Abstract
Vaccine hesitancy plays a crucial role in worldwide pandemic-control efforts. The multifaceted nature of vaccine hesitancy entails many psychological factors that are widely discussed in the literature, although few studies specifically compile these factors. Thus, this systematic review aims to synthesize the psychological factors contributing to vaccine hesitancy. As per the PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines, a systematic search was conducted on electronic databases PubMed, Scopus, Science Direct, PsycNET, and Web of Science, and a manual search was conducted on Google Scholar. Out of the 2289 articles obtained, 79 studies that met the inclusion criteria were deemed eligible for the review. The findings highlight appraisals of the COVID-19 pandemic, vaccine safety and side effects, vaccine confidence/trust, trust in government and healthcare professionals, scepticism around vaccine production, conspiracy beliefs, emotions, and information and knowledge about the vaccine as the major psychological factors contributing to vaccine hesitancy. Concerningly, misinformation on COVID-19 vaccination spread through social media platforms, increasing vaccine hesitancy. Recommendations for government authorities, healthcare professionals, and implications for future research are also outlined.
1. Introduction
Sporadic outbreaks of contagious diseases have had a significant and long-lasting impact on societies throughout history. Vaccination has emerged as a critical healthcare response to the rising number of communicable diseases infecting the global population [1]. Even though a growing body of evidence reveals that vaccines are safe [2,3], vaccine hesitancy is also on the rise [4]. Vaccine hesitancy alludes to a lag in acceptance or refusal to uptake a vaccine despite the available facilities of vaccination programmes [2]. Further, the Sage Working Group has proposed that attitudes toward vaccination are influenced by three primary categories of variables: convenience, complacency, and confidence. Convenience pertains to vaccination accessibility, complacency refers to infection risk and immunization relevance, and confidence refers to belief in vaccine safety or efficacy [5].
Previous research has indicated vaccination hesitancy as a global issue, with many reasons for vaccine refusal [6,7]. Studies have explored hesitancy in cases of diseases such as polio, pertussis, measles, tetanus [8], influenza [9], and human papillomavirus (HPV) [10]. Perceived risks versus advantages, religious beliefs and a limited awareness were among the most common reasons cited [11,12]. Many studies have demonstrated that unhealthy behaviours influence vaccine acceptance, such as alcohol intake [13,14] and smoking habits [15,16]. There are mixed results regarding physical activity and vaccine uptake. Several studies have reported decreased physical activity as an obstacle to vaccination in some instances [17,18,19] and as a booster in other cases [13,20]. Thus, vaccine hesitancy has been studied through the lens of several cognitive and behavioural factors to date. Negative attitudes to vaccinations have been related to mistrust of authority segments of society, such as government officials, healthcare providers, and scientists [21,22,23,24]. Altogether, the evidence suggests that various psychological factors likely differentiate people who oppose vaccines and those who accept them.
The aforementioned determinants can also be adapted to the current COVID-19 vaccine hesitancy. Individuals who hesitate or refuse to vaccinate are characterized by more self-interest, distrust of specialists and authorities, greater adherence to religious beliefs, and the harbouring of conspiratorial and suspicious beliefs [25]. Moreover, people may use self-protection habits to replace vaccination in mitigating COVID-19. They may presume that conforming to such safety measures is sufficient for preventing infection [26]. This situation could be due to the spread of vaccine-related misinformation within society [27]. Furthermore, strong associations between intent to vaccinate and perceived safety [28], links between a negative attitude toward COVID-19 vaccines and the refusal to vaccinate [29], and the relationship between religiosity and a lesser degree of intent to vaccinate [30] highlight the need to understand the psychological factors contributing to vaccine hesitancy.
Further, many of the available works on vaccine hesitancy identify explicit reasons provided by people for opposing vaccination [9,31,32,33]. Although this knowledge is valuable, it is restricted in its capacity to elucidate why people arrive at their various epistemological positions [34]. Therefore, it may be more insightful to identify the psychological factors that characterize and differentiate individuals who hesitate to take or refuse vaccines from those who are responsive to vaccine programs. Thus, this systematic review aims to synthesise and integrate evidence on psychological factors of vaccine hesitancy in the pandemic context. Such a review can guide interventional programs designed to build and strengthen responses to combat the pandemic threat [35].
2. Methods
The current review was structured as per the updated guidelines for reporting systematic reviews [36].
2.1. Eligibility Criteria
The following inclusion criteria were used. The current review did not limit studies conducted solely among any specific group of participants as the study objective included understanding the psychological factors of vaccine hesitancy among different populations across the world. Studies were included if they investigated psychological factors associated with vaccine hesitancy. The search was limited to the English language. Further, articles were included if they were published from 2019 onward. The review chose this year as the cut-off as the analysis focused on the COVID-19 pandemic. The review excluded conference abstracts, unpublished manuscripts (preprints), commentaries, editorials, and publications that analysed only the secondary data.
2.2. Search Strategy
Online databases of PubMed, Scopus, Science Direct, PsycNET, and Web of Science were systematically examined using a combination of keywords: “cognitive”, “behavioural”, “determinant”, “emotional”, “psychological”, “vaccine hesitancy”, “vaccine refusal”, “vaccine opposition”, “vaccine reactance”, “vaccine resistance”, “vaccine acceptance”, “COVID-19”, and “SARS-CoV-2”. Boolean operators “AND” and “OR” were employed at this time to integrate keywords on each database. An additional literature search was conducted using Google Scholar to identify any other relevant articles.
2.3. Selection Process and Data Extraction
The first author (John Romate) completed the study conceptualization and came up with the search terms and carried out the search. The first three authors (John Romate., E.R. and A.G.) simultaneously screened the articles for the titles and abstracts independently. The identified references obtained through database search were exported to reference management software, Zotero, and then duplicates and retracted studies were removed. Next, the remaining citations were exported to a Microsoft Excel spreadsheet. These studies were screened against the eligibility criteria based on the titles and abstracts. Subsequently, a full-text review was conducted for articles with abstracts that met the eligibility criteria, again by the first three authors. The PRISMA flowchart was adhered to for each phase of article screening. After the full-text review of the studies for eligibility, data extraction was completed by the first two authors. The following data were extracted from each finalized article: author, year of publication, details concerning the country, sample information, and psychological factors.
2.4. Quality Assessment and Evidence Synthesis
The quality assessment of included studies was completed using critical appraisal tools from the Joanna Briggs Institute (JBI) [37]. These tools were scored on a rating scale of ‘yes’, ‘no’, ‘unclear’, and ‘not applicable’ across several study domains. Articles were appraised by the second and third authors (E.R. and A.G.) and a third reviewer decided on any discrepancies (John Romate). A narrative synthesis of extracted evidence was carried out comparing and contrasting the overall data and qualitatively presented as themes. The reviewers reached a consensus on the study findings through frequent discussions.
3. Results
3.1. Identification of Studies
An initial search on five electronic databases yielded 2289 records, of which 748 were from PubMed, 894 from Scopus, 412 from Science Direct, 128 from PsycNET, and 95 from Web of Science. Further, an additional 12 studies were identified via the Google Scholar search. After deduplication and removal of retracted items, the remaining 1562 records were screened for selection based on the inclusion criteria (Figure 1). Subsequently, 1401 records were removed after the title and abstract screening. Of the 161 reports sought for retrieval, the full text was not available for 16 studies. The remaining 145 reports were assessed for eligibility. The full-text analysis excluded 66 reports that were not about the psychological factors of COVID-19 vaccine hesitancy. Thus, the final analysis included 79 quantitative studies on COVID-19 vaccination with an emphasis on the psychological factors associated with vaccine hesitancy.
