Abstract
The present study investigated the feasibility and effectiveness of pseudo-weight resistance training using mixed-reality (MR) technology for shoulder muscle activation in healthy individuals. Thirty-two healthy students aged 20~35 years participated in this preliminary study and were divided into two groups. Participants in the MR group received 30 min of training three times a week for 4 weeks using a customized MR-based pseudo-weight resistance training system. Those in the control group performed the same exercises using a conventional training program. Muscle activation of the deltoids, upper trapezius, infraspinatus, and supraspinatus were measured before and after the intervention. There was a statistically significant difference in middle deltoid, upper trapezius, and supraspinatus muscle activation in the MR group (p < 0.05), while the control group showed a significant difference in the anterior and middle deltoid, upper trapezius, and supraspinatus (p < 0.05). Regarding the between-group comparison, no statistically significant difference was observed for all six muscles (p > 0.05). Without any superiority of physical weight resistance training in the pseudo-weight training program, an MR-based pseudo-weight resistance training system can potentially be used for muscle-strengthening training, especially for early rehabilitation programs. However, further study using a large sample size with a long experimental duration is needed for more evidence of the presented technology and its use in home training.
1. Introduction
The rapid growth of science and technology has made possible the development of many computer-altered technologies that can intensify or replace our perception of the world. These technologies comprise virtual reality (VR), augmented reality (AR), and mixed reality (MR) [1]. Having many potential benefits, these technologies are making important changes in various areas and components of our daily life [2].
VR, which is technology that immerses users within a computer-generated virtual environment [3,4], and AR, which encrusts digital content on top of the physical world [4,5], are used for entertainment, training, education [6], and healthcare, such as in rehabilitation [7]. VR and AR are often used in rehabilitation as gamified exercises (exergames) and have been reported to be effective in improving physical performance, including muscle strength, in healthy individuals as well as in patients with disorders and impairments [8,9]. These findings probably result from the fact that exergames provide enjoyable and challenging experiences. These types of immersive experiences can make users train more safely and can motivate patients during home exercise programs in a new and exciting way [10]. However, it remains difficult for healthcare providers and patients themselves to quantify the intensity of the exercise performed during exergames. Although the implementation of additional devices such as treadmills and stationary bicycles may help to quantify and manage the intensity of the exergames played by patients during training sessions [11], buying and installing those devices requires more expense and an adequate environment.
Another method used to quantify the weights of objects manipulated during exergames is pseudo-haptic technology, which provides real-time haptic feedback. A pseudo-weight can be described as a virtual weight that can be perceived without any contact with a physical weight [12]. This technology has been applied to users by providing a sense of touch when they catch or manipulate virtual objects using haptic devices [13]. There have been numerous wearable pseudo-haptic devices in the form of haptic gloves that provide touch and weight sensations. However, they have been found to reduce the user’s natural range of motion during exercise and remain expensive [14]. With the emergence of MR, which is a technology that combines AR and VR features, as it merges the real and virtual environments’ [2] visual cues (interactive imagination), MR can be used to create a more efficient pseudo-weight based on visualization and perception. Moreover, since MR stimulates users’ imaginations and interactions and is capable of maintaining both real and virtual worlds, this new approach of pseudo-weight training using visual cues can be translated into haptic feedback [15,16].
In a previous study, Park [17] developed an algorithm that uses machine learning and created a virtual pseudo-weight technique that only relies on the user’s perception and visualization and is sensible to movement directions and velocity. Despite the development of this new approach, which does not require pseudo-haptic devices, such as haptic gloves, no study has been conducted to assess its feasibility and effectiveness on muscle activation. It is well known that resistance exercise is an effective method to assess the activity of muscles, as it produces strong muscle contractions when an external force has been applied. Previous studies have shown that several impacts of resistance training help to increase muscle activation and the cross-sectional area of muscle fibers, increase muscle strength [18], and delay the aging-related process of sarcopenia [19]. Therefore, performing resistance exercises may result in increasing muscle power for a healthy life, which is one of the principal reasons for improving muscle performance in various cases [20]. Another important factor influencing muscle contractions is that the central nervous system plays a crucial role as a regulator and stimulates the fast or slow twitch of fibers [21]. It would be of much interest to assess the effects of using pseudo-weights for resistance training with MR technology on muscle activation.
