perspective, we performed ethnobotanical fieldwork. We have interviewed the traditional healers (THs) of any category who have fixed premises, in the region of Eastern Morocco.
2. Results and Discussions
2.1. Demographic Information of the THs and Professional Activity
2.1.1. Demographic Information of all Respondents
A total of 30 interviews were conducted in eight markets of Eastern Morocco. All of these interviews were with individuals with THs in their work premises, while more than 15 people declined to answer our questionnaires. Table 1 presents the demographic information of all respondents. All respondents are men, and only one woman was surveyed. All people who sell herbal remedies in the market are male. All the women I met in the market who were active in the field of plants were street vendors. Men dominate the practice of traditional medicine in the region. Most of the respondents (80%) were born in the region of Eastern Morocco. 80% belonged to one of the many ethnic groups of Eastern Morocco. 53% of the respondents have never lived outside the region. 67% own no land in the area. 83.33% speak more than one language and even 20% speak more than four languages (Arabic, French, English, Tamazight, Spanish). Concerning their levels of education, the results obtained show that 40% of surveyed individuals had a primary school education and 30% had a secondary school education, this is a high level of education in Morocco/the region and this high percentage reflects the average level of schooling of the population of the region. Only 3.33% were found to be illiterate. This low rate of illiteracy can be an advantage to the development of the practice of the profession. The most striking result remains that 16.67% of the people surveyed had (obtained) a university-level of education). The high number of higher-level practitioners will undoubtedly change this area, in particular because they know to avoid the complications related to the toxicity of certain medicinal plants and the possible negative side effects [5]. Finally, 6.67% of these respondents fuqaha (singular: fqih). Most are integrated and have even been known locally (33%), regionally (23%), and nationally (6.66%) (Table 1).

Table 1.
Demographic information of all traditional healers (THs).
2.1.2. Description of the Professional Activity
In this region, the majority of THs are multi-purpose herbalists (80%) (Table 2), the specialized herbalists come in next with a percentage of 13.3%. 80% of the people practice only this occupation, while 13.3% have other professions. Only four THs have a diploma related to medicinal plants or the specialties they practice (13.3%). Only 33.17% use reference books (6.67% Arabic references) that concern the use of medicinal plants. Only 20% go to patients’ houses, and they set prices before treatment with a percentage of 70% in fees with 73%. All THs have the same scales. All THs have at least four years of experience in this field. 40% of THs have been practicing this profession for more than 14 years. 93.3% have no relationship with scientific institutions. 70% of THs report that the field is unorganized and the profession is not regulated (Table 2).
Table 2.
Description of the professional activity of traditional healers (THs).
2.1.3. The Nature of the Products Sold by the THs
The products sold in herbalism are plants (67%), minerals (26.7%), animal parts (36.7), magic indices (3.33%), and herbal products (33.3%). Almost all THs that practice magic with their herbalism have refused to investigate with us. Most THs do not prepare the herbal products they sell in their practice. In fact, only 10% prepare their own products. The plants used and sold by the interviewed THs are purchased from wholesalers or collectors with a percentage of 70% (Table 2).
2.1.4. Diagnosis of Diseases
The THs report that the biggest problem in traditional medicine is diagnosis. That is why 40% of THs provide their traditional/herbal treatment after their patient has first been diagnosed with western medicine. Diagnosis by THs is done by interrogation 43% of the time and by body examination with 10% of the time based on the appearance and the complexion of the patient or the notion of hot and cold. In the cases where the symptoms are a manifestation of supernatural forces, the diagnosis is made by specialized healers (fûqha) who rely on the Quran or magic. Then only 30% of the THs do not make a diagnosis (Table 2).
2.1.5. Use of Traditional Medicine
83% of THs used medicinal plants, while only 60% used Western Medicine. 70% prefer to take care of plants because they are natural and have no side effects (Table 2).
2.1.6. Conservation and Transmission of Knowledge
60% of THs did not acquire their knowledge by transmission from father to son. 33.33% acquired this knowledge through personal experience. 76.67% do not have anyone to replace them. The remaining 33.33% have already trained people in herbalism. In most cases, training is done by observation and orally during the process of treating or selling plants (Table 2). Knowledge about the use of medicinal plants and their preparation procedures is generally passed down from generation to generation. However, this form of transmission is not always assured, putting this knowledge in danger of being lost [6]. The inventory of this knowledge is extremely valuable because it is likely to disappear with the disappearance of this kind of lifestyle and means of communication [7] (Table 2).
2.2. Medicinal Plants of Eeastern Morocco, Use, Knowledge and Importance by THs
2.2.1. Cultural Wealth
In total, 750 medicinal uses for plants were collected. After these reports were cleaned up to eliminate no plant treatments, generic plant names, and no medicinal uses, 722 responses remained. These responses were analyzed to identify medicinal plants and determine the importance of each species. The synthesis of the survey data led to an exhaustive inventory of the medicinal plants known and sold by THs to the population of Eastern Morocco (Table 3). In alphabetical order, we list the plants, their vernacular and scientific identities, their method of preparation, the form, mode, and dosage for administering remedies, the therapeutic virtues, the duration of preparation, the added ingredients, the toxicity, and the specimen. In addition to the data obtained from the survey, we present other information obtained from the literature: vernacular names used and medicinal uses in other regions of Morocco, toxicity, biological type, flowering period, ecology, bioclimate, endemism, and geographical distribution (Table A1).
Table 3.
Medicinal plants of Eeastern Morocco by THs, use, part used, preparation, route of administration, categories of diseases, toxicity, other data and the importance for each species according to the FC (frequency of citation).
To simplify the analysis, each plant response is considered a single treatment. Analytical measures of ethnobotany were then implemented to assess which species are the most important. The importance of the plants was reported according to the frequency cited (FC).
After taxonomic identification, we were able to document a total of 135 ethnomedicinal species, belonging to 125 genera and 64 families administered in about 722 herbal preparations for the treatment of 23 disease categories. LAMIACEAE was the leading family with 12 species, followed by FABACEAE (11 species), ASTERACEAE (10 species), APIACEAE (9 species), ZINGIBERACEAE (6 species), SOLANACEAE, ROSACEAE (5 species each) and the remaining ones were represented by less than four species (Table 3 and Figure 1). Our findings regarding the predominance utilization of family LAMIACEAE, FABACEAE, ASTERACEAE, and APIACEAE in Eastern Morocco were in agreement with other regions of Morocco and constitute the main groups of medicinal flora in most other Mediterranean countries [7,8,9,10].
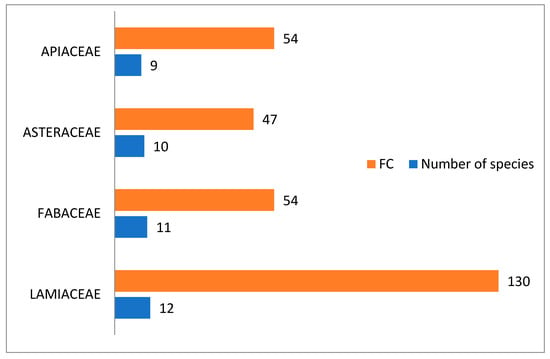
Figure 1.
Most important families by frequency of citation and number of species.
2.2.2. Description of the Species
The inventoried medicinal species fall into three categories: 55.80% are spontaneous species, 28.50% are cultivated species, and 16.20% are imported plants (Table A1). This is consistent with the results found by El-Hilaly in Taounate which states that 61% of the inventoried plants are wild species, grown with 37% and cultivated as well as spontaneous with 1.9% [11]. In addition, not native species (21 plants or 16.20%) are less important than native species (112 plants or 84.32%). This data is consistent with the findings in 2006 by a study by the US Agency for International Development on MPA at the national level. These findings may explain the observed overexploitation of these plants by the local population who use them not only to heal, but also as a source of income by marketing them. Based on the work of Oualidi J., et al. in 2012, we ranked the plants according to their chorology. 29 of the plants inventoried or 21.64% are endemic species of North Africa and 14 (10.44%) are endemic species of Morocco, while the others have a different and vast chorology [12].
The result of life form analysis showed that therophytes (TH: annual, biennal or perennial herbaceous) constituted the highest proportion (17 species or 23.6%) of the identified species, followed by chamephytes (CH: shrubs) (16 species or 22.3%), phanerophytes (PH: trees and shrubs) (14 species or 19.5%), neophanerophytes (nPH) (10 species or 13.9%) and hemicryptophytes (annual, biennal or perennial herbaceous) (8 species or 11.2%). This finding is consistent with other studies [13] (Table A1). Generally, 44.7% of the medicinal species recorded in eastern Morocco (59 plants) flower during the spring, (46 plants) or 34.8% flower in summer, followed by 12.1% (16 plants) in winter and 6.8% (9 plants) in autumn. As for bioclimatic types, the listed plants belong to six bioclimatic: saharan, semi-arid, arid, humid, sub-humid, and high mountains. However, we note a dominance of medicinal species belonging to semi-arid bioclimates coming in at 38.2% (84 plants) (Semi-Arid mild: 53 plants or 24.1%, semi-arid cold: 28 plants or 12.7% and semi-arid: 3 plants or 1.4%), (53 plants) or 24.1% belong to sub-humid bioclimates followed by (36 plants) or 16.4% in arid bioclimates, (13 plants) or 5.9% in saharan and in the end the wet, mountainous bioclimates with 1.4% (3 species). For geographical distribution, the plants’ natural habitats can be divided into three clearly delineated regions: the first significant group occupies the Rif regions, Middle Atlantic Morocco, North Atlantic Morocco, and the High Atlas Mountains at the rate of 12.1% (34 plants), 11% (31 plants), 11% (31 plants), 10.6% (30 plants) respectively; followed by the second group occupying the Middle Atlas regions, Mediterranean Coast, Eastern Morocco Mountains, Anti Atlas Mountains, Eastern Morocco Plateau, Saharan Morocco, Saharan Atlas Mountains with the lower percentages of 9.6%; 9.2%; 7.4%; 7.4%; 5.0%; 4.3%; 4.3%, respectively, and the third group, 8.50% of the total, contains the species occupying all of Morocco with some exceptions (Table A1 and Figure 2).
