
Strategies for Treating Traumatic Neuromas with Tissue-Engineered Materials

 , , , ,
, , , ,
Abstract
1. Introduction
2. Peripheral Nerve Injury, Regeneration, and Traumatic Neuroma Formation
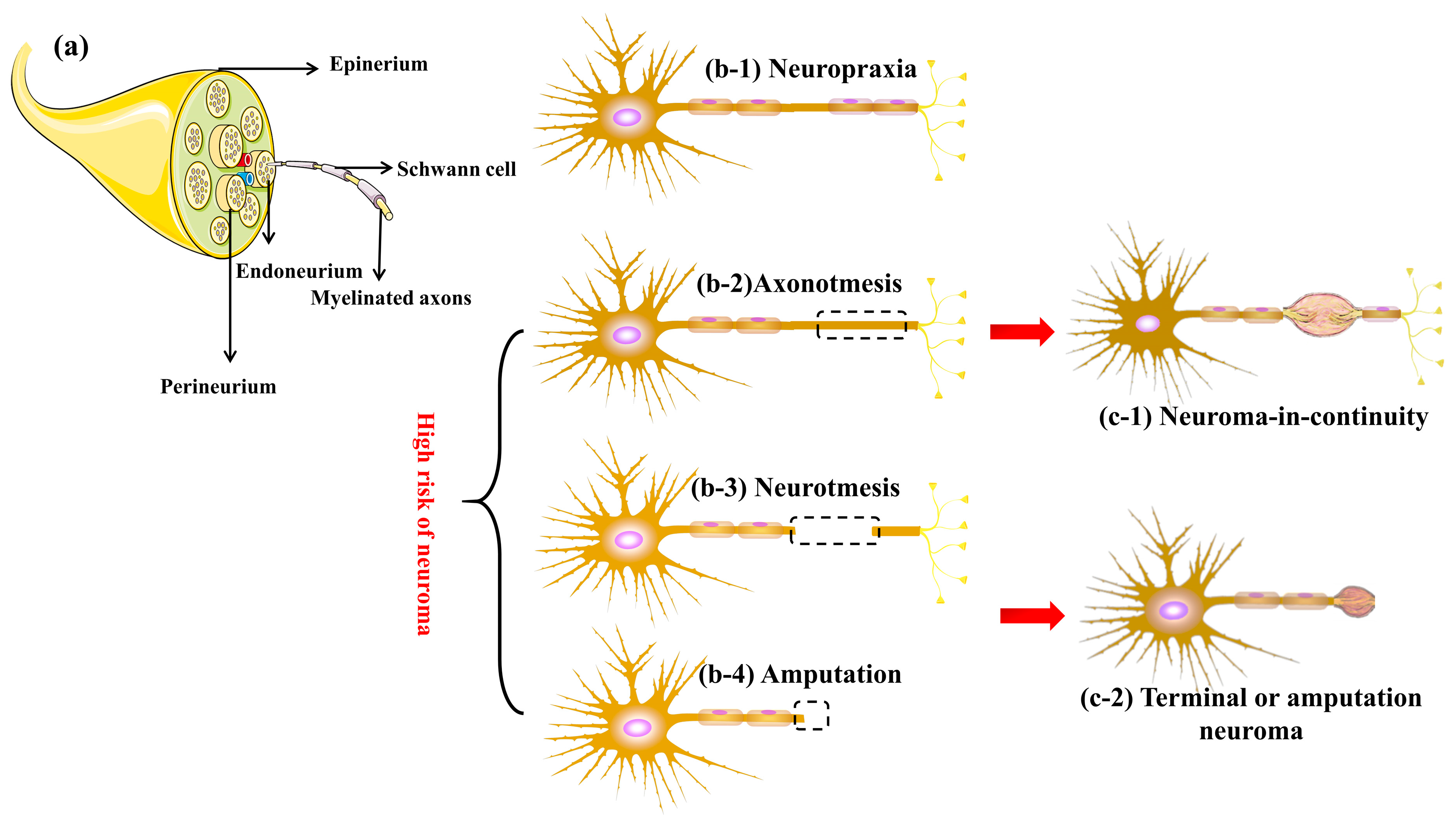
2.1. Peripheral Nerve Injuries and Neuroma
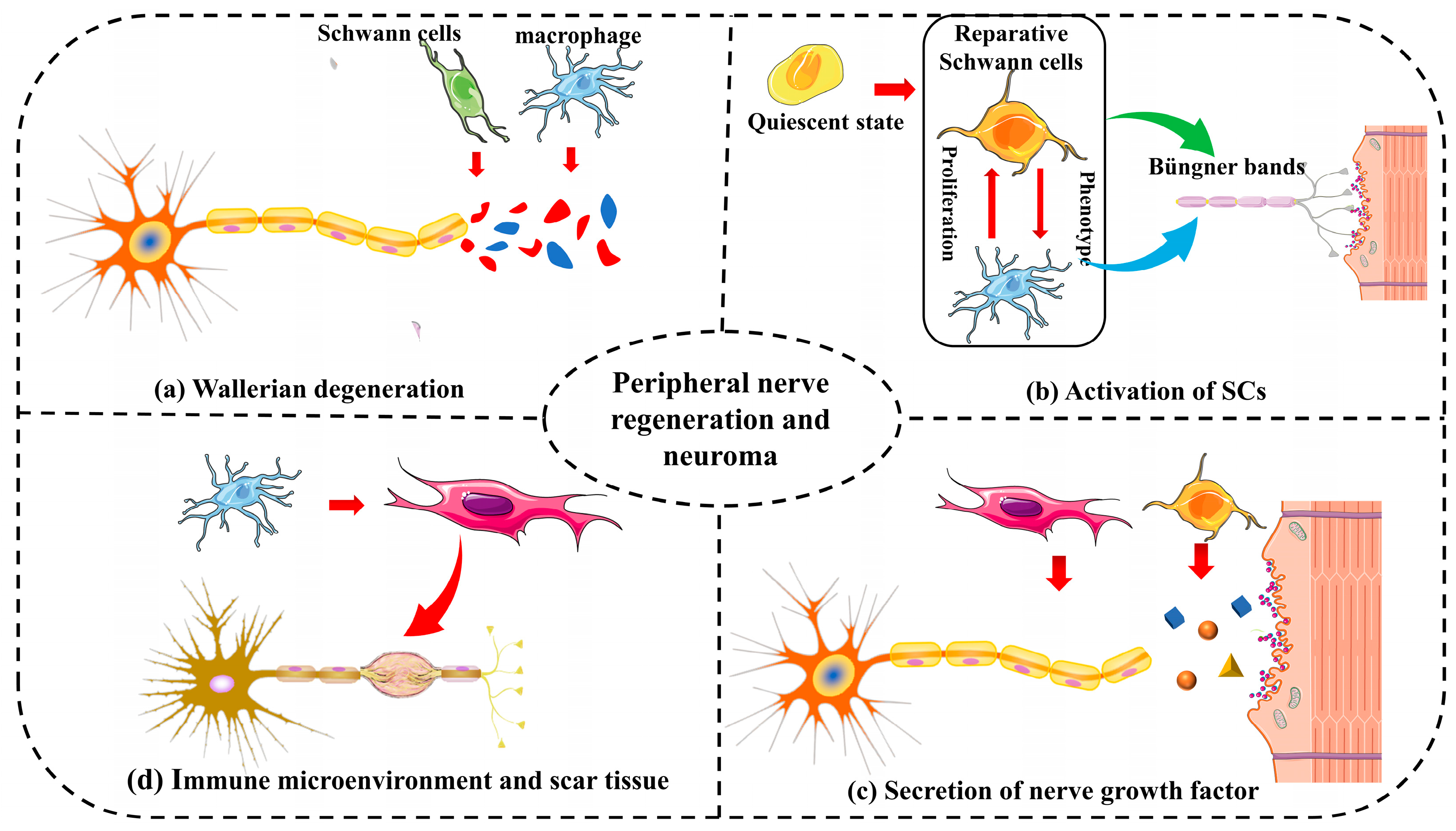
2.2. Peripheral Nerve Regeneration and Neuroma
2.3. Mechanisms of Neuroma Formation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Study and Methods | Source | Observations and Conclusions |
|---|---|---|---|
| NGF | The expression of NGF was quantified by immunohistochemistry [36]. | Damaged nerve axons | The expression of NGF was significantly elevated in patients with traumatic neuroma compared to normal individuals |
| The NGF receptors p75 and trkA and the BDNF receptor GFRalpha-1 were semiquantitatively analyzed by immunohistochemistry [37]. | Glial cells | The immunoreactivity of trkA receptor was significantly increased in the traumatic neuroma group | |
| A mouse model of severe limb injury was used to study the role of sensory nerve fibers in fibrous scar tissue travel [38]. | Myofibroblasts | NGF expressed by myofibroblasts is an important factor in the formation of neuroma after severe limb trauma | |
| BDNF | Expression of BDNF and its receptor trkB after sciatic nerve transection in wild-type and heterozygous trkB-deficient mice [31]. | Injured peripheral nerves | Trkb-deficient mice did not develop traumatic neuromas after long-stage peripheral nerve injury |
| After sciatic nerve transection, the rats were given BDNF-containing and antagonistic BDNF-containing connective tissue chambers, respectively, and the incidence of traumatic neuroma was observed [39]. | Endogenous secretion | BDNF plays a key role in the development of neuropathic pain after peripheral nerve injury, and its local inactivation reduces the incidence and severity of neuroma formation | |
| The formation of a neuroma 2 weeks after complete transection of the inferior alveolar nerve was confirmed by histological analysis [40]. | Damaged nerve axons | Local administration of DNF antibody inhibited the proliferation of connective tissue at the injured site, promoted the integrity of nerve fibers, and reduced the formation of traumatic neuroma | |
| Neuroinflammatory peptides | IL-6 antiserum or CGRP receptor antagonist was administered at the sciatic nerve ligation site [41]. | Calcitonin gene-related peptide (CGRP) is expressed by the axons of neuromas | CGRP is involved in the formation of neuroma by upregulating the secretion of IL-6 in macrophages |
| Neuroma model animals were treated daily with histidine and loratadine [42]. | Histamine; mast cell | Endogenous histamine reduces neuropathic pain caused by traumatic neuromas | |
| Immunostaining was used to compare the contents of substance P and CGRP in axons of normal and neuroma sides [33]. | Substance P; mast cell | The neuroma showed a large number of disorganized axonal contours and positive immunostaining for CGRP or Substance P | |
| Inflammatory factor | To compare the expression of anti-inflammatory factors and proinflammatory factors in neuroma [43]. | TNF-α, IL-1β, IL-6, and IL-10 | IL-6 and IL-1β may play a role in the formation of traumatic neuroma, while IL-10 may inhibit neuroma formation |
| The expression of inflammatory factor genes in the injured sciatic nerve was detected [44]. | IL-1β, IL-10, IFN-γ, and TNF-α; macrophage | The high expression of proinflammatory and anti-inflammatory cytokines may be associated with the formation of fibrosis caused by irreversible nerve injury and, therefore, may be associated with the formation of traumatic neuroma | |