To date, there has been less interest in research regarding pseudo-weight technology in rehabilitation, especially in home training programs. To our knowledge, no research has assessed the effects of pseudo-weight resistance training using MR technology on muscle activation or, more particularly, on its short-term effects. Therefore, the goal of the present study was to assess the effects of pseudo-weight training using HoloLens MR Glasses on shoulder muscle activation in an attempt to determine its feasibility in healthy young adults.
2. Materials and Methods
2.1. Research Design
The present study was a randomized, controlled trial preliminary study with two groups (the MR group and the control group) with a pre-test and post-test measurement design, conducted in the Department of Physical Therapy, Sun Moon University, Republic of Korea. The study procedure followed the Declaration of Helsinki and was approved by the Institutional Review Board of Sun Moon University (SM-202206-028-2). Before participating in this study, all participants were informed of the aims of the study and the procedure and were allowed to ask questions. All signed an informed consent form.
2.2. Sample Size Calculation
The sample in this study was calculated by the software G∗power version 3.1.9.7 (Heinrich Heine, Düsseldorf, Germany). The calculations were made with a 0.25 effect size, 0.05 alpha level, two groups, and four measurements. According to these parameters, a sample size of 30 participants was required to achieve a power of 90%. One more participant was added to each group in case of dropouts, for a total of 32 participants.
2.3. Participants
A total of thirty-two (32) volunteers (14 women and 18 men) were recruited for this study. All participants were healthy college students without surgery or upper or lower extremity injuries within the preceding three months. Only participants who had at least some experience of using VR or AR devices and did not have any problem with maintaining standing stability were included in the experiment. Participants who had any significant shoulder injury or surgical history were excluded. During the experiment, all participants were instructed to refrain from intensive exercise and received monetary compensation at the end of the experiment for the time and effort they provided.
2.4. Randomization
In the present study, we used the simple randomization method and conducted it using a computerized random number generator from 1 to 32. Participants with odd numbers were allocated to the MR group and those with even numbers to the control group. The number randomization procedure was conducted by an investigator who was not involved in outcome measurement, intervention, or data analysis.
2.5. MR Group
Participants allocated to the MR group used a commercially available head-mounted Microsoft HoloLens 2 device (Microsoft Corporation, Redmond, Washington, DC, USA). The HoloLens was configured using the pseudo-weight algorithm developed by the Data Reality Corporation (Seoul, Republic of Korea) and a rehabilitation exercise program designed in the Department of Physical Therapy of Sun Moon University. The pseudo-weight training consisted of participants training using a virtual weight (dumbbell), lifting it as if it was physically real. The force needed to lift the dumbbell was the same as the force required for the real dumbbell, including the velocity and direction of the movement. Details of the pseudo-weight algorithm and its integration are published elsewhere [17]. The MR environment created through the HoloLens made it possible to present digital objects such as dumbbells and trainer avatars as if they were in the real world, mixing them with the surrounding environment. Moreover, the upper body of each participant was replaced by an avatar, allowing them to be present at the virtual training center event (they were physically in a laboratory room). The upper-body avatar was colored green when the exercise was correctly performed and turned red when incorrect movement was executed (e.g., flexion instead of abduction). The exercises were performed in this designed MR environment. Before performing the exercises, participants had 15 min to practice using the MR Glass while four (4) inertial measurement unit (IMU) sensors were attached to their upper limb joints (2 IMU sensors at 5 cm above the elbow and 2 others at the wrist). The IMU sensors were used to provide participants with feedback on the ongoing exercises (acceleration and deceleration of the movement) to ensure the correct performance of the movements (Figure 1).