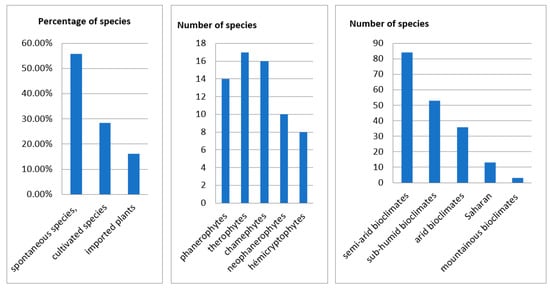
Figure 2.
Description of the species.
2.3. The Vernacular Names
Although the official language of Morocco is Arabic, various other languages like tamaziġt and šalha with various local dialects are spoken by a large number of indigenous communities of Eastern Morocco. As a result, there is a wide variety of vernacular names for (these) plants at the local level. A species with one vernacular name has different names from language to language or dialect to dialect. For example, the plant Allium sativum is called tûm in Arabic and tišart or taskart in tamazight. In addition, the vernacular name of the plant can indicate the whole plant, the part used (ssadra for the whole plant or nbaġ for the fruit which indicates Ziziphus lotus, their botanical characteristics (botanical indicates the black seeds for Nigella sativa), and their physiological effects (ḵayyâṭa indicates heals wounds for Telephium imperati).
The data show that only 84 species belonging to 45 families have a single vernacular name not shared with other species. Among these species, echoing the findings from the ethnobotanical studies conducted since 1991, there are 12 species with a single vernacular name in all the regions of Morocco and 62 species that have more than one name in the other regions of Morocco. Six species have a single name in the other regions of Morocco but more than one name in Eastern Morocco. The other species have more than one name in the region of Eastern Morocco and in winter the other regions (Table 3). These results coincide with other ethnobotanical studies carried out in Morocco [14,15,16,17,18,19].
2.4. Toxicity
60% of THs do not leave anyone in their herbalism because they know the danger of plants and their products for humans if they are sold without their control (Table 3). In case of absence (16.16%) leave confident people in relation to the field such as their parents or grandparents (grandmothers), employees, and trainees. The pharmacological analysis of the plants identified, allowed us to identify the toxic plants used in traditional pharmacopoeia in the area based on the survey and using different works, known in the scientific literature, namely “The Moroccan Traditional Pharmacopoeia, ancient Arabic medicine and popular knowledge” [3] “Toxicology in Morocco” [20], and “Toxic Plants—plants dangerous to humans and animals” [21]. The results obtained show that (59 plants) 43.7% of the plants used can cause poisoning (Table 3 and Table A1). 31% (43 plants) of plants are reported in the literature as toxic species. 27.9% of plants (12 plants) that are reported to be toxic based on the literature are also reported as toxic medicinal plants by THs. THs inventoried 16 toxic plants in addition to the species reported in the literature. The tradipraticians and the population in Morocco, have fairly important knowledge of the toxicity of medicinal plants [22]. This is contradictory to the work of Benlamdini which shows that the majority of users of traditional medicine are unaware of the toxicity of these plants [23].
2.5. Characteristics of Inventoried Recipes
2.5.1. Parts of the Plants Used
The aerial part (including leaves (34.49%), seeds (30.39%), flowers (14.78%), bark (5.95%), fruits (4.92%), boughs (3.90%) and the resin (0.41%)) is the most used part with 94.98%. Ethnobotanical studies conducted by [8,24,25,26,27,28], also show that the aerial part, especially the leaves, is the part mainly used in the various therapeutic preparations. In the context of conservation, the use of leaves in herbal preparations implies a more sustainable practice. Poffenberger’s studies have shown that removing 50% of the leaves from a tree does not significantly affect its survival [29]. Nevertheless, the collection of these organs is anarchic by local users who tend to pull the whole plant instead of focusing only on the desired part. Therefore this practice can contribute to deforestation and the degradation of ecosystems and natural resources [23]. The high frequency of use of the aerial part, especially leaves, flowers, and leafy branches, can be explained by the ease and speed of the harvest [30] and the fact that they are the site of photosynthesis and sometimes the storage of secondary metabolites responsible for the biological properties of the plant [31]. These organs provide the majority of alkaloids, glycosides, and essential oils [32]. The harvest of the underground part of the plant removes the possibility of the plant obtaining nutrients, which affects its vegetative aspect as well as its physiology [33]. However, while we see a low usage of this part (including the roots, rhizomes, and bulbs) at a percentage rate of 5.02%, it does not entail a risk of the plant’s disappearance. Figure 3 shows the rate of use of all reported plant parts.
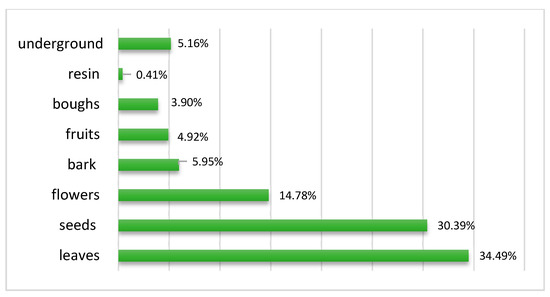
Figure 3.
Parts of the plants used.
2.5.2. Recipe Preparation Techniques
Some plants in their natural form are not suitable to be used directly as a drug and should be subjected to processes like pretreatment, detoxification, and formulation prior to administration. The processing methods include cleaning, cutting, stir-frying, charring, steaming, boiling, burning, etc. The aims of processing are to enhance the efficacy and/or reduce the toxicity and to change the effects or properties of crude drugs [34]. According to the survey, the powder is the most popular preparation method for the plants studied. It represents 42.18%. This result is corroborated by the works of Ghourri M. with a percentage rate of 84.73% [25,35], El Yahyaoui O. with a percentage of 36% [27], and Messaoudi M. with 57% [36]. However, decoction (26.17%) and infusion (21.84%) are modes used just as frequently. These results are different from the work of [23,24,37,38], who reported that decoctions is most commonly used at a rate of 47%, 37.6%; 26.80%; 40.55% respectively. Other preparation techniques (including burning, cooking with food, in the form of oil, direct, maceration, vinegar, juice, and salad) are used less often at a rate of 9.79%. According to Salhi, a decoction can collect the most active ingredients and attenuate or cancel the toxic effect of certain recipes [24]. Benlamdini N. said that decoction warms the body and disinfects the plant to cancel the toxic effect of some recipes, but it can destroy some active ingredients of the species used [23]. After processing, the chemical components of the crude drugs may change dramatically [39]. In addition, medicinal plants have side effects when they are incorrectly ingested by patients. As a result, alternative medicine must be practiced with care and within specific parameters and measurements (Figure 4).
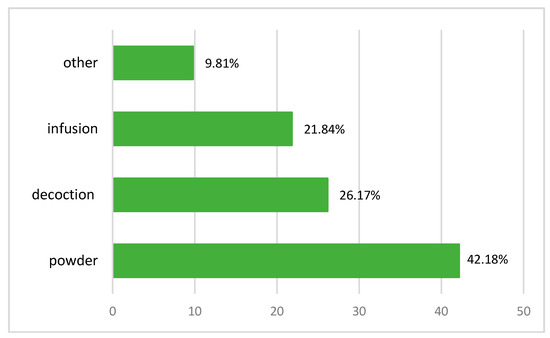
Figure 4.
Recipe preparation techniques.
2.5.3. Routes for Administering Remedies
The most frequently used mode of remedy administration is oral ingestion (82.96%). Today, most of the medicines are given orally which is in agreement with some other studies: El Rhaffari L. et al. with 57% [8] and Ouhaddou H. et al., with 64.5% [40]. Nevertheless, several works reveal other important routes. The external route (including several ways of administration: local application, bath, washing) represents 13.7% (Figure 5).
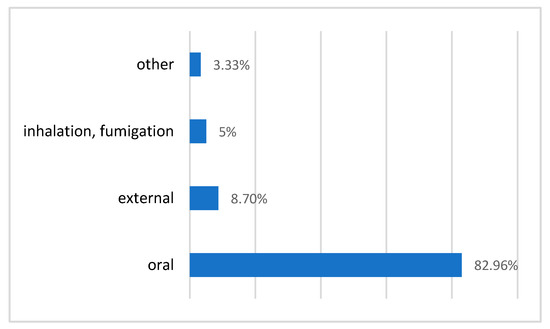
Figure 5.
Routes for administering remedies.