| Quantitative analysis of the expression of inflammatory factors in peripheral nerve stump [30]. | TNF-α, IL-6, and IL-1β | Expression of proinflammatory cytokines TNF-α, IL-6, and IL-1β was significantly increased in the dorsal root ganglia of traumatic neuromas | |
| α-SMA | The expression of α-SMA in neuroma was observed by immunofluorescence staining [35]. | Myofibroblasts | The expression of α-SMA was positively correlated with the pain index of patients |
| A rat model of amputated neuroma was used to quantitatively analyze the expression of α-SMA [45]. | Myofibroblasts | Levels of α-SMA and the pain marker c-fos were significantly higher in the amputation group | |
| Quantitative analysis of α-SMA expression in the terminal of neuroma was performed [46]. | Myofibroblasts | Capping transected rat sciatic nerves while concurrently administering myelin-associated glycoprotein was linked to reduced levels of α-SMA and autotomy behavior |
3. Traditional Treatment Options and Challenges
3.1. Nonsurgical Treatments
3.2. Surgical Treatments
4. Tissue-Engineered Materials for Neuromas
4.1. Composition and Types of Tissue-Engineered Materials
4.1.1. Composition of Tissue-Engineered Materials
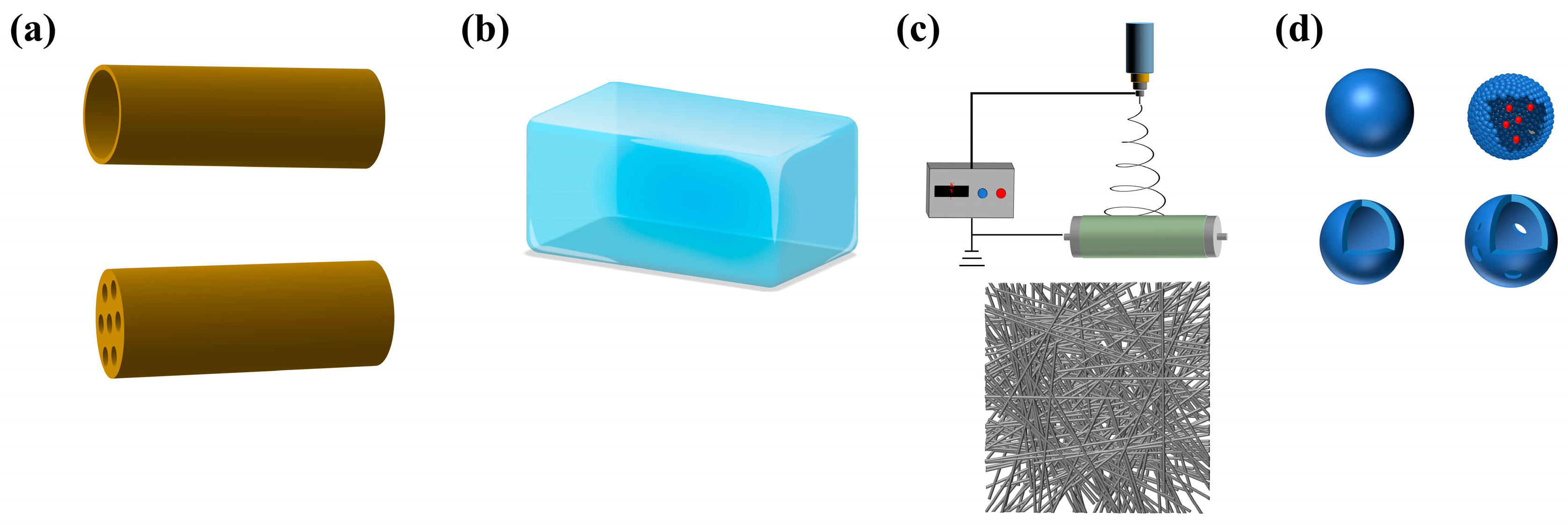
4.1.2. Type of Tissue-Engineered Materials
4.2. Biomaterial-Based Scaffolds

4.3. Growth Factor Incorporation
| Growth Factors | Receptors | Signaling Pathways | Bio-Function in Promoting Peripheral Nerve Regeneration |
|---|---|---|---|
| Nerve growth factor (NGF) [83] | TrkA, p75NTR |
|
|
| Brain-derived neurotrophic factor (BDNF) [84] | TrkB, p75NTR |
|
|
| Glial-derived neurotrophic factor (GDNF) [85] | GFRα 1~4 |
|
|
| Neurotrophin-3 (NT-3) [86] | TrkC, p75NTR |
|
|
| Insulin-like growth factor (IGF-1) [87] | IGF 1R, and 2R |
|
|
| Basic fibroblast growth factor (bFGF) [88] | FGFR I-IIIc |
|
|
| Vascular endothelial growth factor (VEGF) [89] | VEGF R1~R3 NP1, NP2 |
|
|
4.4. Cell-Based Approaches

4.5. Electrical Stimulation
5. Summary and Challenge
Author Contributions
Funding
Conflicts of Interest
References
- List, E.B.; Krijgh, D.D.; Martin, E.; Coert, J.H. Prevalence of residual limb pain and symptomatic neuromas after lower extremity amputation: A systematic review and meta-analysis. Pain 2021, 162, 1906–1913. [Google Scholar] [CrossRef]
- Hwang, C.D.; Hoftiezer, Y.A.J.; Raasveld, F.V.; Gomez-Eslava, B.; van der Heijden, E.P.A.; Jayakar, S.; Black, B.J.; Johnston, B.R.; Wainger, B.J.; Renthal, W.; et al. Biology and pathophysiology of symptomatic neuromas. Pain 2022, 60, 550–564. [Google Scholar] [CrossRef] [PubMed]
- Tal, M.; Minert, A.; Devor, M. Resurgent neuropathic discharge: An obstacle to the therapeutic use of neuroma resection? Pain 2023, 164, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Janes, L.E.; Fracol, M.E.; Dumanian, G.A.; Ko, J.H. Targeted Muscle Reinnervation for the Treatment of Neuroma. Hand Clin. 2021, 37, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Starr, B.W.; Chung, K.C. Traditional Neuroma Management. Hand Clin. 2021, 37, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Shamoun, F.; Shamoun, V.; Akhavan, A.; Tuffaha, S.H. Target Receptors of Regenerating Nerves: Neuroma Formation and Current Treatment Options. Front. Mol. Neurosci. 2022, 15, 859221. [Google Scholar] [CrossRef] [PubMed]
- Qian, Y.; Cheng, Y.; Cai, J.; Zhao, X.; Ouyang, Y.; Yuan, W.E.; Fan, C. Advances in electrical and magnetic stimulation on nerve regeneration. Regen. Med. 2019, 14, 969–979. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.B.; Winograd, J.M.; Redmond, R.W. Surgical Approaches for Prevention of Neuroma at Time of Peripheral Nerve Injury. Front. Surg. 2022, 9, 819608. [Google Scholar] [CrossRef] [PubMed]