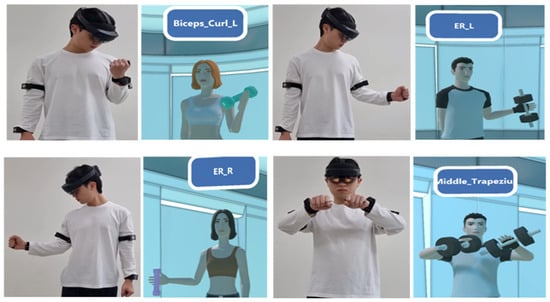
Figure 1.
Exercise accuracy practice using IMU sensors.
For this study, participants were asked to perform three different exercises (10 repetitions × 3 sets for each exercise), always in the same order: (1) shoulder scaption (standing position), (2) shoulder press (sitting position), and (3) shoulder external rotation (standing position) with 10 kg (1 RM) for males and 8 kg (1 RM) for females. The weight of 10 kg for males was chosen based on previous studies that used 10 kg as a weight to fully stimulate the muscle [22]. The 8 kg weight for females was adapted to our participants since they were unable to lift the 10 kg dumbbell for 10 repetitions. The selected exercises were designed to target the deltoids, the upper trapezius, the infraspinatus, and the supraspinatus muscles, as they involved a combination of shoulder flexion, abduction, and external rotation. Additionally, the chosen exercises are among the exercises recommended by Moseley et al. [23] for shoulder rehabilitation programs. Participants were instructed to perform the exercises by following the instructions given by a trainer avatar with a pre-recorded audio voice. Participants were asked to wear the HoloLens during exercise performance as well as during the electromyography (EMG) measurement. However, they were instructed to remove it during the resting periods. After completing the MR Glass exercise program, participants were asked to fill out a customized survey to evaluate their subjective feelings about using the MR Glass device. The survey consisted of ten questions with a simple “yes or no” answer. Figure 2 shows the screen of the MR-based pseudo-weight system and Figure 3 the exercise performed by the HoloLens device.
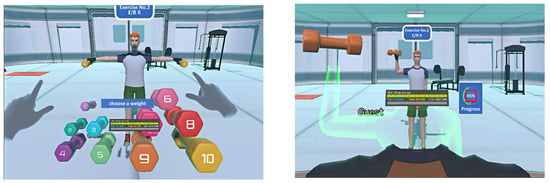
Figure 2.
MR-based pseudo-weight system screen.
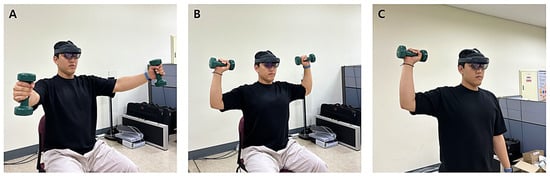
Figure 3.
Training using a HoloLens device: (A) shoulder scaption, (B) shoulder press, (C) shoulder external rotation.
2.6. Control Group
Participants in the control group were asked to perform the same tasks as those in the MR group by using real physical dumbbells, without using the MR Glass. They performed the same number of repetitions and sets as those in the MR group (10 repetitions × 3 sets for each exercise): (i) shoulder scaption (standing position), (ii) shoulder press (sitting position), (iii) shoulder external rotation (standing position) with 10 kg (1 RM) for males and 8 kg (1 RM) for females.