2.5.4. Association with Other Plants and/or Ingredients
The remedies used by THs generally contain compounds of plants, animals and minerals (Table 3). Compound remedies plants, animals, minerals) are prescribed at a rate of 35.87%, while simple recipes are at a rate of 64.12%. Of the 135 species recorded, 42 are used in simple remedies and 93 in compound remedies or in both compound and simple recipes.
The predominance of monospecific remedies is confirmed by El-Rhaffari L. et al. in 2002 [8].
Among the 259 combined remedies, 150 remedies or 20.78% contain ingredients of an animal nature (honey, milk, camel fat, chicken), 8.17%, or 59 remedies contain vegetable ingredients (plants, plant pollen, plant juices, and extraction of plants by water and vinegar), 5.68% or 41 remedies contain mixtures of plants known to traditional Moroccan medicine as râṣl-ḥanût (Mixture of Plants (Heat Therapy and Spices)), ḥarîra (soup),ḵala (Mixture of ground plants used as poultice in the case of headaches) [3] or simply meals or beverages, meat as djâj baldi: Free-range chickens (called djâj baldi in Morocco)and finally to facilitate management, 1.25% or nine remedies are ingested with water (Table 3).
This preponderance of monospecific remedies benefits patients. Indeed, combinations of plants badly matched are sometimes dangerous. In Africa, bad mixtures cause about 30% of fatal accidents [41] because synergistic action frequently results from bad combinations of medicinal plants as reported by Fleurentin and Pelt [42]. We retain here that simple remedies are the most used which can be explained by the search for simplicity in the preparation of the remedy. When recipes are compound, they contain in large part ingredients animal in origin, especially honey and milk. In addition, the use of more than one plant species to prepare a cure for diseases is attributed to the additive or synergistic effects they may have [43]. The ingredients originating from animals are identified as honey, milk, and pieces of animal organs, and according to Ouhaddou H. et al., In 2015 [40], they are added to improve the acceptability and the medicinal properties of the remedies. They are usually taken orally (Table 4).
Table 4.
Description of the remedies.
2.5.5. The Duration of the Preparation
THs reported preparation took the form of decoction and infusion at a rate of 49%. The duration of these forms of preparation does not exceed 20 min for all THs. On the other hand, the duration for maceration can reach from 3 h to several days for the population of Eastern Morocco according to the work realized by Fakchich J. and Elachouri M. in 2014 [44]. According to this study, the duration required for preparing the remedy depends on the type of preparation necessary (infusion, decoction, maceration, requires extraction with solvents), and also the parts of the plants used (leaves, stem, root, bark, rhizome). The results show that a decoction of roots or bark takes longer than one of leaves or flowers. The maceration of the seeds requires a longer time than the infusion of leaves or flowers. It is also noted that resins can be used directly. The majority of THs recommend using the plant twice a day, once in the morning and once at night, but they are not able to agree on the duration of the treatment. They all feel that they must examine the patient before making a diagnostic decision [36].
2.6. Diseases and Treatments
2.6.1. The Most Common Ailments
Results from the analysis of ethnobotany data show that registered medicinal plants are involved in the treatment of 23 disease categories. Digestive system problems are treated at a rate of 18.28% (131 citations) followed by nutrition problems at 9.41% (68 citations), problems of the reproductive system at 8.01% (58 citations), system nervous problems at 7.75% (56 citations) and skin problems at 7.06% (51 citations). Similar results are observed in an ethnobotanical study examining the population of the same region [44]. This same survey revealed that the majority of medicinal species are used mainly against diseases of the digestive system, at a rate of 50%, follow diseases of the skin (15%), the circulatory system (13%), the respiratory system (10%), and the reproductive system (5%). The remaining diseases (ophtalmic, bone, urinary, laryngological, and nervous system) represent less than 7% [44]. These values reflect the health profile of Eastern Morocco which is strongly dominated by diseases of the digestive system and dermatological pathologies. Therefore, it is interesting that labs look into the eradication of these pathologies to improve the well-being of these populations.
2.6.2. Diversity of Plants Used in the Treatment of diseases
The most frequently reported diseases also use the largest variety of plants. Gastrointestinal problem uses 56 species followed by nutrition problems (43 species), problems of the reproductive system (35 species), problems of the nervous system and dermatological problems (28 species).
2.7. Informant Consensus Factor
The results of the Informant Consensus Factor Calculator (ICF) (Table 5 and Figure 6) show that the value in our study ranges from 0.07 to 0.60. Cancer has a high ICF value of 0.60 with 21 reported uses of nine distinct species. It is followed by gastrointestinal disorders with an ICF value of 0.58, and pathologies of the nervous system ICF: 0.51. The lowest agreement between informants was observed when discussing the plants used to treat cholesterol, IFC: 0.07, poisoning problems ICF: 0.14, and ophthalmic diseases ICF: 0.17. The low ICF values observed in our study could result from a lack of communication between traditional healers in different regions of the area studied or from a lack of knowledge of problems that only slightly affect the population. These results strongly agree with data found by Fakchich J. and Elachouri in 2014 [44] in a survey of the population from the same region.
Table 5.
Category of diseases, symptom, ICF, NUR (number of use citations in each ailment), NT (number of species used for this ailment).
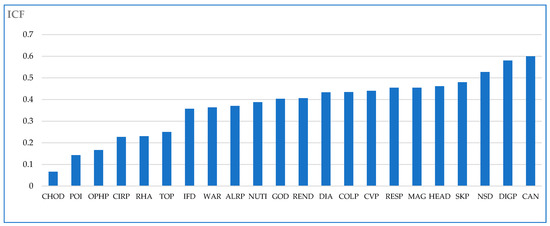
Figure 6.
Informant Consensus Factor (ICF) in Eeastern Morocco by traditional healers.
2.8. The Most Important Species According to FC
Species most commonly cited (hight FC) by THs for treatments are listed in descending order: Origanum compactum Benth (26 citations), Matricaria chamomilla L. (25 citations), Salvia officinalis L. (21 citations), Peganum harmala L. (20 citations), Lavandula dentata L. (17 citations), Berberis hispanica Boiss. & Reut. (17 citations), Rosmarinus officinalis L. (16 citations) (Table 3).
These plants are used excessively which poses a threat to long-term existence especially to those that are rare and endemic. In addition, all these species are commonly reported in the literature as being the most important medicinal plants and the most used species by people in different regions of Morocco. Thus, conserving these species in their habitats and protecting the public from their toxicity, must be central to the decision makers interest.
These plants are widely used in the literature and are even well-studied in laboratories (Table 3). Taking the following examples:
The folk species of Origanum compactum Benth., has the most cultural significance according to the FC. O. compactum Benth., is an endemic plant of Morocco, aromatic, used for cooking, and occupies the first order according to FC. It contains a toxic essence and at high dose, it causes gastric bleeding, albuminuria, and steatosis of the liver [20].
It is reported to treat 12 diseases by THs in the region of Eastern Morocco: gastrointestinal problems, cold problems, kidney disease, reproductive system problems, warming, nutritional problems, high cholesterol, circulation problems, dermatological problems, diabetes, intoxication, pathology of the respiratory system, nervous system problems and to various categories of diseases in other regions of Morocco: nutrition problems [26], allergies [44,45], circulation [40], dermal problems [26,46], diabetes [25,47,48], gastrointestinal problems [40,44,49], cold problems [10,38,46], infections [17], urinary problems [40,46,50], dental problems [38], 2011, problems with reproduction [51], respiratory problems [28,38,40,52], rheumatism, and bones problems [28,40,46,53].
Matricaria chamomilla L. is the second most culturally significant species according to the frequency cited. It is reported to treat nine diseases. It grows on farmland and uncultivated land as well as in fields, and gardens. It is widely used in Morocco to treat various categories of diseases: nutritional problems [36,54], allergies [26]; cardiac problems [55,56], dermatological problems [36,46,57], diabetes [47,49,58], gastrointestinal problems [36,46], colds [44], hypertension [56], infection [26], dental problems [59], pathologies of the renal system [55], pathologies of the reproductive system [10,54,55]; respiratory problems [10,38,60]; rheumatism and bone problems [10,54,60], nervous system problems [36,38,46], spasmodic [36,38,57], head diseases [59,61].
Peganum harmala L. occupies the fourth according to FC. It is used for 11 diseases in Eastern Morocco according to THs. It grows in the steppes, uncultivated fields, rubble, plains, and low mountains. The plant is reported to be toxic by THs but is not toxic at low doses [20]. Among the 12 THs that inventoried it as a medicinal plant, only two remedies are administered orally, which reassures us about its toxicity. It is widely used in different regions of Morocco to treat various diseases: nutrition problems [8,36], cancer [38,62,63], heart problems [8,56], circulation problems [8,64]; dental problems [8], dermatological problems [8,9,26], diabetes [38,47,48], digestion problems [8,38,57], fever [23,37,64], colds [23,37,38], hypertension [8,56,65], infection [8,10,64], intoxication [10,38,49,57], magic [10,54,57], eye disease [8], kidney problems [8,50], pathologies of the reproductive system [10,40,64], respiratory problems [8,40], rheumatism [44,64,66], nervous system problems [10,40,67], spasmodic [10,38,64], head disease [23,68].