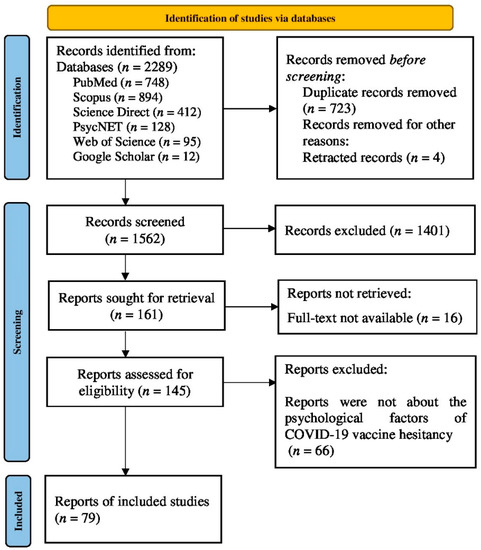
Figure 1.
The PRISMA flow diagram depicting the selection of studies for the systematic review.
3.2. Study Characteristics
Of the 79 studies selected for the final analysis, two were published in 2020, 58 were published in 2021, and the remaining 19 were published in 2022 (Table 1). The included studies were conducted in the United States (US) (n = 10), China (n = 5), UK (n = 4), Saudi Arabia (n = 4), Italy (n = 3), Kuwait (n = 3), India (n = 3), Bangladesh (n = 3), South Korea (n = 3), Jordan (n = 3), Turkey (n = 2), Tunisia (n = 2), Qatar (n = 2), Turkey (n = 2), Thailand (n = 2), Ireland & UK (n = 2), Hong Kong (n = 2), and one study each from Malta, Austria, Canada, Pakistan, Palestine, France, Egypt, Iran, Mexico, Mongolia, Norway, Brazil, UAE, Africa, Ethiopia, Cyprus, Greece, Portugal, Australia, Iraq, Zimbabwe, and Nigeria. Of the remaining two studies, one was conducted across nine low- and middle-income countries and the other was in Jordan, Kuwait, and other Arab countries. The selected studies included those completed prior to COVID-19 vaccine authorization (which analysed the psychological factors of future vaccine hesitancy by assuming that vaccines would be available) and those studies conducted after the authorization of COVID-19 vaccines. All the finalized articles used cross-sectional designs (n = 79). Most of the studies were conducted among the general population (n = 48). Other studies covered healthcare workers, medical students, university students, parents, physicians, mothers with a mental health history, vaccine priority population, adults with multiple sclerosis, nursing students, nurses and midwives, college students, and pregnant and lactating women.

Table 1.
Summary of study characteristics.
3.3. Quality Assessment
The quality assessment of 79 studies included in the current systematic review was conducted using JBI critical appraisal tools. The risk of bias for the assessed studies was generally at a moderate to high level. Moreover, no studies were eliminated based on the level of quality appraisal. The quality assessment results can be found in the supplementary file.
3.4. Psychological Factors Associated with Vaccine Hesitancy
The current review findings provide a comprehensive list of various psychological factors associated with vaccine hesitancy but further suggest such factors could be conceptualized into seven main themes: appraisals of the COVID-19 pandemic, vaccine safety and side effects, general vaccine confidence/trust, trust in government and healthcare professionals, scepticism around vaccine production, conspiracy beliefs, emotions, and information and knowledge about the vaccine (Table 2).
Table 2.
Overview of psychological factors related to vaccine hesitancy.
3.4.1. Appraisal of COVID-19 Pandemic
The literature review clearly evidences the association between appraisals of COVID-19 and vaccine hesitancy. Specifically, vaccine hesitancy was reported more likely among respondents with little to no fear of COVID-19 infection [42,45,46,51,62,69,75]. One study revealed that respondents who considered the vaccination to be unnecessary and with lower perceived danger of COVID-19 with greater vaccine hesitancy showed vaccine complacency [79]. Further, individuals who experienced no symptoms during the pandemic were more likely to report vaccine hesitancy [83]. Thus, participants who more strongly perceived their risk of being infected by COVID-19 as lower demonstrated a higher tendency toward vaccine hesitancy [84]. Similarly, vaccination was accepted by more people who were afraid of COVID-19 than those who were not [105]. Specifically, a study including an Irish and UK sample reported higher fear of COVID-19 among the vaccine accepting groups than those who were vaccine-hesitant [115].
3.4.2. Vaccine Safety and Side Effects
One theme extracted from the investigated studies was that perceptions of the safety and side effects of the COVID-19 vaccine had a greater influence on vaccine hesitancy. Participants’ concerns regarding the safety and efficacy of the COVID-19 vaccine were found in many studies [38,39,41,44,48,49,50,53,57,58,63,71,76,77,78,83,84,85,86,88,89,96,102,104,111,115]. More evidently, the respondents in a reviewed study reported 29 reasons for vaccine hesitancy/rejection, wherein the top reason was safety concerns about vaccines [59]. Moreover, people perceived vaccines as unsafe [94] and believed that vaccines may interfere with the treatment outcome or efficacy of other medical/health conditions [75,81]. Whereas, some individuals were hesitant to uptake the vaccine because of the possible side effects of vaccines, as reported in Refs. [48,53,56,57,58,59,60,63,65,71,75,80,86,88,89,92,93,95,96,97,98,100,101,104,107,114]. Concerns about side effects and the efficacy of the vaccine were perceived as barriers that negatively influence willingness to accept vaccination [39]. The findings revealed that such concerns may range from possible vaccine side effects, beliefs regarding the disease itself, people’s perception of rushing to conduct vaccine trials, profiteering of pharmaceutical companies from vaccines, and preferred dependence on natural immunity. In general, participants who were ready to receive a vaccine against COVID-19 showed lesser concerns when compared to individuals who are hesitant to vaccinate.
3.4.3. Vaccine Confidence/Trust
Individual vaccine confidence/trust in general was found to negatively correlate with COVID-19 vaccine hesitancy. The findings emphasized that respondents with high levels of vaccine confidence or trust in general reported low vaccine hesitancy when compared with those people who had low vaccine trust [42,44]. Several studies reported the association of low confidence in vaccinating against COVID-19 or vaccines in general with vaccine hesitancy [61,65,83,103,105]. Further, mistrust in the vaccine made many individuals unwilling to get vaccinated [42,53,56,98]. Moreover, individuals who were less likely to have received previous vaccines against influenza were less likely to receive a COVID-19 vaccine [38,45]. Previous vaccination behaviour against the flu increased the intention to uptake the vaccine but decreased with an increase in general doubts regarding the vaccine [40]. In one study, participants reported uncertainty and mistrust in vaccines as the most common reason for avoiding COVID-19 vaccination [60].
3.4.4. Trust in Government and Healthcare Professionals
The findings identified medical mistrust as a major cognitive factor influencing vaccine hesitancy during the COVID-19 pandemic. Some of the studies revealed that, during the COVID-19 pandemic, there was widespread medical distrust that made a vast number of people refuse vaccination [25,59,69,72,75,82,115]. Moreover, lack of trust in the government led to vaccine hesitancy by generating concerns about the vaccination information provided by government agencies [25,47,50,62,69,77,84,98,104,108,115]. Specifically, in one study, slightly more than half of the participants lacked trust in the ability of governments and other relevant authorities in ensuring the availability of a safe and effective vaccine [111]. Another study reported that trust in the government or voting behaviour was related to vaccine hesitancy. People who voted for opposition parties or did not even vote were more likely to hesitate than respondents who voted for the governing parties [47]. Further, “anti-vaccine” attitudes were also found to be related with “anti-authority” attitudes [25,46].