2.7. Outcome Measurement
EMG signals were recorded simultaneously from six shoulder muscles using a surface EMG. The surface EMG used for the recording was a portable 4-channel BTS-FREEEMG Muscle Tester (BTS Bioengineering Corp, Seoul, Republic of Korea) with wireless electrodes. Electrodes were positioned on the belly of the deltoids (anterior, middle, posterior), upper trapezius, infraspinatus, and supraspinatus of the dominant side. Arm dominance was determined by the arm used for writing. The electrodes were positioned according to previous studies [24,25], and the detailed position of each muscle is presented in Table 1. The distance between the electrodes was a minimum of 2 cm. The same investigator was responsible for placing all electrodes in order to ensure the consistency of the measurement. Signals were cleared using a bandwidth frequency ranging from 10 to 1500 Hz. A computer equipped with BTS-FREEEMG (BTS Bioengineering Corp, Seoul, Republic of Korea) was used to calculate the root mean square, record it, and save the data automatically. Before the recording, skin preparation to reduce impedance was conducted by a licensed physiotherapist by initially cleaning the recording skin surface with 70% alcohol wipes to ensure that the skin was clean.

Table 1.
Positions of the electromyography electrodes.
A manual resistance test by the same investigator was conducted to measure the baseline EMG data for the maximal voluntary isometric contraction (MVIC) for each muscle before the exercise. EMG was measured for 10 s twice with a 10 s rest between repetitions and a 2 min rest between each muscle assessment. The highest recorded muscle activity was used for normalization. The procedure of measuring the MVIC for each muscle was adapted from a previous study [26] and is described in Table 2. EMG activity was recorded at 2 weeks and 4 weeks after the exercises were performed, in the same positions for both groups, except that manual resistance was not performed. For participants in the MR group, EMG was recorded while they used the resistance of the pseudo-weight, and those in the control group used the resistance of the dumbbell.
Table 2.
Maximal voluntary isometric contraction measurement settings.
2.8. Statistical Analysis
The Statistical Package for Social Sciences (SPSS) software ver. 29.0 for Windows (SPSS Inc, Chicago, IL, USA) was used for the analysis of the results. Descriptive statistics were recorded to analyze the demographic characteristics of participants and the baseline MVIC values of all muscles from both groups. Data are presented as mean ± standard deviation. The baseline MVIC value was used to ensure that both groups had a non-significant difference in muscle activation before the exercises. Since muscle activations in the two conditions (pseudo-weight and real dumbbell) were the main outcome targets, we conducted a paired-sample t-test to make a direct comparison of the muscle activation changes over time (between the pre-and post-intervention measurements) and an independent-sample t-test to compare the difference between the groups. The significance level was set at p < 0.05.
3. Results
3.1. Demographic Characteristics
The thirty-two participants in this study all completed the training program and attended all intervention sessions. By the end of the study, none of the participants had dropped out. The general characteristics of both groups of participants are displayed in Table 3. There were no significant differences between the two groups in terms of general characteristics.
Table 3.
General characteristics of the participants and baseline muscle activation.
3.2. Muscle Activation
The within-group comparisons for muscle activation showed statistically significant differences in some muscles in both groups. First, in the MR group, the paired-sample t-test showed a statistically significant difference between the pre-test and post-test in the middle deltoid (p = 0.024), upper trapezius (p = 0.013), and supraspinatus (p = 0.011). Despite an increase in mean value from the pre-test to the post-test in the anterior deltoid, posterior deltoid, and infraspinatus, no statistically significant difference was observed (p > 0.05). In the control group, there were statistically significant differences in the anterior deltoid (p = 0.014), middle deltoid (p = 0.014), upper trapezius (p = 0.023), and supraspinatus (p = 0.021). However, the posterior deltoid and infraspinatus did not show a significant difference (p > 0.05), although an increase in mean value was observed between the pre-test and post-test.
Second, the independent-sample t-test used to compare the differences between the two groups showed no statistical difference in muscle activation for any of the six muscles (p > 0.05). The mean and standard deviation differences for the within-group comparison (pre-test and post-test comparison) are presented in Table 4, and the between-group comparison values are presented in Table 5. The baseline MVIC values are displayed as a reference for participants’ muscle contraction but were not used in the analysis of the muscle activity changes in either group since the measurement method was different.
Table 4.
Comparison of muscle activation within groups.
Table 5.
Comparison of muscle activation between groups.