3. Materials and Methods
3.1. Description of the Study Area
Eastern Morocco is one of the largest regions of Morocco (Figure 7). He covers an area of 90 127 km2 and lies between 34°41′00″ N and 1°54′00″ W. The region has 8 administrative prefectures/provinces, namely Oujda-Angad, Berkane, Nador, Jerada, Taourirt, Driouch, Guercif, and Figuig (2014 census). Located on the plains (Angad and Triffa plains), surrounded by mountain ranges (beni-Znassen and horsts chains) and close to the Mediterranean Sea, the region of Eastern Morocco enjoys a climate and a diverse flora. Thus, 471 species and medicinal subspecies which represent 11% of the Moroccan flora, are divided into 302 genera; about 34% of all Moroccan genera, and 85 families; about 69% (Kahouadji, 1995). In addition to its floristic potential, the population of Eastern Morocco has a rich and ancient tradition in herbal medicine. The conservation and management of this floristic and cultural wealth is an important issue. Indeed, the ethnobotanical bibliography of Eastern Morocco shows that some studies on medicinal plants have been published in recent decades on the ethnobotanical knowledge of Eastern Morocco. Among these works, we quote the work of Ziyyet et al., from 1997, which made it possible to inventory the medicinal plants used by the patients for medication, diabetes, and hypertension, Fakchich J. and Alachouri in 2014 inventoried the medicinal plants used by the population to treat the different categories of diseases and the work of Alami et al. In 2015, this focuses on the plants used by diabetics in Orient Morocco.
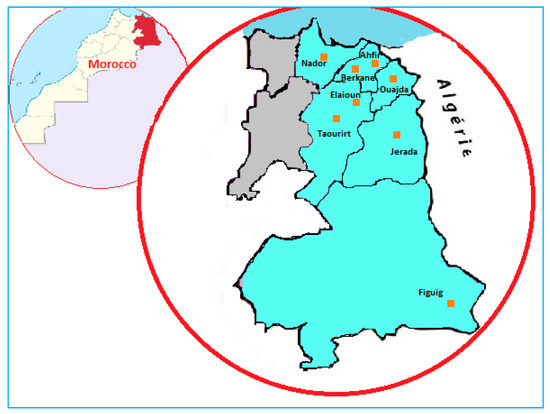
Figure 7.
The map of Eeastern Morocco with the regions of investigation.
3.2. Ethnobotanical Survey
The study area has been researched using local traditional healers. 30 THs from 8 villages were interviewed. The interviewees were all identified by snowball sampling in eight markets of eastern Morocco: Oujda, Berkane, Ahfir, Elaioun, Jerada, Nador, Taourirt, and Figuig. The involvement of the president of the association of herbalists of Morocco facilitated the approach with the (THs). Specifically, I first explained to the THs the reasons for our visit and after they agreed, we began the interview. Each survey began by collecting information on socio-demographic characteristics: sex/age/ethnicity/level of study/professional activity: description, nature of products sold, diagnoses, conservation, transmission, and toxicity. Then, information on vernacular names, medicinal uses, herbal part (s) as pharmacological uses, and preparation and treatment methods were recorded. Respondents then used a memory recall free-listing method to list the medicinal plants with which they were familiar.
3.3. Floristic Identification and Taxonomic Validation
Medicinal plants were collected or purchased, identified, labeled, and preserved at the plant section of Herbarium University Mohammed First Oujda Morocco (HUMPO). They were later verified with/on/using the African Plant Database [69] and Plant List [70]. Plants with the correct nomenclature were arranged alphabetically by family name, vernacular name, and ethnomedicinal uses.
3.4. The Vernacular Names
For the French translation of Arabic and Berber, we opted for the G.S. Colin system which is the most adapted to the local language and dialects and has the advantage of being simple and precise [3,71]. The equivalence code between Latin characters and Arabic and Berber characters are presented in Table 6.
Table 6.
Code between Latin characters and Arabic and Berber characters.
3.5. Classification of Diseases
For the classification of diseases, we adopted the alternative classification system accepted by the WHO, International Classification of Primary Care (ICPC), which was closer to ethnomedical reality with some modifications. Available online: (http://www.who.int/classifications/icd/adaptations/icpc2/en/) (accessed on 15 February 2022) (Table 5).
3.6. Data Analysis
Once the data was collected, several methods of analysis were used. Firstly, a qualitative analysis was performed to compile a catalog of medicinal plants. Second, the tow ethnobotanical indexes were used (Frequency Cited (FC) and Informant Consensus Factor (ICF)). FC is used to determine the importance of each plant within THs practices. ICF is used to determine the degree of consensus of informants (THs). Excel and Sphinx was used for analysis.
3.6.1. Frequency Cited (FC)
Frequency Cited is the number of times a plant was reported. A plant can be mentioned multiple times by a single respondent (THs).
3.6.2. Informant Consensus Factor for Each Ailment (ICF)
Informant Consensus Factor “ICF” [72,73], is calculated using the following formula:
where Nur is the number of use citations in each ailment and Nt is the number of species used for this ailment.
ICF = (Nur − Nt)/(Nur − 1)
4. Conclusions
This work has made it possible to know that most of the traditional healers surveyed are over 30 years. The overwhelming majority of traditional practitioners are male, and only one female case is among the respondents, the fact that all the owners of premises in the market are gender masculine. All the women we have met in the market who are active, are itinerant sellers. Men dominate the practice of traditional medicine in the region. The majority of traditional healers surveyed are not illiterate. The low illiteracy rate can be an advantage to the development of the practice of the trade. More than half of traditional healers said they did not practice the diagnosis of diseases. For the rest of the TPs, the diagnosis is made by questioning or by body examination and is based either on the notion of hot and cold or on the appearance and complexion of the patient. The acquisition of ancestral knowledge in less than half is done through the hereditary transfer in the extension of a family tradition or through personal experiences. Most of them do not provide a succession. In most cases, the formation of future THs is done by participatory observation, orally during the process of processing or selling plants on-premises for medication and sale of ancestral drugs. In most cases, the formation of future THs is done by participatory observation, orally during the process of processing or selling plants on-premises for medication and sale of ancestral drugs.
Thus, we recommend that traditional medicine be valued. Traditional practitioners should benefit from better supervision and a greater guarantee of the rights related to their knowledge. Being very often the first people to whom patients turn for their recovery, traditional healers will have to be trained in prevention and health promotion. They will have to open up to science to test the effectiveness and safety of the proposed remedies and direct cases that they deem beyond their competence in conventional medicine.
By interviewing 30 traditional healers on the medicinal plants used in Eastern Morocco, we were able to identify 134 species and a fungus, and we spread them over 59 families. The aerial part is the most used. The oral route is the most common route of administration by THs. The remedies used by THs generally contain compounds of vegetable, animal, and mineral origin. These remedies are in the form of simple or compound recipes. Thus, of the 135 species recorded, 42 are used in simple recipes, 93 in compound recipes, or both types of recipes.
Among these species, the most dominant are also those that are best known at the national and/or local flora scale: LAMIACEAE (12 species), FABACEAE (11 species), ASTERACEAE, and APIACEAE with 9 species. The plants that stand out for their local importance, due to their popularity, are Origanum compactum Benth, Matricaria chamomilla L., Salvia officinalis L., Peganum harmala L., Lavandula dentata L., Berberis hispanica Boiss. & Reut., Rosmarinus officinalis L. with the largest FC, NR, and NU. In Eastern Morocco, THs still possess significant knowledge and know-how explained by the high number of medicinal plants suggested for the medication of the population. This know-how is consistent with the high ICF for most diseases. The categories of ailments that have a high ICF are cancer and gastrointestinal disorders.
Author Contributions
Conceptualization, M.E. and J.F.; methodology, J.F., N.B. and M.E.; software, H.O., M.B., L.K. and J.F.; Visualization, H.Z. and N.B.; validation, M.E. and J.F.; formal analysis J.F.; data curation, J.F.; resources, M.A.W.C. and A.A.; writing—original draft preparation, J.F. and M.E.; supervision, M.E.; review and editing, M.A.W.C., N.B., L.K. and A.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2022R147), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All the data supporting the findings of this study are included in this article.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
Medicinal plants of Eeastern Morocco by THs and their descriptions in the literature.
Table A1.