3.4.5. Scepticism around Vaccine Production
Expedited vaccine production is reported as a contributing factor to vaccine hesitancy across many studies [59,71,95,100,109]. The individual assumption that vaccines were developed rapidly without reasonable trial duration and with safety issues may result in hesitancy to accept their vaccination to ensure effectiveness [41]. Relatedly, mistrust in vaccine-developing companies [59], pharmaceutical lobbying [82], and policymakers’ and managers’ motivations to recommend the vaccine [83] were also reported as concerns that led people to refuse or delay COVID-19 vaccination. Moreover, less trust in science or scientists [25,61,62] has influenced perceptions of people about vaccination.
3.4.6. Conspiracy Beliefs
The evidence suggested that people who reported vaccine hesitancy were less likely to receive pandemic-related information from sources including healthcare professionals and scientists [46], and their perception of the causes of COVID-19 largely constituted conspiracy theories held by individuals [25,46,54,62,66,67,68,69,72,110]. For instance, participants in one study had a conspiracy belief that COVID-19 has an “artificial origin” [46], whereas another study reported individuals’ belief in a pre-planned pandemic [99]. Further, participants in another study revealed conspiracy beliefs such as the injection of microchips into recipients and infertility related to vaccination, respectively [68]. Relatedly, the findings revealed that people who exhibited vaccine hesitancy reported that they were concerned about misinformation related to the vaccine [54,64,67]. Whereas, addressing misinformation on the COVID-19 vaccine can enhance public confidence in healthcare experts, mitigate the effects of conspiracy beliefs, and motivate individuals to follow COVID-19 preventive measures [69].
3.4.7. Emotions
People’s anxiety about COVID-19 vaccines and their rapid production can result in vaccine hesitancy [46,59,71,95,100,109]. Relatedly, worry that the COVID-19 vaccine might adversely affect their present medical/health condition may make people unlikely to obtain the COVID-19 vaccine [75,81,109]. The findings also revealed that people with less fear of COVID-19 were more likely to exhibit vaccine hesitation [42,45,46,115]. Conversely, the findings from another study suggested that individuals who refused to vaccinate had low levels of anxiety, were less worried about the current pandemic, and found the pandemic to be media hype that induced fear. Moreover, their level of resilience perception was high [69]. Further, individuals who reported fear of injection were more likely to hesitate to accept COVID-19 vaccination than individuals who reported no such fear [43,44,105]. Conversely, concerns of losing loved ones to COVID-19 and worries regarding healthcare system overload were found as positive predictors of willingness to uptake the vaccine [69].
3.4.8. Information and Knowledge about Vaccines
The findings indicated social media platforms as a major source of information on COVID-19 vaccines [57,62,66,68,70,73,76]. Further, individuals who were resistant to vaccination expressed less reliance and trust in authoritative and traditional sources of information [25] and broadcast and print media information [62]. Meanwhile, participants in one study indicated healthcare and social service providers as the most trusted sources of vaccination-related information [62]. Conversely, findings from another study indicated that individuals who reported vaccine hesitancy were less likely to receive pandemic-related information from sources including healthcare professionals and scientists [46]. Moreover, inconsistent information from elected authorities and public health professionals was found to influence vaccine hesitancy [103]. In addition, a lack of correct information on the COVID-19 vaccines acts as a potential barrier to COVID-19 vaccine uptake [38,44,58,60,102]. Besides, individuals who were unaware of the vaccine type authorized in their nations were more likely to exhibit vaccine hesitancy [59]. Furthermore, another study revealed that low levels of knowledge of the preventive measures related to COVID-19 led to vaccine refusal [69].
4. Discussion
Vaccine hesitancy acts as a potential threat to global health and limits the health system’s ability to contain the spread of the virus. The aim of the current systematic review was to integrate available evidence on the psychological factors contributing to vaccine hesitancy. The findings reveal an association of increased risk perception with greater vaccine hesitancy. These findings during the pandemic are consistent with previous studies that have revealed risk perception as a robust predictor of protective health behaviours and prevention intention, which includes vaccine uptake [116]. The findings further indicate that the safety and possible side effects of the COVID-19 vaccine play a crucial role in vaccine hesitancy. Research before the pandemic showed that concerns about safety and side effects of vaccines are among the essential factors influencing decisions to vaccinate, specifically for newly produced vaccines [32,117,118]. Similarly, uncertainty and mistrust in vaccines were the most common reason to avoid vaccination. Individuals with more doubts regarding vaccines in general were less willing to receive vaccination. Moreover, the current review findings are in line with prior studies that reported that those who received vaccination against seasonal flu in 2019 were more likely to vaccinate against new pandemic diseases [119,120]. Although vaccine hesitancy has been characterized as vaccine-specific and context-specific [2], the current review suggests that it is plausible that, the more individuals who had concerns about vaccinations in general, the less likely they were to uptake any type of vaccine [40]. Thus, it is critical to provide information regarding the efficacy, safety, and side effects of COVID-19 vaccines to people [121] considering that the reviewed studies highlight the crucial role of such information in combating vaccine hesitancy [57,58].
The findings further reveal that individuals’ trust in health professionals is associated with their intention to vaccinate. This result was consistent with a study conducted before the pandemic indicating that physician recommendation is strongly correlated with vaccine acceptability among patients [122]. Meanwhile, medical mistrust, which is described as an absence of trust in healthcare professionals, the healthcare system, medical treatments, and the government as a custodian of public health [123,124], is identified as a major cognitive factor influencing vaccine hesitancy during the COVID-19 pandemic. Moreover, rapid development of COVID-19 vaccines resulted in a low willingness to vaccinate. A recent review reveals that mass production of vaccines, equitable distribution of those vaccines over the world, and uncertainty about their long-term efficacy are the main obstacles that could prevent COVID-19 vaccination programmes from being successfully implemented [125]. The findings further show that a lack of trust in vaccine manufacturers, governments, and health care providers can lead to the backing of conspiracy beliefs that can cause a negative impact on public health due to their contribution to vaccine hesitancy. The acceptance of such beliefs could be connected to concerns about the vaccine’s perceived safety and the uncertainty about COVID-19 vaccine benefits; a similar trend was observed in studies on influenza vaccine hesitancy [117,126]. Similarly, individuals susceptible to conspiracy beliefs may ignore the interventions developed by scientists and medical professionals [127]. Thus, the review emphasizes that the healthcare professionals should update the public on vaccine-related information, both verified as well as uncertain information, which, in turn, helps to develop trust in healthcare professionals and authorities.
An earlier study before the current pandemic linked negative emotions with vaccine attitudes and vaccination risk perceptions [128]. The findings on emotions and vaccine hesitancy during the current COVID-19 pandemic also confirmed this trend. Establishing a balance between the pandemic perceptions of individuals and their emotional response to the pandemic was viewed as important as these factors were found to affect vaccination behaviour. The current review identifies the need for including emotionally compelling ideas in vaccine promotion, along with strengthening the credibility and trust in government authorities and experts.
Further, the degree of individual knowledge and information regarding the illness and vaccine are crucial in achieving herd immunity as they influence vaccine uptake. The findings show an increased focus on media platforms, particularly social media, in shaping individual opinion on the COVID-19 pandemic and vaccinations. However, uncritical usage of social media information was more likely to increase vaccine hesitancy. Instant access and wide communication between users when coupled with anonymity provided an immense ability for social media to propagate unvetted and unverified information. For instance, people who exhibited vaccine hesitancy report the need to address misinformation related to the safety of the vaccine [45]. The World Health Organization has also raised an alert on the need to combat the “infodemic”, another form of epidemic that quickly spreads misleading information, fake news, and incorrect scientific claims [129]. Moreover, social media algorithms allowed audiences to follow content that conformed to their views and rejected contrasting views, leading to the formation of communities who subscribe to particular ideologies and opinions [130]. Past outbreaks of SARS, Ebola, and H1N1 have highlighted the pivotal role of health-related information in vaccine acceptance and disease prevention [131]. Thus, the findings stress the importance of credible and reliable information on COVID-19 vaccines to reduce vaccine hesitancy and eradicate misinformation on social media.