Finally, regarding the survey, only participants in the MR group were asked to complete it and the results are presented in Table 6. Although all participants reported no pain during or after the use of the MR Glasses, some reported having visual fatigue during and after wearing the device. Ten of the sixteen participants affirmed that the device was comfortable, and fourteen of them were favorable to using it for long-term training programs. In addition, the majority of participants reported no loss of balance, and no loss of the notion of time was observed in any participants. Some of them reported not to have felt the real environment surrounding them while wearing the MR Glasses. However, no accident, injury, or adverse effect was noticed.
Table 6.
Survey on the use of MR Glasses.
4. Discussion
The purpose of the present study was to investigate the feasibility and effectiveness of a pseudo-weight resistance training program using an MR Glass (HoloLens) device on shoulder muscle activation in healthy adults. Our results show that training with a pseudo-weight while wearing the MR Glasses effectively affected the activity of some muscles tested. Although an increase in muscle activation was observed in the anterior deltoid, middle deltoid, and supraspinatus, mean muscle activation was comparatively lower than in the control group. Additionally, while no statistically significant difference was observed between the MR group and the control group, training using a pseudo-weight with the MR Glasses produced less muscle activation both before and after the training compared with their baseline MVIC.
In our experiment, participants repeated various shoulder movements, including flexion, extension, adduction, and abduction in a rhythmic and steady sequence. Thus, we can postulate that participants’ motivation and degree of immersion during the performance of the exercises were greater in the MR group compared with the exercise performed using physical weights in the control group. However, our findings showed that all muscle activities in the MR group were lower than those in the control group. This can be explained by the fact that using the pseudo-weight with the avatar in some way reduced the haptic sense of weight, and the amount of muscle activity became lower due to the lack of physical contact with the real world.
Additionally, low muscle activation in the MR group in the present study may be due to limited realistic weight recognition, as this completely relied on visual perception of the weighted dumbbells. This explanation is supported by a previous study conducted by Hummel et al. [27] who affirmed that weight recognition during exergames in VR or AR environments is an essential factor that contributes to a more realistic interaction with virtual objects, which may directly influence muscle activation. Contrary to previous studies that used the vibration of electric muscle stimulators or controllers [28,29], our approach used visual information and a hand-tracking algorithm to manipulate weighted dumbbells.
In terms of resistance exercise, it has been reported that physiological responses to resistance appear generally in the nervous system, which plays a crucial role in the initial contraction and adaptation of muscles [30,31]. It is possible to increase muscle activation using physical weights without visible changes in the muscle, placing emphasis on the haptic effect of weight resistance. Although using MR Glasses with pseudo-weights provides a realistic effect of weight exercise, its impact on weight perception and neuronal activity may be limited without real haptic perception.
In a previous study, Conwit et al. [32] affirmed that when resistance was maintained steadily and then increased during the training period, it resulted in muscle adaptation and high potential action in the motor unit. In our study, we used a steady resistance load for both the MR group and the control group. However, the force of the hand grip at the wrist and the implication of the elbow joint may be another major reason for the difference in muscle activation level between the two groups.
Interestingly, no significant difference was observed between the real dumbbell resistance exercise and the pseudo-weight exercise. This may be related to the fact that visual stimuli, or visual feedback, affect the neuromuscular system. Several studies have demonstrated that visual stimuli enhance the activation of muscles and that different stimuli may have different effects on muscles [33,34,35]. It is important to mention that multiple types of sensory information are transmitted to the brain, which integrates them and stimulates voluntary muscle contraction. Consistent with this mechanism, the visual perception of weight created by the pseudo-weight system on the MR Glass certainly provides sensory information to brain neurons, resulting in muscle activation that was not significantly different from real resistance training.