Medicinal plants of Eeastern Morocco by THs and their descriptions in the literature.
| Scientific Name | Biological Type | Ecology | Provenance | Bioclimatic Stages | Biogeographic Distribution | Toxicity in Literature [7,9] |
|---|---|---|---|---|---|---|
| Acacia gummifera Willd. | Ph | P E | plains and low mountains | A SAd | Ms AA HA Mam Man | |
| Aframomum melegueta (Roscoe) K. Schum. | I. | |||||
| Ajuga iva (L.) Schreb. | hem (TH) | P E | degraded forests and scrublands, uncultivated fields, rockeries, plains and mountains | A SAd SAf SH H | all of Morocco | is not toxic but in high doses causes cephalalgia |
| Allium sativum L. | C. | is not toxic but prolonged use on the skin can produce excoriations | ||||
| Aloysia citriodora Palau | C. | its prolonged use can cause gastric irritation | ||||
| Alpinia officinarum Hance) | I. | |||||
| Ammodaucus leucotrichus Coss. & Durieu | Th | p | desert sand, river gravel | S A | Ms AA? | is not toxic at low doses |
| Ammoides pusilla (Brot.) Breistr. | Th | P E | rocky and clayey slopes, plains and low mountains | A SAd SH | MA Mam Man Op Om LM R | is not toxic at low doses |
| Anabasis aretioides Coss. & Moq. ex Bunge | Ch | A | desert, steppes | S | Ms | at low doses, it is a little toxic |
| Anacyclus pyrethrum (L.) Link | Hém | P E | forest clearings, matorrals, pastures, (plains), low, middle and high mountain | Saf SH H HM | As AA HA MA Man Op Om R | toxic in high doses; it causes headache and sometimes even the loss of consciousness |
| Anastatica hierochuntica L. | Th | H P | steppes | S A | Ms As AA | |
| Apium graveolens L. | Th-b (Hém) | P E (A) | marshes and watersides of the plains, widely cultivated | A SAd SH | Ms Mam Man Op Om LM R | |
| Arbutus pavarii Pamp. | Ph (Nph) | A H | forests and matorrals, plains, low and middle Mountains | SAd SH H | AA HA MA Mam Man Om LM R | |
| Argania spinosa (L.) Skeels | Ph | P | plains and low mountains | S A SAd | Ms AA HA Mam LM | |
| Aristolochia fontanesii Boiss. & Reut. | G | P | fields, eras, matorrals, stony, clay or sandy soils, plains, low and medium. Mountains | SAd SH H | AA HA MA Mam Man Om LM R | Aristolochin causes renal irritation up to necrosis of the epitelial elements and paralisy of the limbs |
| Artemisia herba alba Asso | CH (Hém) | E A | steppes and rocky pastures | S A SAf | Ms AA HA MA Op Om LM R | toxic in high doses |
| Astracantha gummifera (Labill.) Podlech | ||||||
| Avena sativa L. | C. | is not toxic at low doses | ||||
| Berberis hispanica Boiss. & Reut. | Nph (Ph) | P E | forests and matorrals, cracks in mountain rocks | Saf SH H | As (rare) HA MA R | |
| Beta vulgaris L. | Th, Hém | P | maritime rocks, rubble, meadows, wasteland, plains, low and mid. Mountains | A SAd SH | all of Morocco except the Saharan regions | |
| Boswellia sacra Flueck. | I. | is not toxic at low doses | ||||
| Calamintha nepeta (L.) Savi | Ch | H P E | forests and matorrals, stony erms, rocks, plains and low mountains | SAd SH H | HA HM Man Om LM R | |
| Calendula arvensis (Vaill.) L. | Th | H P E | all of Morocco | |||
| Camellia sinensis (L.) Kuntze | I., C. | is not toxic | ||||
| Cannabis sativa L. | C. | very toxic; it causes anaphrodisia | ||||
| Capparis spinosa L. | Ch (Nph) | (H) P E | rocks, walls, rocky and clay slopes, plains and low mountains | S A Sad SH | spontaneous in Morocco | several substances which have been shown to be toxic |
| Capsicum annuum L. | C. | |||||
| Carlina gummifera (L.) Less. | Hém (G) | E A | Open matorrals, hermes, wasteland, plains and low mountains | A SAD SH | HA MA Mam Man Om LM R | roots are very toxic; the heat destroys its toxic power |
| Carum carvi L. | C. | is not toxic at low doses | ||||
| Cassia senna L. var. senna | I. | |||||
| Ceratonia siliqua L. | Ph | A H | plains and low mountains | SAD (SAF) SH | As AA HA MA Mam Man Op? Om LM R | fruit is not toxic |
| Chenopodium ambrosioides L. | Th | P E A | Naturalized in fresh uncultivated environments, ditches, hedges, sandy alluvium | A SAD SH | Ms HA Mam Man Op LM R | |
| Cinnamomum cassia (L.) J.Presl | I. | |||||
| Cistus populifolius L. | Nph | P | low mountain and plains matorrals | SH H | R | |
| Citrullus colocynthis (L.) Schrad. | G | E | S A SAd | Ms As AA Mam Man Op LM R | most of the time, toxic accidents occur during attempted abortions | |
| Citrus limon (L.) Burm. f. | ||||||
| Citrus salicifolia Raf. | ||||||
| Coriandrum sativum L. | C. | |||||
| Corrigiola telephiifolia Pourr. | Hém | P E | Stony and sandy land, plains and mountains | SAD SAF SH | AA HA MA Mam Man R | |
| Costus (ND) | ||||||
| Crataegums monogyna Jacq. | Nph (Ph) | H P | low and middle Mountains | SAd SAf SH H | all of Morocco except Ms et As | |
| Crocus sativus L. | C. | is not toxic at low doses | ||||
| Cuminum cyminum L. | C. | |||||
| Curcuma longa L. | I. | |||||
| Cydonia oblonga Mill. | C. | |||||
| Cynara cardunculus L. | G | P E | pastures and wasteland, especially in clay soils, plains and low mountains | A SAd SH | MA Mam Man Op Om LM R | |
| Daphne gnidium L. | CH | P | forests, matorrals, fields, eras, plains, low and mid. Mountains | SAd SH | all of Morocco except Ms. | berries are very poisonous |
| Datura stramonium L. | Th | P E A | crops, rubble and open areas, nitrophilic | S A SAd SH | all of Morocco | plant is very poisonous |
| Delphinium staphisagria L. | Hém | P | forests and cool matorals, plains and low mountains | SH H | western rif | in high doses it causes fatal poisoning |
| Dittrichia viscosa (L.) Greuter | Ch (Nph) | E A | open environments on sufficiently humid clay substrates, waterfronts, plains and low mountains | A SAd Saf SH H | no Saharan Morocco | is not toxic at low doses |
| Elettaria cardamomum (L.) Maton | I. | |||||
| Eruca vesicaria (L.) Cav. | Th | P € | SAd (SAF) | Mam Op? LM | ||
| Eucalyptus torquata Luehm. | I. | is not toxic at low doses | ||||
| Euphorbia falcata L. | Th | P E | eras, crops, fallows, plains, low (and middle) mountains | A SAd Saf SH H | all of Morocco except the Ms | the plants for internal use, causes gastroenteritis more or less severe |
| Euphorbia resinifera O. Berg | Nph (-s) | E | limestone bedrock, low and middle Mountains | A SAd SAf | AA HA MA Mam | in high doses the plant causes hematuria and death by asphyxiation. the plant and its fresh or dry latex are dangerous products |
| Ferula communis L. | G | P E | plains, low and middle Mountains | A SAD SAF SH H | all of Morocco | very toxic |
| Foeniculum vulgare Mill. | Ch (Hém; Tb-b) | P E | uncultivated fields, arid hillsides, ravines, rocks, plains and low mountains | A SAd SAf SH H | all of Morocco except the Ms | oil is very toxic |
| Fraxinus angustifolia Vahl | Ph | H P | low and middle Mountains | SAD SAF SH H | HA MA Mam Man Om LM R | is not toxic |
| Globularia alypum L. | Ch | P | forests and matorals, plains and low mountains | A SAD SAF SH (H) | all of Morocco | is not toxic; a high dose causes headache and a lowering of temperatur |
| Glycine max (L.) Merr. | is not toxic at low doses | |||||
| Glycyrrhiza glabra L. | C. | is not toxic at low doses | ||||
| Helianthus annuus L. | C. | |||||
| Herniaria hirsuta L. | Th | (H) P E | sandy fields, places uncultivated arid | SAd SH | Mam Man LM R | |
| Hibiscus sabdariffa L. | I. | |||||
| Hordeum vulgare L. | C. | is not toxic | ||||
| Hyoscyamus albus L. | Th | P E | rubble, crops, old walls | A SAD SAF SH H | AA HA MA Mam Man Op Om LM R | toxic in high dose |
| Hyoscyamus niger L. | Th | P E | crops, rubble, plains, low and middle Mountains | SAD SH H | HA MA Man LM? R | toxic in high dose |