- Dumanian, G.A.; Potter, B.K.; Mioton, L.M.; Ko, J.H.; Cheesborough, J.E.; Souza, J.M.; Ertl, W.J.; Tintle, S.M.; Nanos, G.P.; Valerio, I.L.; et al. Targeted Muscle Reinnervation Treats Neuroma and Phantom Pain in Major Limb Amputees: A Randomized Clinical Trial. Ann. Surg. 2019, 270, 238–246. [Google Scholar] [CrossRef]
- Yang, Q.; Su, S.; Liu, S.; Yang, S.; Xu, J.; Zhong, Y.; Yang, Y.; Tian, L.; Tan, Z.; Wang, J.; et al. Exosomes-loaded electroconductive nerve dressing for nerve regeneration and pain relief against diabetic peripheral nerve injury. Bioact. Mater. 2023, 26, 194–215. [Google Scholar] [CrossRef]
- Sisti, A.; Uygur, S.; Lopez-Schultz, S.D.; Konofaos, P. Nerve Capping Techniques for Neuroma Management: A Comprehensive Literature Review. Ann. Plast. Surg. 2024, 92, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.; Deng, P.J.; He, F.L.; Yan, L.W.; Tu, Z.H.; Liu, X.L.; Quan, D.P.; Bai, Y.; Zheng, C.B.; Zhu, Q.T. A decellularized nerve matrix scaffold inhibits neuroma formation in the stumps of transected peripheral nerve after peripheral nerve injury. Neural Regen. Res. 2023, 18, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Wan, T.; Zhang, F.-S.; Qin, M.-Y.; Jiang, H.-R.; Zhang, M.; Qu, Y.; Wang, Y.-L.; Zhang, P.-X. Growth factors: Bioactive macromolecular drugs for peripheral nerve injury treatment—Molecular mechanisms and delivery platforms. Biomed. Pharmacother. 2024, 170, 116024. [Google Scholar] [CrossRef] [PubMed]
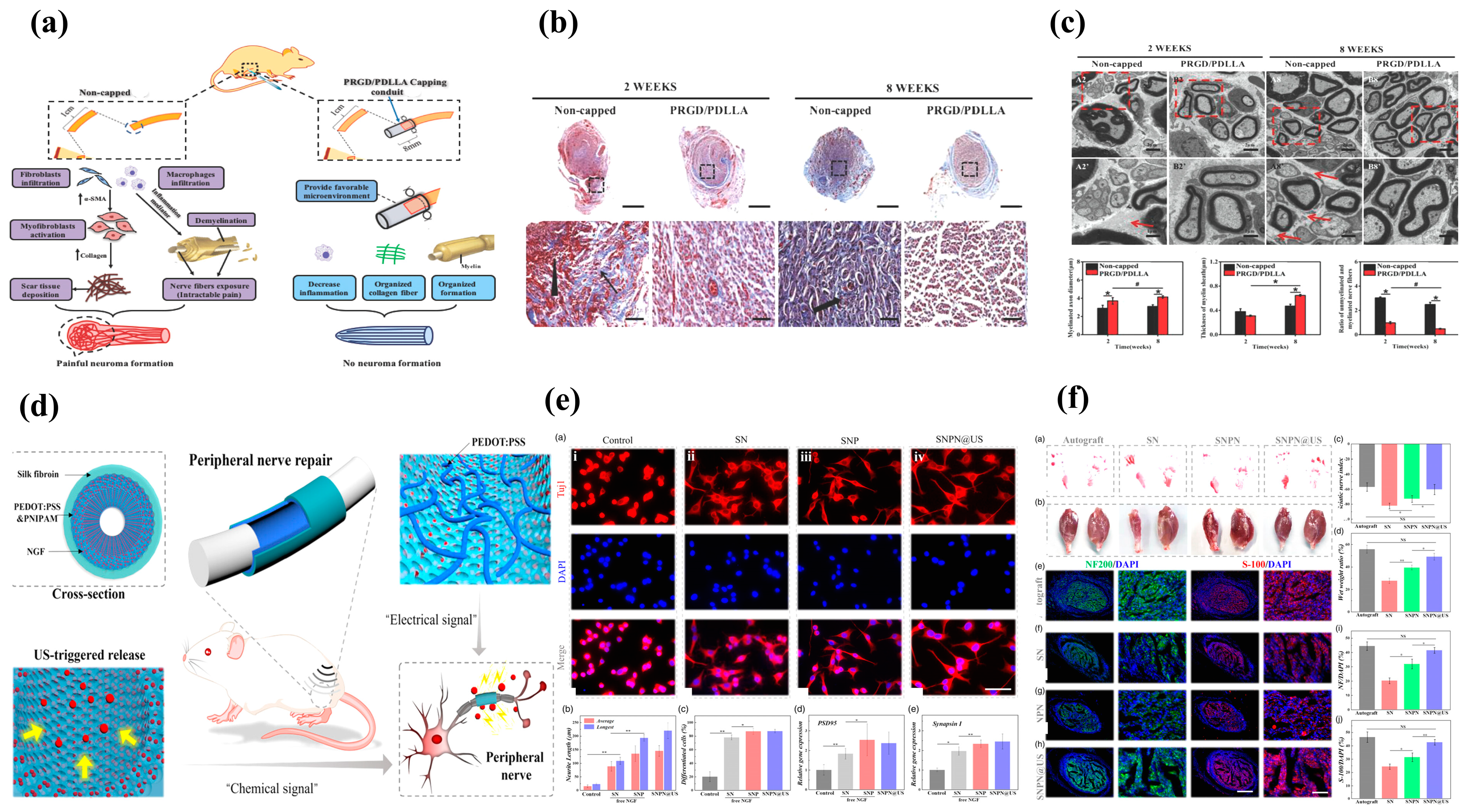
- Yin, Y.; Li, B.; Yan, Q.; Dai, H.; Wang, X.; Huang, J.; Li, S. Promotion of peripheral nerve regeneration and prevention of neuroma formation by PRGD/PDLLA/β-TCP conduit: Report of two cases. Regen. Biomater. 2015, 2, 119–124. [Google Scholar] [CrossRef]
- Yang, X.; Huang, L.; Yi, X.; Huang, S.; Duan, B.; Yu, A. Multifunctional chitin-based hollow nerve conduit for peripheral nerve regeneration and neuroma inhibition. Carbohydr. Polym. 2022, 289, 119443. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Lang, Y.; Chang, M.-W.; Zhao, M.; Li, C.; Liu, S.; Wang, B. Leveraging Oriented Lateral Walls of Nerve Guidance Conduit with Core–Shell MWCNTs Fibers for Peripheral Nerve Regeneration. Adv. Healthc. Mater. 2024, 2303867. [Google Scholar] [CrossRef] [PubMed]
- Kocher, M.; Yilmaz, S.; Visoiu, M. Sciatic nerve neuropraxia following embolization therapy in a patient receiving quadratus lumborum nerve block. J. Clin. Anesth. 2022, 78, 110601. [Google Scholar] [CrossRef]
- Kim, H.W.; Shim, S.W.; Zhao, A.M.; Roh, D.; Han, H.M.; Middleton, S.J.; Kim, W.; Chung, S.; Johnson, E.; Prentice, J.; et al. Long-term tactile hypersensitivity after nerve crush injury in mice is characterized by the persistence of intact sensory axons. Pain 2023, 164, 2327–2342. [Google Scholar] [CrossRef] [PubMed]
- Fordington, S.; Manford, M. A review of seizures and epilepsy following traumatic brain injury. J. Neurol. 2020, 267, 3105–3111. [Google Scholar] [CrossRef]
- Chhabra, A.; Ahlawat, S.; Belzberg, A.; Andreseik, G. Peripheral nerve injury grading simplified on MR neurography: As referenced to Seddon and Sunderland classifications. Indian J. Radiol. Imaging 2014, 24, 217–224. [Google Scholar] [CrossRef]
- Barberá, J.; Garcia, G.; Lopez-Orta, A.; Gil-Salu, J.L. The role of the neuroma in autotomy following sciatic nerve section in rats. Pain 1988, 33, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Wan, T.; Wang, Y.L.; Zhang, F.S.; Zhang, X.M.; Zhang, Y.C.; Jiang, H.R.; Zhang, M.; Zhang, P.X. The Porous Structure of Peripheral Nerve Guidance Conduits: Features, Fabrication, and Implications for Peripheral Nerve Regeneration. Int. J. Mol. Sci. 2023, 24, 14132. [Google Scholar] [CrossRef] [PubMed]