5. Implications, Limitations, and Future Recommendations
While the world expects COVID-19 vaccines to protect public health and prevent the collapse of healthcare systems, the current review reveals vaccine hesitancy (and consequent vaccine refusal) as a potential barrier. On the other hand, the findings suggest that psychological factors underlying vaccine hesitancy can be effectively used to design future vaccination campaigns that can deal with vaccine hesitancy. Further, understanding the psychological determinants can provide a suitable direction and knowledge for intervention developments. As the COVID-19 pandemic continues with new variants, achieving herd immunity is the ultimate goal, and, in this context, the findings of the current review can be extremely beneficial toward increasing vaccine acceptance and to prepare for any similar future crises.
The current study concentrated on psychological factors influencing vaccination hesitancy. However, there may be varying degrees of connection between psychological factors and certain vaccinations. However, vaccine-type-based findings were not reported in the current review. Additionally, it is possible that significant distinctions may exist between hesitancy, refusal, and opposition, all of which require future study. Because the studies reviewed were cross-sectional, causal conclusions between psychological factors and vaccination hesitancy require future approaches with greater care. More longitudinal or intervention studies are thus required. Further, the review might have classified each psychological factor by country when identifying the contributing factors to vaccine hesitancy, which would have made it simpler to comprehend the underlying reasons for COVID-19 vaccine hesitancy in each nation. Moreover, the psychological characteristics of vaccine-hesitancy may change over time due to the increasing availability of scientific data on COVID-19 vaccinations. Thus, further studies may be needed to identify and analyse these changes over time. However, the review attempted to provide a comprehensive understanding of the psychological factors of vaccine hesitancy by including articles from 2020 to 2022.
The adverse effect of vaccine hesitancy on the development and implementation of mass vaccination programmes needs to be managed with evidence-based vaccine information and effective and proactive measures to fight misinformation. It is important to assign expert groups of scientists and healthcare professionals to provide accurate and reliable data on vaccination in order to reduce vaccine ambiguity and distrust among the public. Healthcare practitioners need to listen to the public concerns, answer their questions, and counter misinformation. Moreover, social media need to pay considerable attention to misleading information regarding vaccination. Besides, it is crucial to conduct studies on vaccine hesitancy by considering conspiracy theories as the general beliefs of people regarding conspiracy theories can be reflected in their vaccine-related attitudes.
6. Conclusions
Vaccine hesitancy is a major challenge to public health during pandemics. This systematic review focused on the psychological factors of vaccine hesitancy and reported the crucial determinants found to be common across countries and different demographic groups. The most common reason for vaccine hesitancy was its safety and side effects. However, conspiracy beliefs and using social media platforms to spread vaccine-related misinformation have also challenged the acceptance of vaccines worldwide. The lack of adequate vaccine information highlights the need to disseminate high-quality and reliable information to enhance vaccine acceptance and coverage. Extensive vaccination campaigns and educational initiatives are required in concert with vaccination promotion efforts to address the psychological factors contributing to vaccine hesitancy. Thus, the government and healthcare professionals need to focus on various cognitive, behavioural, and emotional characteristics of people to successfully cope with vaccine hesitancy and achieve herd immunity.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/vaccines10111777/s1. Supplementary File S1: PRISMA 2020 checklist; Supplentary File S2: Quality assessment results.
Author Contributions
Conceptualization, J.R. (John Romate); Methodology, formal analysis, data curation and investigation, J.R. (John Romate), E.R. and A.G.; writing—original draft preparation, A.G., J.R. (John Rages), R.L., J.J. and S.B.; Writing—review & editing, J.R. (John Romate), E.R., A.G. and J.A.; Supervision, E.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mesch, G.S.; Schwirian, K.P. Vaccination hesitancy: Fear, trust, and exposure expectancy of an Ebola outbreak. Heliyon 2019, 5, e02016. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Thangaraju, P.; Venkatesan, S. WHO Ten threats to global health in 2019: Antimicrobial resistance. Med. J. 2019, 44, 1150–1151. [Google Scholar] [CrossRef]
- Pang, J.; Wang, M.X.; Ang, I.Y.H.; Tan, S.H.X.; Lewis, R.F.; Chen, J.I.-P.; Gutierrez, R.A.; Gwee, S.X.W.; Chua, P.E.Y.; Yang, Q.; et al. Potential Rapid Diagnostics, Vaccine and Therapeutics for 2019 Novel Coronavirus (2019-nCoV): A Systematic Review. J. Clin. Med. 2020, 9, 623. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dubé, E.; Schuster, M.; MacDonald, N.E.; Wilson, R.; The SAGE Working Group on Vaccine Hesitancy. Measuring vaccine hesitancy: The development of a survey tool. Vaccine 2015, 33, 4165–4175. [Google Scholar] [CrossRef] [PubMed]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting Form data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef]
- Wagner, A.L.; Masters, N.B.; Domek, G.J.; Mathew, J.L.; Sun, X.; Asturias, E.J.; Ren, J.; Huang, Z.; Contreras-Roldan, I.L.; Gebremeskel, B.; et al. Comparisons of Vaccine Hesitancy across Five Low- and Middle-Income Countries. Vaccines 2019, 7, 155. [Google Scholar] [CrossRef]
- Wolfe, R.M.; Sharp, L.K. Anti-vaccinationists past and present. BMJ 2002, 325, 430–432. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.-L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Karafillakis, E.; Larson, H.J. The benefit of the doubt or doubts over benefits? A systematic literature review of perceived risks of vaccines in European populations. Vaccine 2017, 35, 4840–4850. [Google Scholar] [CrossRef]