| Illicium verum Hook.f. | ||||||
| Juglans regia L. | C. | is not toxic at low doses | ||||
| Juncus acutus L. | Hém (GR) | P E | hygrophilic and halophilic, sands and salty mud, edges of rivers and dayas, plains, low (and mid) mountains | S A SAD SAF SH H | Ms HA Mam Man Op LM R | is not toxic at low doses |
| Lagenaria siceraria (Molina) Standl. | C. | |||||
| Laurus nobilis L. | Ph | (H) P | ravines and rocks of forests and Matorrals, plains, and mountains up to 1800 m | SH H | MA R | |
| Lavandula dentata L. | CH Nph | P A | plains and low mountains | SAd SH | AA HA MA Mam Man LM OM R | |
| Lawsonia inermis L. | C. | is not toxic at low doses | ||||
| Lepidium sativum L. | C. | is not toxic | ||||
| Linum usitatissimum L. | Th | P E | Man Man LM R | seeds containing linamarin which on hydrolysis gives cyaanhydriden acid. A high dose is toxic | ||
| Lupinus albus L. | C. | |||||
| Malus pumila Mill. | C. | |||||
| Mandragora officinarum L. | G | P E | Matorrals, ermes, uneducated places, fields | SAd SH | Mam Man LM R | several accidents and even deaths have been reported |
| Matricaria chamomilla L. | Th | H P € | Harvests, fields, uncultivated, gardens | SAd SH | Man LM R | |
| Mentha pulegium L. | Hém | P E | humid places, plains, low mountains | SAd SH H | no saharien Morocco | is not toxic in high doses, it causes loss of consciousness and cardiac disorder |
| Mentha spicata L. | C. | is not toxic | ||||
| Myristica afragrans Houtt. | I. | toxic in medium doses | ||||
| Myrtus communis L. | Nph | P | plains, and low mountains | SAd SH | Man OM LM R | not very toxic but its essence can cause headache |
| Nerium oleander L. | Nph | P E | edges of wadis | S A Sad Saf SH H | all Morocco | very toxic |
| Nigella sativa L. | C. | high dose toxic | ||||
| Ocimum basilicum L. | C. | is not toxic at low doses | ||||
| Olea europaea L. | Ph | P | plains, and low mountains | A SAd SAf SH H | no saharien Morocco | is not toxic at low doses |
| Opuntia ficus-indica (L.) Mill. | Nph | P E | plains, low and middle Mountains | A Sad SH | HA MA Mam Man Om LM R | is not toxic, ingestion of a large number of fruits causes stubborn constipation and sometimes dangerous |
| Origanum compactum Benth. | Ch | E | forests, matorrals, fields, erms, rocks, plains and low mountains | A SAd SH | MA Mam Man R | Essence of origon in high doses causes paralysis pressured by excitations |
| Origanum majorana L. | C. | in high doses gasoline is stupefying and toxic for humans | ||||
| Panax ginseng C.A.Mey. | I. | |||||
| Papaver rhoeas L. | Th | P E | fields, harvests, wasteland, plains, low and middle mountains | A SAd SAf SH H | all of Morocco | |
| Papaver somniferum L. | Th | (H) P E | fields, uncultivated places, plains, low and mid. Mountains | S A SAD SAF SH | all of Morocco | |
| Peganum harmala L. | CH | P E | steps, uncultivated fields, rubble, plains and low mountains | S A SAd | all of Morocco | is not toxic at low doses |
| Phillyrea angustifolia L. | Ph | H P | clear forests and Matorals, plains, low and middle Mountains | SAd SH H | As? HA MA Man R | |
| Phoenix dactylifera L. | C. | P | Saharan and arid streams and oases | S A | Ms As AA HA Mam | is not toxic |
| Pimpinella anisum L. | C. | in high doses, it causes stupidity and convulsions | ||||
| Piper cubeba L. f. | I. | |||||
| Piper longum L. | I. | |||||
| Piper nigrum L. | I. | is not toxic at low doses | ||||
| Pistacia atlantica Desf. | Ph | P E | lains, low and middle mountains | A SAd SAf SH | all of Morocco | In low doses, the fruit is not toxic |
| Pistacia Ientiscus L. | Ph | P | plaines, basses (et moy.) montagnes | SAD SH H | As AA HA MA Mam Man Om LM R | is not toxic at low doses |
| Prunus dulcis (Mill.) D. A. Webb | Ph | H P | orests and rocks | SAd SH H | MA Mam Om R | |
| Punica granatum L. | C. | high dose bark is very toxic | ||||
| Quercus faginea Lam. | Ph | h | N.Afr. | |||
| Quercus suber L. | Ph | P E | plains, low and middle mountains | SH H | HA MA Man R | |
| Ricinus communis L. | seeds is very toxic | |||||
| Rosa centifolia L. | C. | |||||
| Rosmarinus officinalis L. | contains a toxic gasoline in high dose, it causes tomacal hemorrhage, albuminuria and steatosis of the liver | |||||
| Rubia peregrina L. | Ch (G) | P E | forests and matorals, low and middle plains Mountains | A SAd SAf SH H | HA MA Mam Man Om LM R | is not toxic at low dose |
| Ruta chalepensis L. | Ch | P E | clear forests, dry uncultivated hillsides, rocks, plains, low and middle mountains | A SAd SAf SH | HA? Mam Man Om R | is not toxic at low doses |
| Salvia officinalis L. | C. | |||||
| Sesamum indicum L. | C. | |||||
| Sorghum bicolor (L.) Moench | C. | |||||
| Syzygium aromaticum (L.) Merr. & L. M. Perry(3) | I. | I. | ||||
| Tamarindus indica L. | I. | |||||
| Telephium imperati L. | hém (ch) | P E | rocky erms and mountain rocks | SAf SH HM | As AA HA MA Man Op Om R | |
| Terminalia chebula Retz. | ||||||
| Tetraclinis articulata (Vahl) Mast. | Ph | E | plains, low (and middle) mountains | SAd (SH) | AA HA MA Mam Man Op Om LM R | is not toxic at low doses |
| Tetraena gaetula (Emb. & Maire) Beier & Thulin | Ch | P E | epandage argileux salés | Ms oriental | ||
| Thymelaea hirsuta (L.) Endl. | Nph | H P | steps, forest glades, rockeries | A SAd SAf SH | As AA occidental HA MA Mam Op Om LM? R? | |
| Thymus broussonetii Boiss. | Ch | P | clear forests and Matorrals, plains and low mountains | A SAd | HA Mam Man | |
| Tilia sylvestris Desf. | I. | |||||
| Trigonella foenum-graecum L. | C. | |||||
| Urtica dioïca L. | GR | P E | wet cultivated places, fresh ravines | A | Mam | a decoction administered internally may cause eczema and urine retention |
| Valeriana celtica L. | G | E | limestone and sand-limestone rocks, high mountains | SAf SH HM | MA north eastern | |
| Vicia faba L. | C. | |||||
| Viscum album L. | Ch (-p) | P E | wet forests | H | ||
| Vitis vinifera L. | C. | |||||
| Warionia saharae Benth. & Coss. | Nph | P E | substrate rocky, plains, low mountains | S A SAd | Ms As AA HA Mam | |
| Zea mays L. | C. | is not toxic at low doses | ||||
| Zingiber officinale Roscoe | I. | I. | is not toxic; in high doses it can cause amnesia | |||
| Ziziphus lotus (L.) Lam. | (Ph) Nph | P E | not forest areas, plains, low (and middle) mountains | S A SAd SAf SH | all of Morocco | fruit is not toxic in low doses |
Abbreviation: Biological type: Classification adopted by Sauvage (1961) in the Flore des Subéraies Marocaines and by Fennane et al. (1999 and 2007) in the Flore Pratique du Maroc, volume 1 and 2: Ph: Phanérophytes (trees); Nph: Nanophanérophytes (shrubs and shrubs); Ch: Chamephytes, G: geophyte (bulb, rhizome, tuber), Hem: haemicophyte, NPh: nanophanerophyte, Ph: phanerophyte, Th: therophyte. Bioclimatic stages: Defined by Emberger (1939); S: Saharan, A: Arid, SA: Semi-arid, SH: Subhumide, H: Humid, HM: High Mountains, Phytogeographic Divisions: according to Fennan et al. 1999–2014; Ms (Saharan Morocco), As (Saharan Atlas), AA (Anti Atlas), HA (High Atlas), MA (Middle Atlas), Mam (Middle Atlantic Morocco), Man (North Atlantic Morocco), Op (Eastern Plateaus), Om (Eastern Morocco Mountains), LM (Mediterranean Coast), R (Rif). Ecological status: C (cultivated); I (imported), N.Afr. (endemic to North Africa); Mar. (endemic to Morocco); S-W. Mar. (endemic to South West of Morocco); Medit. and Sah.-Sindh. (endemic to the Mediterranean and Sindian Sahara); Medit. (endemic to the Mediterranean); N.Afr. and Eur (endemic to northern Africa and Europe).