- Han, G.H.; Peng, J.; Liu, P.; Ding, X.; Wei, S.; Lu, S.; Wang, Y. Therapeutic strategies for peripheral nerve injury: Decellularized nerve conduits and Schwann cell transplantation. Neural Regen. Res. 2019, 14, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Min, Q.; Parkinson, D.B.; Dun, X.P. Migrating Schwann cells direct axon regeneration within the peripheral nerve bridge. Glia 2021, 69, 235–254. [Google Scholar] [CrossRef]
- Jha, M.K.; Passero, J.V.; Rawat, A.; Ament, X.H.; Yang, F.; Vidensky, S.; Collins, S.L.; Horton, M.R.; Hoke, A.; Rutter, G.A.; et al. Macrophage monocarboxylate transporter 1 promotes peripheral nerve regeneration after injury in mice. J. Clin. Investig. 2021, 131, e141964. [Google Scholar] [CrossRef] [PubMed]
- Lindenlaub, T.; Sommer, C. Partial sciatic nerve transection as a model of neuropathic pain: A qualitative and quantitative neuropathological study. Pain 2000, 89, 97–106. [Google Scholar] [CrossRef]
- Mathieu, L.; Diner, C.; Aries, P.; Thomas, M.; Truffaut, S.; de L’escalopier, N. Preemptive targeted muscle reinnervation: The single incision approach should be avoided in trans-tibial traumatic amputation. Military Med. Res. 2022, 9, 60. [Google Scholar] [CrossRef]
- Foltán, R.; Klíma, K.; Spacková, J.; Sedy, J. Mechanism of traumatic neuroma development. Med. Hypotheses 2008, 71, 572–576. [Google Scholar] [CrossRef] [PubMed]
- Ji, F.; Zhang, Y.Y.; Cui, P.; Li, Y.; Li, C.X.; Du, D.P.; Xu, H. Preventive Effect of Local Lidocaine Administration on the Formation of Traumatic Neuroma. J. Clin. Med. 2023, 12, 2476. [Google Scholar] [CrossRef]
- Pu, S.; Wu, Y.; Tong, F.; Du, W.-J.; Liu, S.; Yang, H.; Zhang, C.; Zhou, B.; Chen, Z.; Zhou, X.; et al. Mechanosensitive Ion Channel TMEM63A Gangs Up with Local Macrophages to Modulate Chronic Post-amputation Pain. Neurosci. Bull. 2023, 39, 177–193. [Google Scholar] [CrossRef]
- Kotulska, K.; Larysz-Brysz, M.; Marcol, W.; Grajkowska, W.; Józwiak, S.; Lewin-Kowalik, J. The role of trkB receptor in the formation of post-traumatic neuroma. Folia Neuropathol. 2006, 44, 221–227. [Google Scholar]
- Jimenez-Andrade, J.M.; Ghilardi, J.R.; Castañeda-Corral, G.; Kuskowski, M.A.; Mantyh, P.W. Preventive or late administration of anti-NGF therapy attenuates tumor-induced nerve sprouting, neuroma formation, and cancer pain. Pain 2011, 152, 2564–2574. [Google Scholar] [CrossRef] [PubMed]
- Zochodne, D.W.; Theriault, M.; Sharkey, K.A.; Cheng, C.; Sutherland, G. Peptides and neuromas: Calcitonin gene-related peptide, substance P, and mast cells in a mechanosensitive human sural neuroma. Muscle Nerve 1997, 20, 875–880. [Google Scholar] [CrossRef]
- Xie, W.R.; Strong, J.A.; Zhang, J.M. Localized sympathectomy reduces peripheral nerve regeneration and pain behaviors in 2 rat neuropathic pain models. Pain 2020, 161, 1925–1936. [Google Scholar] [CrossRef]
- Yan, H.D.; Gao, W.Y.; Pan, Z.J.; Zhang, F.; Fan, C.Y. The Expression of α-SMA in the Painful Traumatic Neuroma: Potential Role in the Pathobiology of Neuropathic Pain. J. Neurotrauma 2012, 29, 2791–2797. [Google Scholar] [CrossRef]
- Atherton, D.D.; Taherzadeh, O.; Facer, P.; Elliot, D.; Anand, P. The potential role of nerve growth factor (NGF) in painful neuromas and the mechanism of pain relief by their relocation to muscle. J. Hand Surg.-Br. Eur. Vol. 2006, 31B, 652–656. [Google Scholar] [CrossRef]
- Harpf, C.; Dabernig, J.; Humpel, C. Receptors for NGF and GDNF are highly expressed in human peripheral nerve neuroma. Muscle Nerve 2002, 25, 612–615. [Google Scholar] [CrossRef]
- Lee, S.Y.; Hwang, C.; Marini, S.; Tower, R.J.; Qin, Q.Z.; Negri, S.; Pagani, C.A.; Sun, Y.X.; Stepien, D.M.; Sorkin, M.; et al. NGF-TrkA signaling dictates neural ingrowth and aberrant osteochondral differentiation after soft tissue trauma. Nat. Commun. 2021, 12, 4939. [Google Scholar] [CrossRef] [PubMed]