- Pelčić, G.; Karačić, S.; Mikirtichan, G.L.; Kubar, O.I.; Leavitt, F.J.; Cheng-tek Tai, M.; Morishita, N.; Vuletić, S.; Tomašević, L. Religious exception for vaccination or religious excuses for avoiding vaccination. Croat. Med. J. 2016, 57, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Garcia, R.; Arinezfernandez, M.C.; Garciacarballo, M.; Hernandezbarrera, V.; de Miguel, A.G.; Carrascogarrido, P. Influenza vaccination coverage and related factors among Spanish patients with chronic obstructive pulmonary disease. Vaccine 2005, 23, 3679–3686. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.J.; Cho, S.-I. Influenza Vaccination Coverage among Adults in Korea: 2008–2009 to 2011–2012 Seasons. Int. J. Environ. Res. Public Health 2014, 11, 12162–12173. [Google Scholar] [CrossRef]
- Wada, K.; Smith, D.R. Influenza Vaccination Uptake among the Working Age Population of Japan: Results from a National Cross-Sectional Survey. PLoS ONE 2013, 8, e59272. [Google Scholar] [CrossRef]
- Chiatti, C.; Barbadoro, P.; Lamura, G.; Pennacchietti, L.; Di Stanislao, F.; D’Errico, M.M.; Prospero, E. Influenza vaccine uptake among community-dwelling Italian elderly: Results from a large cross-sectional study. BMC Public Health 2011, 11, 207. [Google Scholar] [CrossRef]
- Pulcini, C.; Massin, S.; Launay, O.; Verger, P. Factors associated with vaccination for hepatitis B, pertussis, seasonal and pandemic influenza among French general practitioners: A 2010 survey. Vaccine 2013, 31, 3943–3949. [Google Scholar] [CrossRef]
- Takayama, M.; Wetmore, C.M.; Mokdad, A.H. Characteristics associated with the uptake of influenza vaccination among adults in the United States. Prev. Med. 2012, 54, 358–362. [Google Scholar] [CrossRef]
- Damiani, G.; Federico, B.; Visca, M.; Agostini, F.; Ricciardi, W. The impact of socioeconomic level on influenza vaccination among Italian adults and elderly: A cross-sectional study. Prev. Med. 2007, 45, 373–379. [Google Scholar] [CrossRef]
- Schmitz, H.; Wübker, A. What determines influenza vaccination take-up of elderly Europeans? Health Econ. 2011, 20, 1281–1297. [Google Scholar] [CrossRef]
- Jamison, A.M.; Quinn, S.C.; Freimuth, V.S. “You don’t trust a government vaccine”: Narratives of institutional trust and influenza vaccination among African American and white adults. Soc. Sci. Med. 2018, 221, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Nihlén Fahlquist, J. Vaccine hesitancy and trust. Ethical aspects of risk communication. Scand. J. Public Health 2017, 46, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Mesch, G.S.; Schwirian, K.P. Confidence in government and vaccination willingness in the USA. Health Promot. Int. 2014, 30, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Suk, J.E.; Lopalco, P.; Celentano, L. Hesitancy, Trust and Individualism in Vaccination Decision-Making. PLoS Curr. 2015, 7. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, L.; Jin, H.; Lin, L. Vaccination against COVID-19: A systematic review and meta-analysis of acceptability and its predictors. Prev. Med. 2021, 150, 106694. [Google Scholar] [CrossRef]
- Wake, A.D. The Willingness to Receive COVID-19 Vaccine and Its Associated Factors: “Vaccination Refusal Could Prolong the War of This Pandemic”—A Systematic Review. Risk Manag. Health Policy 2021, 14, 2609–2623. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Soveri, A.; Lewandowsky, S.; Karlsson, L.; Karlsson, H.; Nolvi, S.; Karukivi, M.; Lindfelt, M.; Antfolk, J. Fearing the disease or the vaccine: The case of COVID-19. Pers. Individ. Differ. 2021, 172, 110590. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Olagoke, A.A.; Olagoke, O.O.; Hughes, A.M. Intention to Vaccinate Against the Novel 2019 Coronavirus Disease: The Role of Health Locus of Control and Religiosity. J. Relig. Health 2020, 60, 65–80. [Google Scholar] [CrossRef]
- Siddiqui, M.; Salmon, D.A.; Omer, S.B. Epidemiology of vaccine hesitancy in the United States. Hum. Vaccines Immunother. 2013, 9, 2643–2648. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Marti, M.; de Cola, M.; Macdonald, N.E.; Dumolard, L.; Duclos, P. Assessments of global drivers of vaccine hesitancy in 2014—Looking beyond safety concerns. PLoS ONE 2017, 12, e0172310. [Google Scholar] [CrossRef] [PubMed]
- Hornsey, M.J.; Harris, E.A.; Fielding, K.S. The psychological roots of anti-vaccination attitudes: A 24-nation investigation. Health Psychol. 2018, 37, 307–315. [Google Scholar] [CrossRef]
- de Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Tufanaru, C.; Qureshi, R.; Mattis, P.; Mu, P. Conducting systematic reviews of association (etiology): The Joanna Briggs Institute’s Approach. Int. J. Evid. Based Health 2015, 13, 163–169. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of U.S. adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Caserotti, M.; Girardi, P.; Rubaltelli, E.; Tasso, A.; Lotto, L.; Gavaruzzi, T. Associations of COVID-19 risk perception with vaccine hesitancy over time for Italian residents. Soc. Sci. Med. 2021, 272, 113688. [Google Scholar] [CrossRef]
- Alqudeimat, Y.; Alenezi, D.; AlHajri, B.; Alfouzan, H.; Almokhaizeem, Z.; Altamimi, S.; Almansouri, W.; Alzalzalah, S.; Ziyab, A.H. Acceptance of a COVID-19 Vaccine and Its Related Determinants among the General Adult Population in Kuwait. Med Princ. Pract. 2021, 30, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Willis, D.E.; Andersen, J.A.; Bryant-Moore, K.; Selig, J.P.; Long, C.R.; Felix, H.C.; Curran, G.M.; McElfish, P.A. COVID-19 vaccine hesitancy: Race/ethnicity, trust, and fear. Clin. Transl. Sci. 2021, 14, 2200–2207. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Cordina, M.; Lauri, M.A.; Lauri, J. Attitudes towards COVID-19 vaccination, vaccine hesitancy and intention to take the vaccine. Pharm. Pract. 2021, 19, 2317. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Dobalian, A.; Ward, K.D. COVID-19 Vaccine Hesitancy and Its Determinants Among Adults with a History of Tobacco or Marijuana Use. J. Community Health 2021, 46, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Nazlı, Ş.B.; Yığman, F.; Sevindik, M.; Deniz Özturan, D. Psychological factors affecting COVID-19 vaccine hesitancy. Ir. J. Med. Sci. 2021, 191, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Schernhammer, E.; Weitzer, J.; Laubichler, M.D.; Birmann, B.M.; Bertau, M.; Zenk, L.; Caniglia, G.; Jäger, C.C.; Steiner, G. Correlates of COVID-19 vaccine hesitancy in Austria: Trust and the government. J. Public Health 2021, 44, e106. [Google Scholar] [CrossRef] [PubMed]
- Altulahi, N.; AlNujaim, S.; Alabdulqader, A.; Alkharashi, A.; AlMalki, A.; AlSiari, F.; Bashawri, Y.; Alsubaie, S.; AlShahrani, D.; AlGoraini, Y. Willingness, beliefs, and barriers regarding the COVID-19 vaccine in Saudi Arabia: A multiregional cross-sectional study. BMC Fam. Pract. 2021, 22, 247. [Google Scholar] [CrossRef]