The present study has some limitations that need to be acknowledged. First, the present study was a preliminary study conducted on participants without any muscular impairments or disorders, and only one outcome was measured (muscle activation). The results of this study should be interpreted carefully and should be replicated using various exercises and outcome measurements, with more participants to increase statistical power. Second, the exercises were performed with an MR Glass (HoloLens MR device), implying that the result may only be related to this specific head-mounted device. Third, we used specific exercises during the experiment, and they were selected to allow replication. However, some tasks, such as climbing, could include a high risk of fall and injury and could have yielded different muscular activity demands that could have consequently altered some muscles. Fourth, using a Likert scale for the questionnaire would have been better to collect the data. However, we choose to use a yes-or-no format to minimize response bias and create a less complex questionnaire, since it has been found that both questionnaire formats are equally reliable [36].
5. Conclusions
The present study aimed to assess the feasibility and effectiveness of pseudo-weight training using an MR device on muscle activation in healthy young adults. The main findings were that MR-based pseudo-weight training and physical weight training both resulted in an improvement in some muscles’ activation, while there was no significant difference between the two groups. Moreover, a brief survey showed general satisfaction with the training system, though some participants reported mild discomfort due to the headset fixation. We can conclude that pseudo-weight training using HoloLens MR Glasses appeared to be feasible and potentially effective in increasing muscle activity. However, more research is needed to assess its use in home training early rehabilitation programs.
Author Contributions
Conceptualization, D.M.N. and J.-H.Y.; methodology, D.M.N. and D.-Y.L.; software, J.-H.H. and J.-S.K.; formal analysis, S.-G.K.; investigation, D.M.N. and Y.-G.N.; writing—original draft preparation, D.M.N.; writing—review and editing, D.M.N. and J.-H.Y.; supervision, J.-H.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Culture, Sports and Tourism R&D Program through the Korea Creative Content Agency grant funded by the Ministry of Culture, Sports and Tourism in 2022 (Project No. SR202106002).
Institutional Review Board Statement
This study was conducted following the Declaration of Helsinki and approved by the Institutional Review Board of Sun Moon University (SM-202206-028-2).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study and written informed consent has been obtained from participants to publish this paper.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors thank all participants who participated in the experiments and made the completion of this study possible.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Morimoto, T.; Kobayashi, T.; Hirata, H.; Otani, K.; Sugimoto, M.; Tsukamoto, M.; Yoshihara, T.; Ueno, M.; Mawatari, M. XR (extended reality: Virtual reality, augmented reality, mixed reality) technology in spine medicine: Status quo and quo vadis. J. Clin. Med. 2022, 11, 470. [Google Scholar] [CrossRef] [PubMed]
- Flavián, C.; Ibáñez-Sánchez, S.; Orús, C. The impact of virtual, augmented and mixed reality technologies on the customer experience. J. Bus. Res. 2019, 100, 547–560. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, H.; Kim, Y.O. Virtual reality and augmented reality in plastic surgery: A review. Arch. Plast. Surg. 2017, 44, 179–187. [Google Scholar] [CrossRef]