- Marcol, W.; Kotulska, K.; Larysz-Brysz, M.; Kowalik, J.L. BDNF contributes to animal model neuropathic pain after peripheral nerve transection. Neurosurg. Rev. 2007, 30, 235–243. [Google Scholar] [CrossRef]
- Guevara, Y.M.V.; Yoshikawa, H.; Saito, I.; Maeda, T.; Seo, K. Effect of local application of an antibody against brain-derived neurotrophic factor on neuroma formation after transection of the inferior alveolar nerve in the rat. Neuroreport 2014, 25, 1069–1074. [Google Scholar] [CrossRef]
- Ma, W.Y.; Quirion, R. Increased calcitonin gene-related peptide in neuroma and invading macrophages is involved in the up-regulation of interleukin-6 and thermal hyperalgesia in a rat model of mononeuropathy. J. Neurochem. 2006, 98, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Lou, G.D.; Yue, J.X.; Tang, Y.Y.; Hou, W.W.; Shou, W.T.; Ohtsu, H.; Zhang, S.H.; Chen, Z. Effects of histamine on spontaneous neuropathic pain induced by peripheral axotomy. Neurosci. Bull. 2013, 29, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.; Noboru, N.; Young, A.; Thomas, D. Pro and anti-inflammatory cytokine levels (TNF-α, IL-1β, IL-6 and IL-10) in rat model of neuroma. Pathophysiology 2017, 24, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Ruohonen, S.; Khademi, M.; Jagodic, M.; Taskinen, H.S.; Olsson, T.; Röyttä, M. Cytokine responses during chronic denervation. J. Neuroinflamm. 2005, 2, 26. [Google Scholar] [CrossRef] [PubMed]
- Weng, W.D.; Zhao, B.; Lin, D.S.; Gao, W.Y.; Li, Z.J.; Yan, H.D. Significance of alpha smooth muscle actin expression in traumatic painful neuromas: A pilot study in rats. Sci. Rep. 2016, 6, 23828. [Google Scholar] [CrossRef] [PubMed]
- Pi, W.; Li, C.; Zhang, M.; Zhang, W.; Zhang, P.X. Myelin-associated glycoprotein combined with chitin conduit inhibits painful neuroma formation after sciatic nerve transection. Neural Regen. Res. 2022, 17, 1343–1347. [Google Scholar] [CrossRef] [PubMed]
- Morrison, D.R.; Moore, L.S.; Walsh, E.M. Perioperative Pain Management Following Otologic Surgery. Otolaryngol. Clin. N. Am. 2020, 53, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Lans, J.; Westenberg, R.F.; Gottlieb, R.E.; Valerio, I.L.; Chen, N.C.; Eberlin, K.R. Long-Term Opioid Use Following Surgery for Symptomatic Neuroma. J. Reconstr. Microsurg. 2022, 38, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Kent, M.L.; Hsia, H.L.J.; Van de Ven, T.J.; Buchheit, T.E. Perioperative Pain Management Strategies for Amputation: A Topical Review. Pain Med. 2017, 18, 504–519. [Google Scholar] [CrossRef][Green Version]
- Sperry, B.P.; Cheney, C.W.; Conger, A.; Shipman, H.; McCormick, Z.L. Cooled Radiofrequency Ablation of a Large Sciatic Neuroma at the Infrapiriformis Foramen for Recalcitrant Phantom Limb Pain in a Below-Knee Amputee. Pain Med. 2020, 22, 223–226. [Google Scholar] [CrossRef]
- Gougoulias, N.; Lampridis, V.; Sakellariou, A. Morton’s interdigital neuroma: Instructional review. EFORT Open Rev. 2019, 4, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Ernberg, L.A.; Adler, R.S.; Lane, J. Ultrasound in the detection and treatment of a painful stump neuroma. Skeletal Radiol. 2003, 32, 306–309. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.B.; Jacobs, A.; Williams, K.L.; Bour, R.K.; Gyftopoulos, S. Ultrasound-Guided Injection Treatments Versus Surgical Neurectomy for Morton Neuroma: A Cost-Effectiveness Analysis. Am. J. Roentgenol. 2022, 218, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Hertzano, R.; Eisenman, D.J. Large, Symptomatic Tension Pneumocele: 23 Years After Translabyrinthine Resection of an Acoustic Neuroma. Otolaryngol.-Head Neck Surg. 2011, 144, 477–478. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Dip, T.M.; Padhye, R.; Houshyar, S. Review on electrically conductive smart nerve guide conduit for peripheral nerve regeneration. J. Biomed. Mater. Res. Part A 2023, 111, 1916–1950. [Google Scholar] [CrossRef] [PubMed]