- Aloweidi, A.; Bsisu, I.; Suleiman, A.; Abu-Halaweh, S.; Almustafa, M.; Aqel, M.; Amro, A.; Radwan, N.; Assaf, D.; Abdullah, M.Z.; et al. Hesitancy towards COVID-19 Vaccines: An Analytical Cross–Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5111. [Google Scholar] [CrossRef]
- Benham, J.L.; Atabati, O.; Oxoby, R.J.; Mourali, M.; Shaffer, B.; Sheikh, H.; Boucher, J.-C.; Constantinescu, C.; Parsons Leigh, J.; Ivers, N.M.; et al. COVID-19 Vaccine–Related Attitudes and Beliefs in Canada: National Cross-sectional Survey and Cluster Analysis. JMIR Public Health Surveill. 2021, 7, e30424. [Google Scholar] [CrossRef]
- Chaudhary, F.A.; Ahmad, B.; Khalid, M.D.; Fazal, A.; Javaid, M.M.; Butt, D.Q. Factors influencing COVID-19 vaccine hesitancy and acceptance among the Pakistani population. Hum. Vaccines Immunother. 2021, 17, 3365–3370. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Li, X.; Gao, J.; Liu, X.; Mao, Y.; Wang, R.; Zheng, P.; Xiao, Q.; Jia, Y.; Fu, H.; et al. Health Belief Model Perspective on the Control of COVID-19 Vaccine Hesitancy and the Promotion of Vaccination in China: Web-Based Cross-sectional Study. J. Med. Internet Res. 2021, 23, e29329. [Google Scholar] [CrossRef] [PubMed]
- Danabal, K.G.M.; Magesh, S.S.; Saravanan, S.; Gopichandran, V. Attitude towards COVID 19 vaccines and vaccine hesitancy in urban and rural communities in Tamil Nadu, India—A community based survey. BMC Health Serv. Res. 2021, 21, 994. [Google Scholar] [CrossRef]
- Hossain, M.B.; Alam, M.Z.; Islam, M.S.; Sultan, S.; Faysal, M.M.; Rima, S.; Hossain, A.; Al Mamun, A.A. Health Belief Model, Theory of Planned Behavior, or Psychological Antecedents: What Predicts COVID-19 Vaccine Hesitancy Better Among the Bangladeshi Adults? Front. Public Health 2021, 9, 711066. [Google Scholar] [CrossRef]
- Hossain, E.; Islam, S.; Ghose, T.K.; Jahan, H.; Chakrobortty, S.; Hossen, M.S.; Ema, N.S. COVID-19 vaccine acceptability among public university students in Bangladesh: Highlighting knowledge, perceptions, and attitude. Hum. Vaccines Immunother. 2021, 17, 5089–5098. [Google Scholar] [CrossRef] [PubMed]
- Ikiışık, H.; Akif Sezerol, M.; Taşçı, Y.; Maral, I. COVID-19 vaccine hesitancy: A community-based research in Turkey. Int. J. Clin. Pract. 2021, 75, e14336. [Google Scholar] [CrossRef]
- Alabdulla, M.; Reagu, S.M.; Al-Khal, A.; Elzain, M.; Jones, R.M. COVID-19 vaccine hesitancy and attitudes in Qatar: A national cross-sectional survey of a migrant-majority population. Influenza Other Respir. Viruses 2021, 15, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A.E. Vaccine hesitancy: Beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef] [PubMed]
- Qunaibi, E.; Basheti, I.; Soudy, M.; Sultan, I. Hesitancy of Arab Healthcare Workers towards COVID-19 Vaccination: A Large-Scale Multinational Study. Vaccines 2021, 9, 446. [Google Scholar] [CrossRef]
- Asadi Faezi, N.; Gholizadeh, P.; Sanogo, M.; Oumarou, A.; Mohamed, M.N.; Cissoko, Y.; Saliou Sow, M.; Keita, B.S.; Baye, Y.A.M.; Pagliano, P.; et al. Peoples’ attitude toward COVID-19 vaccine, acceptance, and social trust among African and Middle East countries. Health Promot. Perspect. 2021, 11, 171–178. [Google Scholar] [CrossRef]
- Milan, S.; Dáu, A.L.B.T. The Role of Trauma in Mothers’ COVID-19 Vaccine Beliefs and Intentions. J. Pediatr. Psychol. 2021, 46, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Allington, D.; McAndrew, S.; Moxham-Hall, V.; Duffy, B. Coronavirus conspiracy suspicions, general vaccine attitudes, trust and coronavirus information source as predictors of vaccine hesitancy among UK residents during the COVID-19 pandemic. Psychol. Med. 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zhang, R.; Zhou, Z.; Fan, J.; Liang, J.; Cai, L.; Peng, L.; Ren, F.; Lin, W. Parental psychological distress and attitudes towards COVID-19 vaccination: A cross-sectional survey in Shenzhen, China. J. Affect. Disord. 2021, 292, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Castañeda-Vasquez, D.E.; Ruiz-Padilla, J.P.; Botello-Hernandez, E. Vaccine Hesitancy against SARS-CoV-2 in Health Personnel of Northeastern Mexico and its Determinants. J. Occup. Environ. Med. 2021, 63, 633–637. [Google Scholar] [CrossRef]
- Bono, S.A.; Faria de Moura Villela, E.; Siau, C.S.; Chen, W.S.; Pengpid, S.; Hasan, M.T.; Sessou, P.; Ditekemena, J.D.; Amodan, B.O.; Hosseinipour, M.C.; et al. Factors Affecting COVID-19 Vaccine Acceptance: An International Survey among Low- and Middle-Income Countries. Vaccines 2021, 9, 515. [Google Scholar] [CrossRef]
- Al-Sanafi, M.; Sallam, M. Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales. Vaccines 2021, 9, 701. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Hasan, H.; Taim, D.; Al-Mahzoum, K.; Al-Haidar, A.; Yaseen, A.; Ababneh, N.A.; Assaf, A.; et al. Low COVID-19 Vaccine Acceptance Is Correlated with Conspiracy Beliefs among University Students in Jordan. Int. J. Environ. Res. Public Health 2021, 18, 2407. [Google Scholar] [CrossRef]
- Kucukkarapinar, M.; Karadag, F.; Budakoglu, I.; Aslan, S.; Ucar, O.; Yay, A.; Timurcin, U.; Tumkaya, S.; Hocaoglu, C.; Kiraz, I. COVID-19 Vaccine Hesitancy and Its Relationship with Illness Risk Perceptions, Affect, Worry, and Public Trust: An Online Serial Cross-Sectional Survey from Turkey. Psychiatry Clin. Psychopharmacol. 2021, 31, 98–109. [Google Scholar] [CrossRef]
- Piltch-Loeb, R.; Savoia, E.; Goldberg, B.; Hughes, B.; Verhey, T.; Kayyem, J.; Miller-Idriss, C.; Testa, M. Examining the effect of information channel on COVID-19 vaccine acceptance. PLoS ONE 2021, 16, e0251095. [Google Scholar] [CrossRef]
- Alibrahim, J.; Awad, A. COVID-19 Vaccine Hesitancy among the Public in Kuwait: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 8836. [Google Scholar] [CrossRef] [PubMed]
- Acar-Burkay, S.; Cristian, D.-C. Cognitive underpinnings of COVID-19 vaccine hesitancy. Soc. Sci. Med. 2022, 301, 114911. [Google Scholar] [CrossRef] [PubMed]
- Dambadarjaa, D.; Altankhuyag, G.-E.; Chandaga, U.; Khuyag, S.-O.; Batkhorol, B.; Khaidav, N.; Dulamsuren, O.; Gombodorj, N.; Dorjsuren, A.; Singh, P.; et al. Factors Associated with COVID-19 Vaccine Hesitancy in Mongolia: A Web-Based Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 12903. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, O.V.; Johnson, M.S.; Ebling, S.; Amundsen, O.M.; Halsøy, Ø.; Hoffart, A.; Skjerdingstad, N.; Johnson, S.U. Risk, Trust, and Flawed Assumptions: Vaccine Hesitancy During the COVID-19 Pandemic. Front. Public Health 2021, 9, 700213. [Google Scholar] [CrossRef] [PubMed]
- Ehde, D.M.; Roberts, M.K.; Humbert, A.T.; Herring, T.E.; Alschuler, K.N. COVID-19 vaccine hesitancy in adults with multiple sclerosis in the United States: A follow up survey during the initial vaccine rollout in 2011. Mult. Scler. Relat. Disord. 2021, 54, 103163. [Google Scholar] [CrossRef] [PubMed]