- Xiong, J.; Hsiang, E.L.; He, Z.; Zhan, T.; Wu, S.T. Augmented reality and virtual reality displays: Emerging technologies and future perspectives. Light Sci. Appl. 2021, 10, 216. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, Q.; Chen, H.; Song, X.; Tang, H.; Tian, M. An overview of augmented reality technology. J. Phys. Conf. Ser. 2019, 1237, 022082. [Google Scholar] [CrossRef]
- Radianti, J.; Majchrzak, T.A.; Fromm, J.; Wohlgenannt, I. A systematic review of immersive virtual reality applications for higher education: Design elements, lessons learned, and research agenda. Comput. Educ. 2020, 147, 103778. [Google Scholar] [CrossRef]
- Denche-Zamorano, A.; Rodriguez-Redondo, Y.; Barrios-Fernandez, S.; Mendoza-Muñoz, M.; Castillo-Paredes, A.; Rojo-Ramos, J.; Garcia-Gordillo, M.A.; Adsuar, J.C. Rehabilitation is the main topic in virtual and augmented reality and physical activity research: A bibliometric analysis. Sensors 2023, 23, 2987. [Google Scholar] [CrossRef]
- Nekar, D.M.; Kang, H.Y.; Yu, J.H. Improvements of physical activity performance and motivation in adult men through augmented reality approach: A randomized controlled trial. J. Environ. Public Health 2022, 2022, 3050424. [Google Scholar] [CrossRef]
- Pasco, D. The potential of using virtual reality technology in physical activity settings. Quest 2013, 65, 429–441. [Google Scholar] [CrossRef]
- Mouatt, B.; Smith, A.E.; Mellow, M.L.; Parfitt, G.; Smith, R.T.; Stanton, T.R. The use of virtual reality to influence motivation, affect, enjoyment, and engagement during exercise: A scoping review. Front. Virtual Real. 2020, 1, 564664. [Google Scholar] [CrossRef]
- Ng, Y.L.; Ma, F.; Ho, F.K.; Ip, P.; Fu, K.W. Effectiveness of virtual and augmented reality-enhanced exercise on physical activity, psychological outcomes, and physical performance: A systematic review and meta-analysis of randomized controlled trials. Comput. Hum. Behav. 2019, 99, 278–291. [Google Scholar] [CrossRef]
- Mori, S.; Kataoka, Y.; Hashiguchi, S. Exploring pseudo-weight in augmented reality extended displays. In Proceedings of the IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Christchurch, New Zealand, 12 March 2022; pp. 703–710. [Google Scholar]
- Borst, C.W.; Indugula, A. Realistic virtual grasping. In Proceedings of the IEEE Virtual Reality, Bonn, Germany, 12–16 March 2005; pp. 91–98. [Google Scholar]
- Moosavi, M.S.; Raimbaud, P.; Guillet, C.; Plouzeau, J.; Merienne, F. Weight perception analysis using pseudo-haptic feedback based on physical work evaluation. Front. Virtual Real. 2023, 4, 973083. [Google Scholar] [CrossRef]
- Ujitoko, Y.; Ban, Y. Survey of pseudo-haptics: Haptic feedback design and application proposals. IEEE Trans. Haptics 2021, 14, 699–711. [Google Scholar] [CrossRef] [PubMed]
- Stapleton, C.B.; Hughes, C.E.; Moshell, J.M. Mixed reality and the interactive imagination. In Proceedings of the 1st Swedish–American Workshop on Modeling and Simulation, Orlando, FL, USA, 30 October 2002; Volume 1, pp. 30–31. [Google Scholar]
- Park, S.J. A VR-based pseudo weight algorithm using machine learning. J. Korea Soc. Comput. Inf. 2021, 26, 53–59. [Google Scholar]
- Moore, D.R.; Burgomaster, K.A.; Schofield, L.M.; Gibala, M.J.; Sale, D.G.; Phillips, S.M. Neuromuscular adaptations in human muscle following low intensity resistance training with vascular occlusion. Eur. J. Appl. Physiol. 2004, 92, 399–406. [Google Scholar] [CrossRef]
- Johnston, A.P.; De Lisio, M.; Parise, G. Resistance training, sarcopenia, and the mitochondrial theory of aging. Appl. Physiol. Nutr. Metab. 2008, 33, 191–199. [Google Scholar] [CrossRef]
- Behringer, M.; Vom Heede, A.; Yue, Z.; Mester, J. Effects of resistance training in children and adolescents: A meta-analysis. Pediatrics 2010, 126, e1199–e1210. [Google Scholar] [CrossRef]