- Kerasnoudis, A.; Yoon, M.S. Relapsing Neuromas: A Therapeutic Challenge? Clin. J. Pain 2013, 29, 280. [Google Scholar] [CrossRef] [PubMed]
- Wolvetang, N.H.A.; Lans, J.; Verhiel, S.H.W.L.; Notermans, B.J.W.; Chen, N.C.; Eberlin, K.R. Surgery for Symptomatic Neuroma: Anatomic Distribution and Predictors of Secondary Surgery. Plast. Reconstr. Surg. 2019, 143, 1762–1771. [Google Scholar] [CrossRef]
- Roth, E.; Linehan, A.; Weihrauch, D.; Stucky, C.; Hogan, Q.; Hoben, G. Targeted muscle reinnervation prevents and reverses rat pain behaviors after nerve transection. Pain 2023, 164, 316–324. [Google Scholar] [CrossRef] [PubMed]
- González-Prieto, J.; Cristóbal, L.; Arenillas, M.; Giannetti, R.; Muñoz Frías, J.D.; Alonso Rivas, E.; Sanz Barbero, E.; Gutiérrez-Pecharromán, A.; Díaz Montero, F.; Maldonado, A.A. Regenerative Peripheral Nerve Interfaces (RPNIs) in Animal Models and Their Applications: A Systematic Review. Int. J. Mol. Sci. 2024, 25, 1141. [Google Scholar] [CrossRef]
- Liu, K.; Yan, L.S.; Li, R.T.; Song, Z.M.; Ding, J.X.; Liu, B.; Chen, X.S. 3D Printed Personalized Nerve Guide Conduits for Precision Repair of Peripheral Nerve Defects. Adv. Sci. 2022, 9, 2103875. [Google Scholar] [CrossRef]
- Zhang, H.; Guo, J.H.; Wang, Y.; Shang, L.R.; Chai, R.J.; Zhao, Y.J. Natural Polymer-Derived Bioscaffolds for Peripheral Nerve Regeneration. Adv. Funct. Mater. 2022, 32, 2203829. [Google Scholar] [CrossRef]
- Deng, P.; Chen, F.; Zhang, H.; Chen, Y.; Zhou, J. Multifunctional Double-Layer Composite Hydrogel Conduit Based on Chitosan for Peripheral Nerve Repairing. Adv. Healthc. Mater. 2022, 11, 2200115. [Google Scholar] [CrossRef] [PubMed]
- Maksoud, F.J.; Velázquez de la Paz, M.F.; Hann, A.J.; Thanarak, J.; Reilly, G.C.; Claeyssens, F.; Green, N.H.; Zhang, Y.S. Porous biomaterials for tissue engineering: A review. J. Mater. Chem. B 2022, 10, 8111–8165. [Google Scholar] [CrossRef]
- Valentino, C.; Vigani, B.; Zucca, G.; Ruggeri, M.; Marrubini, G.; Boselli, C.; Icaro Cornaglia, A.; Sandri, G.; Rossi, S. Design of Novel Mechanically Resistant and Biodegradable Multichannel Platforms for the Treatment of Peripheral Nerve Injuries. Biomacromolecules 2023, 24, 1731–1743. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.; Wang, G.; Qian, T.; Cai, X.; Zhang, P.; Li, M.; Shen, Y.; Xue, C.; Wang, H. The balanced microenvironment regulated by the degradants of appropriate PLGA scaffolds and chitosan conduit promotes peripheral nerve regeneration. Mater. Today Bio 2021, 12, 100158. [Google Scholar] [CrossRef] [PubMed]
- Yao, Z.; Yuan, W.; Xu, J.; Tong, W.; Mi, J.; Ho, P.-C.; Chow, D.H.K.; Li, Y.; Yao, H.; Li, X.; et al. Magnesium-Encapsulated Injectable Hydrogel and 3D-Engineered Polycaprolactone Conduit Facilitate Peripheral Nerve Regeneration. Adv. Sci. 2022, 9, 2202102. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Gong, J.; Zhang, J.; Zhu, Z.; Qian, Y.; Lu, K.; Zhou, S.; Gu, T.; Wang, H.; He, Y.; et al. Three Potential Elements of Developing Nerve Guidance Conduit for Peripheral Nerve Regeneration. Adv. Funct. Mater. 2023, 33, 2302251. [Google Scholar] [CrossRef]
- Fang, Y.; Wang, C.; Liu, Z.; Ko, J.; Chen, L.; Zhang, T.; Xiong, Z.; Zhang, L.; Sun, W. 3D Printed Conductive Multiscale Nerve Guidance Conduit with Hierarchical Fibers for Peripheral Nerve Regeneration. Adv. Sci. 2023, 10, 2205744. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, X.; Xiao, C.; Liu, B. Engineered hydrogels for peripheral nerve repair. Mater. Today Bio 2023, 20, 100668. [Google Scholar] [CrossRef]