References
- Elachouri, M.; Kharchoufa, L.; Fakchich, J.; Lorigooini, Z. Ancestral phytotherapeutic practices in Morocco: Regards on history, current state, regulatory and safety of commonly used herbal medicine. Arab. J. Chem. Environ. Res. 2021, 8, 133–149. [Google Scholar]
- Renaud, H.-C. Tuhfat Al-Ahbāb Glossaire de la Matière Médicale; Marocaine: Paris, France, 1934. [Google Scholar]
- Bellakhdar, J. La pharmacopée marocaine traditionnelle. In Médecine arabe Ancienne et Savoirs Populaires; Ibis Press: Paris, French, 1997. [Google Scholar]
- Claisse-Dauchy, R.; de Foucault, B. Médecine arabo-musulmane: Modes de transmission des savoirs au Maroc (régions de Meknès et Rabat-Salé). Des. Sources Du Savoir Aux Médicaments Du Futur. 2016, 321–326. [Google Scholar] [CrossRef]
- Bammou, M.; Daoudi, A.; Sellam, K.; El Rhaffari, L.; Ibijbijen, J.; Nassiri, L. Étude Ethnobotanique des Astéracées dans la Région Meknès-Tafilalet (Maroc)/[Ethnobotanical Survey of Asteraceae Family used in Meknes-Tafilalet Region (Morocco)]. Int. J. Innov. Appl. Stud. 2015, 13, 789–815. [Google Scholar]
- Addo-Fordjour, P.; Anning, A.K.; Atakora, E.A.; Agyei, P.S. Diversity and distribution of climbing plants in a semi-deciduous rain forest, KNUST Botanic Garden, Ghana. Int. J. Bot. 2008, 4, 186–195. [Google Scholar] [CrossRef]
- Benítez, G.; González-Tejero, M.R.; Molero-Mesa, J. Pharmaceutical ethnobotany in the western part of Granada province (southern Spain): Ethnopharmacological synthesis. J. Ethnopharmacol. 2010, 129, 87–105. [Google Scholar] [CrossRef]
- El Rhaffari, L.; Zaid, A. Pratique de la phytothérapie dans le sud-est du Maroc (Tafilalet). Un savoir empirique pour une pharmacopée rénovée. Des Sources Du Savoir Aux Médicaments Du Futur. 2001, 293–318. [Google Scholar] [CrossRef]
- Abouri, M.; El Mousadik, A.; Msanda, F.; Boubaker, H.; Saadi, B.; Khalil, C. An ethnobotanical survey of medicinal plants used in Terai forest of western Nepal. J. Ethnobiol. Ethnomed. 2012, 8, 99–123. [Google Scholar] [CrossRef]
- Saadi, B.; Msanda, F.; Boubaker, H. Contributions of folk medicine knowledge in South- western Morocco: The case of rural communities of Imouzzer Ida Outanane Region. Int. J. Med. Plant. Res. 2013, 2, 135–145. [Google Scholar]
- El-Hilaly, J.; Hmammouchi, M.; Lyoussi, B. Ethnobotanical studies and economic evaluation of medicinal plants in Taounate province (Northern Morocco). J. Ethnopharmacol. 2002, 86, 149–158. [Google Scholar] [CrossRef]
- Oualidi, J.E.L.; Khamar, H.; Fennane, M. Checklist des Endémiques et Spécimens Types de la Flore Vasculaire de l’Afrique du Nord. Doc. De L’Institut Sci. 2012, 25, 1–189. [Google Scholar]
- Fennane, M.; Ejdali, M. Aromatic and medicinal plants of Morocco: Richness, diversity and threats Plantes aromatiques et médicinales du Maroc: Richesse, diversité et menaces. Bull. L’institut Sci. Rabat. Sect. Sci. La Vie 2016, 38, 27–42. [Google Scholar] [CrossRef]
- Fakchich, J.; Elachouri, M. An overview on ethnobotanico-pharmacological studies carried out in Morocco, from 1991 to 2015: Systematic review (part 1). J. Ethnopharmacol. 2021, 267, 113200. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, A.; Jamila, F.; Mostafa, E. First insight on ethnobotanical appraisal of plants used traditionally as medicine by berber community (Amazigh-speaking), living in driouch province (north-eastern morocco). Ethnobot. Res. Appl. 2021, 22, 1–71. [Google Scholar] [CrossRef]
- Ziyyat, A.; Legssyer, A.; Mekhfi, H.; Dassouli, A.; Serhrouchni, M.; Benjelloun, W. Phytotherapy of hypertension and diabetes in oriental Morocco. J. Ethnopharmacol. 1997, 58, 45–54. [Google Scholar] [CrossRef]
- Lahsissene, H.; Aahouadi, K.; Tijane, M.; Hseini, S. Catalogue Des Plantes Medicinales Utilisées Dans La Région De Zaër (Maroc Occidental). Lejeunia. Rev. Bot. 2009, 186, 1–26. [Google Scholar]
- Bencheikh, N.; Elbouzidi, A.; Kharchoufa, L.; Ouassou, H.; Merrouni, I.A.; Mechchate, H.; Es-Safi, I.; Hano, C.; Addi, M.; Bouhrim, M.; et al. Inventory of medicinal plants used traditionally to manage kidney diseases in north-eastern Morocc: Ethnobotanical fieldwork and pharmacological evidence. Plants 2021, 10, 1966. [Google Scholar] [CrossRef]
- Ilyass, A.M.; Loubna, K.; Noureddine, B.; Mostafa, E. Ethnobotanical profile of medicinal plants used by people of North-eastern Morocco: Cross-cultural and historical approach (part I). Ethnobot. Res. Appl. 2021, 21, 1–45. [Google Scholar] [CrossRef]
- Charnot, A. La Toxicologie au Maroc, Mémoire de la Société des Sciences Naturelles du Maroc; Emile Larose: Paris, French, 1945; pp. 572–598. [Google Scholar]
- Bruneton, J. Plantes Toxiques: Vegetaux Dangereux Pour L’homme et Les Animaux; Tec: Paris, French, 1996. [Google Scholar]
- Kharchoufa, L.; Bouhrim, M.; Bencheikh, N.; Addi, M.; Hano, C.; Mechchate, H.; Elachouri, M. Potential toxicity of medicinal plants inventoried in northeastern Morocco: An ethnobotanical approach. Plants 2021, 10, 1108. [Google Scholar] [CrossRef]
- Benlamdini, N.; Elhafian, M.; Rochdi, A.; Zidane, L. Étude floristique et ethnobotanique de la flore médicinale du Haut Atlas oriental (Haute Moulouya). J. Appl. Biosci. 2014, 78, 6771. [Google Scholar] [CrossRef]
- Salhi, S.; Fadli, M.; Zidane, L.; Douira, A. Etudes floristique et ethnobotanique des plantes médicinales de la ville de Kénitra (Maroc) Souad. Mediterr. Bot. 2010, 31, 133–146. [Google Scholar] [CrossRef]
- Ghourri, M.; Zidane, L.; Houda, E.Y.; Rochdi, A.; Fadli, M.; Douira, A. Etude floristique et ethnobotanique des plantes médicinales de la ville d’El Ouatia (Maroc saharien). Kastamonu Univ. J. For. Fac. 2012, 12, 218–235. [Google Scholar] [CrossRef]
- Bouayyadi, L.; El Hafian, M.; Zidane, L. Étude floristique et ethnobotanique de la flore médicinale dans la région du Gharb, Maroc. J. Appl. Biosci. 2015, 93, 8770. [Google Scholar] [CrossRef]
- El Yahyaoui, O.; Ouaaziz, N.A.; Sammama, A.; Kerrouri, S.; Bouabid, B.; Lrhorfi, L.A.; Zidane, L.; Bengueddour, R. Etude ethnobotanique: Plantes médicinales commercialisées à la province de Laâyoune; identification et utilisation [Ethnobotanical Study: Medicinal plants commercialized in the province of Laayoune; identification and use]. Int. J. Innov. Appl. Stud. 2015, 12, 533. [Google Scholar]
- Zerkani, H.; Tagnaout, I.; Zair, T.; Meknes, Z. Ethnobotanical survey and inventory of medicinal flora in the rural municipalities of Ait Ishaq, Tighassaline, El-Hammam and Ageulmam azegza—Khenifra province, Morocco. J. Chem. Pharm. Res. 2015, 7, 611–627. [Google Scholar] [CrossRef]
- Poffenberger, M.; Singh, S. Forest management partnerships: Regenerating India’s forests. Unasylva 1992, 43, 46. [Google Scholar]
- Bitsindou, M. Enquête sur la Phytothérapie Traditionnelle à Kindamba et Odzala (Congo) et Analyse de Convergence D’usage des Plantes Médicinale en Afrique Centrale Mem; Doc Ined.; Université Libre de Bruxelles: Brussels, Belgium, 1986. [Google Scholar]
- Bigendako-Polygenis, M.J.; Lejoly, J. La pharmacopée traditionnelle au Burundi. Pesticides et médicaments en santé animale. Pres. Univ. Namur. 1990, 45, 425–442. [Google Scholar]
- Didi, O.E.H.M.; Hadj-Mahammed, M.; Zabeirou, H. Place Des Plantes Spontanees Dans La Medecine Traditionnelle De La Region De OUARGLA (Sahara Septentrional Est). Courr. Du Savoir 2003, 3, 47–51. [Google Scholar]
- Yapi, A. Inventaire des Plantes Médicinales de la Famille des Asteraceae des Marchés de la Commune d’Abobo (Abidjan, Côte d’Ivoire); Université Félix Houphouët-Boigny: Abidjan, Côte d’Ivoire, 2013. [Google Scholar]
- Jaiswal, Y.; Liang, Z.; Zhao, Z. Botanical Drugs in Ayurveda and Traditional Chinese Medicine; Elsevier: Amsterdam, The Netherlands, 2016; Volume 194, ISBN 1700018000. [Google Scholar]
- Ghourri, M.; Zidane, L.; Douira, A. Usage des plantes médicinales dans le traitement du Diabète Au Sahara marocain (Tan-Tan). Japs 2013, 17, 2388–2411. [Google Scholar]
- Messaoudi, M.; Filali, H.; Tazi, A.; Hakkou, F. Ethnobotannical surveys of healing medicinal plants traditionally used in the main Moroccan citiees. J. Pharmacogn. Phyther. Full 2015, 7, 164–182. [Google Scholar]