- Buller, A.J.; Kean, C.J.C.; Ranatunga, K.W. Transformation of contraction speed in muscle following cross-reinnervation; dependence on muscle size. J. Muscle Res. Cell Motil. 1987, 8, 504–516. [Google Scholar] [CrossRef]
- Jung, H.; Seo, J.; Seo, K.; Kim, D.; Park, S. Detection of muscle activation during resistance training using infrared thermal imaging. Sensors 2021, 21, 4505. [Google Scholar] [CrossRef] [PubMed]
- Moseley, J.B., Jr.; Jobe, F.W.; Pink, M.; Perry, J.; Tibone, J. EMG analysis of the scapular muscles during a shoulder rehabilitation program. Am. J. Sports Med. 1992, 20, 128–134. [Google Scholar] [CrossRef]
- Ijiri, T.; Urabe, Y.; Maeda, N.; Sasadai, J.; Suzuki, T. Comparative study of the differences in shoulder muscle activation according to arm rotation angle. Hum. Mov. Sci. 2020, 69, 102567. [Google Scholar] [CrossRef] [PubMed]
- Criswell, E. Cram’s Introduction to Surface Electromyography; Jones & Bartlett Publishers: Burlington, MA, USA, 2010. [Google Scholar]
- Cools, A.M.; Van Tongel, A.; Berckmans, K.; Spanhove, V.; Plaetevoet, T.; Rosseel, J.; Soen, J.; Levy, O.; Maenhout, A. Electromyographic analysis of selected shoulder muscles during a series of exercises commonly used in patients with symptomatic degenerative rotator cuff tears. J. Shoulder Elbow. Surg. 2020, 29, e361–e373. [Google Scholar] [CrossRef]
- Hummel, J.; Dodiya, J.; Wolff, R.; Gerndt, A.; Kuhlen, T. An evaluation of two simple methods for representing heaviness in immersive virtual environments. In Proceedings of the 2013 IEEE Symposium on 3D User Interfaces (3DUI), Orlando, FL, USA, 16–17 March 2013; pp. 87–94. [Google Scholar]
- Kim, J.; Kim, S.; Lee, J. The Effect of Multisensory Pseudo-Haptic Feedback on Perception of Virtual Weight. IEEE Access 2022, 10, 5129–5140. [Google Scholar] [CrossRef]
- Rietzler, M.; Geiselhart, F.; Gugenheimer, J.; Rukzio, E. Breaking the tracking: Enabling weight perception using perceivable tracking offsets. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems, Online, 19 April 2018; pp. 1–12. [Google Scholar]
- Fragala, M.S.; Kraemer, W.J.; Denegar, C.R.; Maresh, C.M.; Mastro, A.M.; Volek, J.S. Neuroendocrine-immune interactions and responses to exercise. Sports Med. 2021, 41, 621–639. [Google Scholar] [CrossRef] [PubMed]
- McCall, G.E.; Byrnes, W.C.; Fleck, S.J.; Dickinson, A.; Kraemer, W.J. Acute and chronic hormonal responses to resistance training designed to promote muscle hypertrophy. Can. J. Appl. Physiol. 1999, 24, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Conwit, R.A.; Ling, S.; Roth, S.; Stashuk, D.; Hurley, B.; Ferrell, R.; Metter, E.J. The relationship between ciliary neurotrophic factor (CNTF) genotype and motor unit physiology: Preliminary studies. BMC Physiol. 2005, 5, 15. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Lloyd, D.G.; Lay, B.S.; Bourke, P.D.; Alderson, J.A. Different visual stimuli affect muscle activation at the knee during sidestepping. J. Sports Sci. 2019, 37, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Fanta, O.; Hadraba, D.; Lopot, F.; Kubový, P.; Bouček, J.; Jelen, K. Pre-activation and muscle activity during frontal impact in relation to whiplash associated disorders. Neuro Endocrinol. Lett. 2013, 34, 708–716. [Google Scholar]
- Pak, N.W.; Lee, J.H. Effects of visual feedback training and visual targets on muscle activation, balancing, and walking ability in adults after hemiplegic stroke: A preliminary, randomized, controlled study. Int. J. Rehabil. Res. 2020, 43, 76–81. [Google Scholar] [CrossRef]
- Dolnicar, S.; Grün, B.; Leisch, F. Quick, simple and reliable: Forced binary survey questions. Int. J. Mark. Res. 2011, 53, 231–252. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).