- Xu, W.; Wu, Y.; Lu, H.; Zhang, X.; Zhu, Y.; Liu, S.; Zhang, Z.; Ye, J.; Yang, W. Injectable hydrogel encapsulated with VEGF-mimetic peptide-loaded nanoliposomes promotes peripheral nerve repair in vivo. Acta Biomater. 2023, 160, 225–238. [Google Scholar] [CrossRef]
- Cai, C.; Zhu, H.; Chen, Y.; Chen, C.; Li, H.; Yang, Z.; Liu, H. Conductive nerve guide conduits based on wet-adhesive hydrogel to accelerate peripheral nerve repair. Appl. Mater. Today 2022, 27, 101491. [Google Scholar] [CrossRef]
- Li, X.; He, N.; Li, X.; Wang, X.; Zhan, L.; Yuan, W.-E.; Song, J.; Ouyang, Y. Graphdiyne-loaded polycaprolactone nanofiber scaffold for peripheral nerve regeneration. J. Colloid Interface Sci. 2023, 646, 399–412. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Thow, S.Y.; Abdullah, S.; Ng, M.H.; Haflah, N.H.M. Advancement of Electrospun Nerve Conduit for Peripheral Nerve Regeneration: A Systematic Review (2016–2021). Int. J. Nanomed. 2022, 17, 6723–6758. [Google Scholar] [CrossRef] [PubMed]
- Liang, F.; Yang, Y.; Chen, Y.; Xie, J.; Liu, S.; Tan, Z.; Tian, L.; Yu, Z.; Shi, Z.; Xie, P.; et al. Ropivacaine microsphere-loaded electroconductive nerve dressings for long-acting analgesia and functional recovery following diabetic peripheral nerve injury. Mater. Today Bio 2023, 21, 100712. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Chang, B.; Dong, H.; Liu, X. Functional microspheres for tissue regeneration. Bioact. Mater. 2023, 25, 485–499. [Google Scholar] [CrossRef]
- Yi, J.; Jiang, N.; Li, B.; Yan, Q.; Qiu, T.; Swaminatha Iyer, K.; Yin, Y.; Dai, H.; Yetisen, A.K.; Li, S. Painful Terminal Neuroma Prevention by Capping PRGD/PDLLA Conduit in Rat Sciatic Nerves. Adv. Sci. 2018, 5, 1700876. [Google Scholar] [CrossRef] [PubMed]
- Fadia, N.B.; Bliley, J.M.; DiBernardo, G.A.; Crammond, D.J.; Schilling, B.K.; Sivak, W.N.; Spiess, A.M.; Washington, K.M.; Waldner, M.; Liao, H.T.; et al. Long-gap peripheral nerve repair through sustained release of a neurotrophic factor in nonhuman primates. Sci. Transl. Med. 2020, 12, eaav7753. [Google Scholar] [CrossRef] [PubMed]
- Dong, Q.; Ai, J.; Xiao, A.; Wu, P.; Wu, M.; Liu, X.; Huselstein, C.; Cai, L.; Feng, X.; Chen, Y. Nerve Defect Treatment with a Capping Hydroxyethyl Cellulose/Soy Protein Isolate Sponge Conduit for Painful Neuroma Prevention. ACS Omega 2023, 8, 30850–30858. [Google Scholar] [CrossRef]
- Millán, D.; Jiménez, R.A.; Nieto, L.E.; Poveda, I.Y.; Torres, M.A.; Silva, A.S.; Ospina, L.F.; Mano, J.F.; Fontanilla, M.R. Adjustable conduits for guided peripheral nerve regeneration prepared from bi-zonal unidirectional and multidirectional laminar scaffold of type I collagen. Mater. Sci. Eng. C 2021, 121, 111838. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, H.; Wen, B.; Lu, L.; Zhao, Y.; Chai, R. Ultrasound-Responsive Composited Conductive Silk Conduits for Peripheral Nerve Regeneration. Small Struct. 2023, 4, 2300045. [Google Scholar] [CrossRef]
- Xu, H.X.; Yu, Y.; Zhang, L.X.; Zheng, F.R.; Yin, Y.X.; Gao, Y.X.; Li, K.B.; Xu, J.Y.; Wen, J.; Chen, H.; et al. Sustainable release of nerve growth factor for peripheral nerve regeneration using nerve conduits laden with Bioconjugated hyaluronic acid-chitosan hydrogel. Compos. Part B-Eng. 2022, 230, 109509. [Google Scholar] [CrossRef]
- Zhu, L.; Jia, S.; Liu, T.; Yan, L.; Huang, D.; Wang, Z.; Chen, S.; Zhang, Z.; Zeng, W.; Zhang, Y.; et al. Aligned PCL Fiber Conduits Immobilized with Nerve Growth Factor Gradients Enhance and Direct Sciatic Nerve Regeneration. Adv. Funct. Mater. 2020, 30, 2002610. [Google Scholar] [CrossRef]