- Rhaffari, L.; Hammani, K.; Benlyas, M.; Zaid, A. Traitement de la leishmaniose cutanée par la phytothérapie au Tafilalet. Biol. Santé 2002, 1, 45–54. [Google Scholar]
- Benkhnigue, O.; Zidane, L.; Fadli, M.; Elyacoubi, H.; Rochdi, A.; Douira, A. Etude ethnobotanique des plantes médicinales dans la région de Mechraâ Bel Ksiri (Région du Gharb du Maroc). Acta Botánica Barcinonensia 2011, 53, 191–216. [Google Scholar]
- Zhao, Z.; Liang, Z.; Chan, K.; Lu, G.; Lee, E.L.M.; Chen, H.; Li, L. A unique issue in the standardization of Chinese materia medica: Processing. Planta Med. 2010, 76, 1975–1986. [Google Scholar] [CrossRef] [PubMed]
- Ouhaddou, H.; Boubaker, H.; Msanda, F.; El Mousadik, A. An ethnobotanical study of medicinal plants of the Agadir Ida Ou Tanane province (southwest Morocco). J. Appl. Biosci. 2015, 84, 7707. [Google Scholar] [CrossRef]
- El–Said, F.; Sofowora, E.A.; Malcolm, S.A.; Hofer, A. An investigation into the efficacy of Ocimum gratissimum as used in Nigerian native medicine. Planta Med. 1969, 17, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Fleurentin, J.; Pelt, J.M. Las plantas medicinales. Mundo Científico 1990, 105, 926–934. [Google Scholar]
- Bussmann, R.W.; Sharon, D. Traditional medicinal plant use in Northern Peru: Tracking two thousand years of healing culture. J. Ethnobiol. Ethnomedicine 2006, 2, 47. [Google Scholar] [CrossRef] [PubMed]
- Fakchich, J.; Elachouri, M. Ethnobotanical survey of medicinal plants used by people in Oriental Morocco to manage various ailments. J. Ethnopharmacol. 2014, 154, 76–87. [Google Scholar] [CrossRef]
- Briguiche, H.; Rochdi, A.; Zidane, L. The catalogue of medicinal plants used in the region of El Jadida. Int. J. Herb. Med. 2015, 2, 46–54. [Google Scholar]
- El Hafian, M.; Benlandini, N.; Elyacoubi, H.; Zidane, L.; Rochdi, A. Étude floristique et ethnobotanique des plantes médicinales utilisées au niveau de la préfecture d’Agadir-Ida-Outanane (Maroc). J. Appl. Biosci. 2014, 81, 7198. [Google Scholar] [CrossRef]
- Benkhnigue, O.; Akka, F.B.; Salhi, S.; Fadli, M.; Zidane, A.D.e.L. Catalogue des plantes médicinales utilisées dans le traitement du diabète dans la région d’Al. J. Anim. Plant Sci. 2014, 23, 3539–3568. [Google Scholar]
- Alami, Z.; Aynaou, H.; Alami, B.; Hdidou, Y.; Latrech, H. Herbal medicines use among diabetic patients in Oriental Morocco. J. Pharmacogn. Phyther. 2015, 7, 9–17. [Google Scholar] [CrossRef]
- Ait, A.; Said, H.; Derfoufi, S.; Sbai, I.; Benmoussa, A. Research Article Ethnopharmacological survey of traditional medicinal plants used for the treatment of infantile colic in Morocco. J. Chem. Pharm. Res. 2015, 7, 664–671. [Google Scholar]
- Ghourri, M.; Zidane, L.; Douira, A. La phytothérapie et les infections urinaires (La pyélonéphrite et la cystite) au Sahara Marocain. J. Anim. Plant. Sci. 2014, 20, 3171–3193. [Google Scholar]
- Bellakhdar, J. Repertory of standard herbal drugs in the Maroccan pharmacopoea. J. Ethnopharmacol. 1991, 35, 123–143. [Google Scholar] [CrossRef]
- El Hilah, F.; Ben Akka, F.; Dahmani, J.; Belahbib, N.; Zidane, L. Étude Ethnobotanique Des Plantes Médicinales Utilisées Dans Le Traitement Des Infections Du Système Respiratoire Dans Le Plateau Central Marocain. J. Anim. Plant Sci. 2015, 25, 3886–3897. [Google Scholar]
- Mikou, K.; Rachiq, S.; Oulidi, A.J.; Beniaich, G. Étude ethnobotanique des plantes médicinales et aromatiques utilisées dans la ville de Fès au MarocEthnobotanical survey of medicinal and aromatic plants used by the people of Fez in Morocco. Phytothérapie 2016, 14, 35–43. [Google Scholar] [CrossRef]
- Fadil, M.; Farah, A.; Haloui, T.; Rachiq, S. Étude ethnobotanique des plantes exploitées par les coopératives et les associations de la région Meknès-Tafilalet au Maroc. Phytotherapie 2015, 13, 19–30. [Google Scholar] [CrossRef]
- Daoudi, A.; Bammou, M.; Zarkani, S.; Slimani, I.; Ibijbijen, J.; Nassiri, L. Étude ethnobotanique de la flore médicinale dans la commune rurale d’Aguelmouss province de Khénifra (Maroc). Phytotherapie 2015, 14, 220–228. [Google Scholar] [CrossRef]
- Eddouks, M.; Maghrani, M.; Lemhadri, A.; Ouahidi, M.L.; Jouad, H. Ethnopharmacological survey of medicinal plants used for the treatment of diabetes mellitus, hypertension and cardiac diseases in the south-east region of Morocco (Tafilalet). J. Ethnopharmacol. 2002, 82, 97–103. [Google Scholar] [CrossRef]
- Merzouki, A.; Ed-derfoufi, F.; Molero Mesa, J. Contribution to the knowledge of Rifian traditional medicine. II: Folk medicine in Ksar Lakbir district (NW Morocco). Fitoterapia 2000, 71, 278–307. [Google Scholar] [CrossRef]
- Orch, H.; Douira, A. Étude ethnobotanique des plantes médicinales utilisées dans le traitement du diabète, et des maladies cardiaques dans la région d ’ Izarène (Nord du Maroc). J. Appl. Biosci. 2015, 86, 7940–7956. [Google Scholar] [CrossRef]
- Tahri, N.; Basti, A.E.L.; Zidane, L.; Rochdi, A.; Douira, A. Etude ethnobotanique des plantes medicinales dans La province de settat (Maroc). J. For. Fac. 2012, 12, 192–208. [Google Scholar]
- Hseini, S.; Kahouadji, A.; Lahssissene, H.; Tijane, M. Analyses floristique et ethnobotanique des plantes vasculaires médicinales utilisées dans la région de Rabat (Maroc occidental). Mediterr. Bot. 2007, 100, 93–100. [Google Scholar]
- Bensalem, S.; Soubhye, J.; Aldib, I.; Bournine, L.; Nguyen, A.T.; Vanhaeverbeek, M.; Rousseau, A.; Boudjeltia, K.Z.; Sarakbi, A.; Kauffmann, J.M.; et al. Inhibition of myeloperoxidase activity by the alkaloids of Peganum harmala L. (Zygophyllaceae). J. Ethnopharmacol. 2014, 154, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Chebat, A.; Skalli, S.; Errihani, H.; Boulaâmane, L.; Mokrim, M.; Mahfoud, T.; Soulaymani, R.; Kahouadji, A. Étude de prévalence des effets indésirables liés à l’utilisation des plantes médicinales par les patients de l’Institut National d’Oncologie, Rabat. Phytotherapie 2014, 12, 25–32. [Google Scholar] [CrossRef]
- Kabbaj, F.Z.; Meddah, B.; Cherrah, Y.; El, M.; Faouzi, A. Ethnopharmacological profile of traditional plants used in Morocco by cancer patients as herbal therapeutics. Phytopharmacology 2012, 2, 243–256. [Google Scholar]
- El Abbouyi, P.A.; Filali-Ansari, N.; Khyari, P.S.; Loukili, H. Inventory of medicinal plants prescribed by traditional healers in El Jadida city and suburbs (Morocco). Int. J. Green Pharm. 2014, 8, 242–251. [Google Scholar] [CrossRef]
- Tahraoui, A.; El-Hilaly, J.; Israili, Z.H.; Lyoussi, B. Ethnopharmacological survey of plants used in the traditional treatment of hypertension and diabetes in south-eastern Morocco (Errachidia province). J. Ethnopharmacol. 2007, 110, 105–117. [Google Scholar] [CrossRef]
- Ouarghidi, A.; Martin, G.J.; Powell, B.; Esser, G.; Abbad, A. Botanical identification of medicinal roots collected and traded in Morocco and comparison to the existing literature. J. Ethnobiol. Ethnomed. 2013, 9, 1. [Google Scholar] [CrossRef]
- Zeggwagh, A.A.; Lahlou, Y.; Bousliman, Y. Enquete sur les aspects toxicologiques de la phytotherapie utilisee par un herboriste à Fes, Maroc. Pan Afr. Med. J. 2013, 14, 1–6. [Google Scholar] [CrossRef]
- EL Hassani, M.; Douiri, E.M.; Bammi, J.; Zidane, L.; Badoc, A.; Douira, A. Plantes médicinales de la Moyenne Moulouya (Nord-Est du Maroc). Ethnopharmacologia 2013, 50, 39. [Google Scholar]
- African Plants (Version 3.4.0). 2016. Available online: http://africanplantdatabase.ch (accessed on 15 February 2022).
- Plant List (Version 1.1. September 2013). Available online: http://www.theplantlist.org (accessed on 15 February 2022).
- Ennaji, M. Multilingualism, Cultural Identity, and Education in Morocco; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2005. [Google Scholar]
- Trotter, R.; Logan, M. Informant consensus: A new approach for identifying potentially effective medicinal plants. Plants Indig. Med. Diet. Routledge 2019, 91–112. [Google Scholar]
- Heinrich, M.; Ankli, A.; Frei, B.; Weimann, C.; Sticher, O. Medicinal plants in Mexico: Healers’ consensus and cultural importance. Soc. Sci. Med. 1998, 47, 1859–1871. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).