- Almaghaslah, D.; Alsayari, A.; Kandasamy, G.; Vasudevan, R. COVID-19 Vaccine Hesitancy among Young Adults in Saudi Arabia: A Cross-Sectional Web-Based Study. Vaccines 2021, 9, 330. [Google Scholar] [CrossRef]
- Jain, J.; Saurabh, S.; Kumar, P.; Verma, M.K.; Goel, A.D.; Gupta, M.K.; Bhardwaj, P.; Raghav, P.R. COVID-19 vaccine hesitancy among medical students in India. Epidemiol. Infect 2021, 149, e132. [Google Scholar] [CrossRef]
- Kumar, R.; Alabdulla, M.; Elhassan, N.M.; Reagu, S.M. Qatar Healthcare Workers’ COVID-19 Vaccine Hesitancy and Attitudes: A National Cross-Sectional Survey. Front. Public Health 2021, 9, 727748. [Google Scholar] [CrossRef]
- Luk, T.T.; Zhao, S.; Wu, Y.; Wong, J.Y.-H.; Wang, M.P.; Lam, T.H. Prevalence and determinants of SARS-CoV-2 vaccine hesitancy in Hong Kong: A population-based survey. Vaccine 2021, 39, 3602–3607. [Google Scholar] [CrossRef]
- Maraqa, B.; Nazzal, Z.; Rabi, R.; Sarhan, N.; Al-Shakhra, K.; Al-Kaila, M. COVID-19 vaccine hesitancy among health care workers in Palestine: A call for action. Prev. Med. 2021, 149, 106618. [Google Scholar] [CrossRef]
- Mejri, N.; Berrazega, Y.; Ouertani, E.; Rachdi, H.; Bohli, M.; Kochbati, L.; Boussen, H. Understanding COVID-19 vaccine hesitancy and resistance: Another challenge in cancer patients. Support. Care Cancer 2021, 30, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Navarre, C.; Roy, P.; Ledochowski, S.; Fabre, M.; Esparcieux, A.; Issartel, B.; Dutertre, M.; Blanc-Gruyelle, A.-L.; Suy, F.; Adelaide, L.; et al. Determinants of COVID-19 vaccine hesitancy in French hospitals. Infect Dis. Now 2021, 51, 647–653. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, B.L.C.A.; Campos, M.A.G.; de Queiroz, R.C.S.; de Alves, M.T.S.S.B.E.; de Souza, B.F.; dos Santos, A.M.; da Silva, A.A.M. Prevalence and factors associated with covid-19 vaccine hesitancy in Maranhão, Brazil. Rev. Saude Publica 2021, 55, 12. [Google Scholar] [CrossRef]
- Park, H.K.; Ham, J.H.; Jang, D.H.; Lee, J.Y.; Jang, W.M. Political Ideologies, Government Trust, and COVID-19 Vaccine Hesitancy in South Korea: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 10655. [Google Scholar] [CrossRef] [PubMed]
- Sethi, S.; Kumar, A.; Mandal, A.; Shaikh, M.; Hall, C.A.; Kirk, J.M.W.; Moss, P.; Brookes, M.J.; Basu, S. The UPTAKE study: A cross-sectional survey examining the insights and beliefs of the UK population on COVID-19 vaccine uptake and hesitancy. BMJ Open 2021, 11, e048856. [Google Scholar] [PubMed]
- Sirikalyanpaiboon, M.; Ousirimaneechai, K.; Phannajit, J.; Pitisuttithum, P.; Jantarabenjakul, W.; Chaiteerakij, R.; Paitoonpong, L. COVID-19 vaccine acceptance, hesitancy, and determinants among physicians in a university-based teaching hospital in Thailand. BMC Infect Dis. 2021, 21, 1174. [Google Scholar] [CrossRef]
- Yahia, A.I.O.; Alshahrani, A.M.; Alsulmi, W.G.H.; Alqarni, M.M.M.; Abdulrahim, T.K.A.; Heba, W.F.H.; Alqarni, T.A.A.; Alharthi, K.A.Z.; Buhran, A.A.A. Determinants of COVID-19 vaccine acceptance and hesitancy: A cross-sectional study in Saudi Arabia. Hum. Vaccines Immunother. 2021, 17, 4015–4020. [Google Scholar] [CrossRef]
- Yeşiltepe, A.; Aslan, S.; Bulbuloglu, S. Investigation of perceived fear of COVID-19 and vaccine hesitancy in nursing students. Hum. Vaccines Immunother. 2021, 17, 5030–5037. [Google Scholar] [CrossRef]
- Albahri, A.H.; Alnaqbi, S.A.; Alshaali, A.O.; Alnaqbi, S.A.; Shahdoor, S.M. COVID-19 Vaccine Acceptance in a Sample from the United Arab Emirates General Adult Population: A Cross-Sectional Survey. Front. Public Health 2021, 9, 614499. [Google Scholar] [CrossRef]
- Singh, A.; Lai, A.H.Y.; Wang, J.; Asim, S.; Chan, P.S.-F.; Wang, Z.; Yeoh, E.K. Multilevel Determinants of COVID-19 Vaccine Uptake Among South Asian Ethnic Minorities in Hong Kong: Cross-sectional Web-Based Survey. JMIR Public Health Surveill. 2021, 7, e31707. [Google Scholar] [CrossRef]
- Ali, M.; Hossain, A. What is the extent of COVID-19 vaccine hesitancy in Bangladesh? A cross-sectional rapid national survey. BMJ Open 2021, 11, e050303. [Google Scholar] [CrossRef] [PubMed]
- Anjorin, A.A.; Odetokun, I.A.; Abioye, A.I.; Elnadi, H.; Umoren, M.V.; Damaris, B.F.; Eyedo, J.; Umar, H.I.; Nyandwi, J.B.; Abdalla, M.M.; et al. Will Africans take COVID-19 vaccination? PLoS ONE 2021, 16, e0260575. [Google Scholar] [CrossRef] [PubMed]
- Boon-Itt, S.; Rompho, N.; Jiarnkamolchurn, S.; Skunkan, Y. Interaction between age and health conditions in the intention to be vaccinated against COVID-19 in Thailand. Hum. Vaccines Immunother. 2021, 17, 4816–4822. [Google Scholar] [CrossRef]
- Yilma, D.; Mohammed, R.; Abdela, S.G.; Enbiale, W.; Seifu, F.; Pareyn, M.; Liesenborghs, L.; van Griensven, J.; van Henten, S. COVID-19 vaccine acceptability among healthcare workers in Ethiopia: Do we practice what we preach? Trop. Med. Int. Health 2022, 27, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Fakonti, G.; Kyprianidou, M.; Toumbis, G.; Giannakou, K. Attitudes and Acceptance of COVID-19 Vaccination among Nurses and Midwives in Cyprus: A Cross-Sectional Survey. Front. Public Health 2021, 9, 656138. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zheng, Y.; Luo, Y.; Ren, J.; Jiang, L.; Tang, J.; Yu, X.; Luo, D.; Fan, D.; Chen, Y. Hesitancy toward COVID-19 vaccines among medical students in Southwest China: A cross-sectional study. Hum. Vaccines Immunother. 2021, 17, 4021–4027. [Google Scholar] [CrossRef] [PubMed]
- Magadmi, R.M.; Kamel, F.O. Beliefs and barriers associated with COVID-19 vaccination among the general population in Saudi Arabia. BMC Public Health 2021, 21, 1428. [Google Scholar] [CrossRef]
- Khairat, S.; Zou, B.; Adler-Milstein, J. Factors and reasons associated with low COVID-19 vaccine uptake among highly hesitant communities in the US. Am. J. Infect Control. 2022, 50, 262–267. [Google Scholar] [CrossRef]
- Holeva, V.; Parlapani, E.; Nikopoulou, V.; Nouskas, I.; Diakogiannis, I. COVID-19 vaccine hesitancy in a sample of Greek adults. Psychol. Health Med. 2021, 27, 113–119. [Google Scholar] [CrossRef]
- Hubach, R.D.; Shannon, B.; Morgan, K.D.; Alexander, C.; O’Neil, A.M.; Ernst, C.; Giano, Z. COVID-19 vaccine hesitancy among rural Oklahomans. Rural Remote Health 2022, 22, 7128. [Google Scholar] [CrossRef]
- Moro, G.L.; Cugudda, E.; Bert, F.; Raco, I.; Siliquini, R. Vaccine Hesitancy and Fear of COVID-19 Among Italian Medical Students: A Cross-Sectional Study. J. Community Health 2022, 47, 475–483. [Google Scholar] [CrossRef]
- Silva, T.M.; Estrela, M.; Roque, V.; Gomes, E.R.; Figueiras, A.; Roque, F.; Herdeiro, M.T. Perceptions, knowledge and attitudes about COVID-19 vaccine hesitancy in older Portuguese adults. Age Ageing 2022, 51, afac013. [Google Scholar] [CrossRef] [PubMed]
- Soares, P.; Rocha, J.; Moniz, M.; Gama, A.; Laires, P.; Pedro, A.; Dias, S.; Leite, A.; Nunes, C. Factors Associated with COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, A.; Dickinson, H.; Dimov, S.; Shields, M.; McAllister, A. The COVID-19 vaccine intentions of Australian disability support workers. Aust. NZ J. Public Health 2022, 46, 314–321. [Google Scholar] [CrossRef]
- Hwang, S.E.; Kim, W.-H.; Heo, J. Socio-demographic, psychological, and experiential predictors of COVID-19 vaccine hesitancy in South Korea, October-December. Hum. Vaccines Immunother. 2021, 18, 1–8. [Google Scholar] [CrossRef]
- Hong, J.; Xu, X.-W.; Yang, J.; Zheng, J.; Dai, S.-M.; Zhou, J.; Zhang, Q.-M.; Ruan, Y.; Ling, C.-Q. Knowledge about, attitude and acceptance towards, and predictors of intention to receive the COVID-19 vaccine among cancer patients in Eastern China: A cross-sectional survey. J. Integr. Med. 2021, 20, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Shareef, L.G.; Fawzi Al-Hussainy, A.; Majeed Hameed, S. COVID-19 vaccination hesitancy among Iraqi general population between beliefs and barriers: An observational study. F1000Research 2022, 11, 334. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; You, M. Direct and Indirect Associations of Media Use With COVID-19 Vaccine Hesitancy in South Korea: Cross-sectional Web-Based Survey. J. Med. Internet Res. 2022, 24, e32329. [Google Scholar] [CrossRef]
- Kumari, A.; Mahey, R.; Kachhawa, G.; Kumari, R.; Bhatla, N. Knowledge, attitude, perceptions, and concerns of pregnant and lactating women regarding COVID-19 vaccination: A cross-sectional survey of 313 participants from a tertiary care centre of North India. Diabetes Metab. Syndr. Clin. Res. Rev. 2022, 16, 102449. [Google Scholar] [CrossRef]
- Moscardino, U.; Musso, P.; Inguglia, C.; Ceccon, C.; Miconi, D.; Rousseau, C. Sociodemographic and psychological correlates of COVID-19 vaccine hesitancy and resistance in the young adult population in Italy. Vaccine 2022, 40, 2379–2387. [Google Scholar] [CrossRef]
- Mundagowa, P.T.; Tozivepi, S.N.; Chiyaka, E.T.; Mukora-Mutseyekwa, F.; Makurumidze, R. Assessment of COVID-19 vaccine hesitancy among Zimbabweans: A rapid national survey. PLoS ONE 2022, 17, e0266724. [Google Scholar] [CrossRef] [PubMed]
- Zammit, N.; Gueder, A.E.; Brahem, A.; Ayouni, I.; Ghammam, R.; Fredj, S.B.; Sridi, C.; Chouchene, A.; Kalboussi, H.; El Maalel, O.; et al. Studying SARS-CoV-2 vaccine hesitancy among health professionals in Tunisia. BMC Health Serv. Res. 2022, 22, 489. [Google Scholar] [CrossRef] [PubMed]
- Ekowo, O.E.; Manafa, C.; Isielu, R.C.; Okoli, C.M.; Chikodi, I.; Onwuasoanya, A.F.; Echendu, S.T.; Ihedoro, I.; Nwabueze, U.D.; Nwoke, O.C. A cross sectional regional study looking at the factors responsible for the low COVID-19 vaccination rate in Nigeria. Pan Afr. Med. J. 2022, 41, 114. [Google Scholar] [CrossRef] [PubMed]
- Skeens, M.A.; Hill, K.; Olsavsky, A.; Buff, K.; Stevens, J.; Akard, T.F.; Shah, N.; Gerhardt, C.A. Factors affecting COVID-19 vaccine hesitancy in parents of children with cancer. Pediatr. Blood Cancer 2022, 69, e29707. [Google Scholar] [CrossRef]
- Walsh, J.C.; Comar, M.; Folan, J.; Williams, S.; Kola-Palmer, S. The psychological and behavioural correlates of COVID-19 vaccine hesitancy and resistance in Ireland and the UK. Acta Psychol. 2022, 225, 103550. [Google Scholar] [CrossRef]
- Betsch, C.; Wicker, S. E-health use, vaccination knowledge and perception of own risk: Drivers of vaccination uptake in medical students. Vaccine 2012, 30, 1143–1148. [Google Scholar] [CrossRef]
- Maurer, J.; Uscher-Pines, L.; Harris, K.M. Perceived seriousness of seasonal and A(H1N1) influenzas, attitudes toward vaccination, and vaccine uptake among U.S. adults: Does the source of information matter? Prev. Med. 2010, 51, 185–187. [Google Scholar] [CrossRef]
- Rubin, J.L.; McGarry, L.J.; Strutton, D.R.; Klugman, K.P.; Pelton, S.; Gilmore, K.E.; Weinstein, M.C. Public health and economic impact of the 13-valent pneumococcal conjugate vaccine (PCV13) in the United States. Vaccine 2010, 28, 7634–7643. [Google Scholar] [CrossRef]
- Chor, J.S.Y.; Pada, S.K.; Stephenson, I.; Goggins, W.B.; Tambyah, P.A.; Clarke, T.W.; Medina, M.; Lee, N.; Leung, T.F.; Ngai, K.L.; et al. Seasonal influenza vaccination predicts pandemic H1N1 vaccination uptake among healthcare workers in three countries. Vaccine 2011, 29, 7364–7369. [Google Scholar] [CrossRef]
- Seale, H.; Heywood, A.E.; McLaws, M.-L.; Ward, K.F.; Lowbridge, C.P.; Van, D.; MacIntyre, C.R. Why do I need it? I am not at risk! Public perceptions towards the pandemic (H1N1) 2009 vaccine. BMC Infect Dis. 2010, 10, 99. [Google Scholar] [CrossRef]
- Medeiros, K.S.; Costa, A.P.F.; Sarmento, A.C.A.; Freitas, C.L.; Gonçalves, A.K. Side effects of COVID-19 vaccines: A systematic review and meta-analysis protocol of randomised trials. BMJ Open 2022, 12, e050278. [Google Scholar] [CrossRef] [PubMed]
- Edwards, K.M.; Hackell, J.M. Committee on Infectious Diseases, Committee on Practice and Ambulatory Medicine. Countering Vaccine Hesitancy. Pediatrics 2016, 138, e20162146. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, J.; Halkitis, P.N. Towards a More Inclusive and Dynamic Understanding of Medical Mistrust Informed by Science. Behav. Med. 2019, 45, 79–85. [Google Scholar] [CrossRef] [PubMed]
- LaVeist, T.A.; Isaac, L.A.; Williams, K.P. Mistrust of Health Care Organizations Is Associated with Underutilization of Health Services. Health Serv. Res. 2009, 44, 2093–2105. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Eastwood, K.; Durrheim, D.N.; Jones, A.; Butler, M. Acceptance of pandemic (H1N1) 2009 influenza vaccination by the Australian public. Med. J. Aust. 2010, 192, 33–36. [Google Scholar] [CrossRef]
- Kata, A. Anti-vaccine activists, Web 2.0, and the postmodern paradigm—An overview of tactics and tropes used online by the anti-vaccination movement. Vaccine 2012, 30, 3778–3789. [Google Scholar] [CrossRef]
- Betsch, C.; Ulshöfer, C.; Renkewitz, F.; Betsch, T. The Influence of Narrative v. Statistical Information on Perceiving Vaccination Risks. Med. Decis. Mak. 2011, 31, 742–753. [Google Scholar] [CrossRef]
- Naeem, S.B.; Bhatti, R.; Khan, A. An exploration of how fake news is taking over social media and putting public health at risk. Health Inf. Libr. J. 2020, 38, 143–149. [Google Scholar] [CrossRef]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef]
- Siegrist, M.; Zingg, A. The Role of Public Trust during Pandemics: Implications for Crisis Communication. Eur. Psychol. 2014, 19, 23–32. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).