- Jiao, J.; Wang, F.; Huang, J.-J.; Huang, J.-J.; Li, Z.-A.; Kong, Y.; Zhang, Z.-J. Microfluidic hollow fiber with improved stiffness repairs peripheral nerve injury through non-invasive electromagnetic induction and controlled release of NGF. Chem. Eng. J. 2021, 426, 131826. [Google Scholar] [CrossRef]
- Huang, L.Y.; Jin, J.H.; Chen, K.; You, S.K.; Zhang, H.Y.; Sideris, A.; Norcini, M.; Recio-Pinto, E.; Wang, J.; Gan, W.B.; et al. BDNF produced by cerebral microglia promotes cortical plasticity and pain hypersensitivity after peripheral nerve injury. PLoS Biol. 2021, 19, e3001337. [Google Scholar] [CrossRef] [PubMed]
- Cintron-Colon, A.F.; Almeida-Alves, G.; VanGyseghem, J.M.; Spitsbergen, J.M. GDNF to the rescue: GDNF delivery effects on motor neurons and nerves, and muscle re-innervation after peripheral nerve injuries. Neural Regen. Res. 2022, 17, 748–753. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Song, L.; Li, Y.; Guo, J.; Huang, S.; Du, S.; Li, W.; Cao, R.; Cui, S. Neurotrophin-3 promotes peripheral nerve regeneration by maintaining a repair state of Schwann cells after chronic denervation via the TrkC/ERK/c-Jun pathway. J. Transl. Med. 2023, 21, 733. [Google Scholar] [CrossRef] [PubMed]
- Hanwright, P.J.; Qiu, C.H.; Rath, J.; Zhou, Y.; von Guionneau, N.; Sarhane, K.A.; Harris, T.G.W.; Howard, G.P.; Malapati, H.; Lan, M.J.; et al. Sustained IGF-1 delivery ameliorates effects of chronic denervation and improves functional recovery after peripheral nerve injury and repair. Biomaterials 2022, 280, 121244. [Google Scholar] [CrossRef] [PubMed]
- Idrisova, K.F.; Zeinalova, A.K.; Masgutova, G.A.; Bogov, A.A.; Allegrucci, C.; Syromiatnikova, V.Y.; Salafutdinov, I.I.; Garanina, E.E.; Andreeva, D.I.; Kadyrov, A.A.; et al. Application of neurotrophic and proangiogenic factors as therapy after peripheral nervous system injury. Neural Regen. Res. 2022, 17, 1240–1247. [Google Scholar] [CrossRef]
- Gao, Y.S.; Dai, C.L.; Zhang, M.; Zhang, J.Y.; Yin, L.; Li, W.H.; Zhang, K.Y.; Yang, Y.M.; Zhao, Y.H. Biomimetic Silk Fibroin Hydrogel for Enhanced Peripheral Nerve Regeneration: Synergistic Effects of Graphene Oxide and Fibroblast Exosome. Adv. Funct. Mater. 2023, 2314610. [Google Scholar] [CrossRef]
- Lei, W.-L.; Peng, C.-W.; Chiu, S.-C.; Lu, H.-E.; Wu, C.-W.; Cheng, T.-Y.; Huang, W.-C. All Biodisintegratable Hydrogel Biohybrid Neural Interfaces with Synergistic Performances of Microelectrode Array Technologies, Tissue Scaffolding, and Cell Therapy. Adv. Funct. Mater. 2024, 34, 2307365. [Google Scholar] [CrossRef]
- Muangsanit, P.; Roberton, V.; Costa, E.; Phillips, J.B. Engineered aligned endothelial cell structures in tethered collagen hydrogels promote peripheral nerve regeneration. Acta Biomater. 2021, 126, 224–237. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Zhang, F.; Zheng, Y.; Liu, Z.; Wang, D.; Wei, Z.; Deng, C. Synergistic effect of nanofat and mouse nerve-growth factor for promotion of sensory recovery in anterolateral thigh free flaps. Stem Cells Transl. Med. 2021, 10, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Tong, Z.; Luo, L.H.; Zhao, Y.N.; Chen, F.X.; Li, Y.P.; Huselstein, C.; Ye, Q.F.; Ye, Q.S.; Chen, Y. Comprehensive strategy of conduit guidance combined with VEGF producing Schwann cells accelerates peripheral nerve repair. Bioact. Mater. 2021, 6, 3515–3527. [Google Scholar] [CrossRef] [PubMed]
- Palombella, S.; Guiotto, M.; Higgins, G.C.; Applegate, L.L.; Raffoul, W.; Cherubino, M.; Hart, A.; Riehle, M.O.; di Summa, P.G. Human platelet lysate as a potential clinical-translatable supplement to support the neurotrophic properties of human adipose-derived stem cells. Stem Cell Res. Ther. 2020, 11, 432. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.; Chang, W.; Zhou, X.Q.; Chen, Y.F.; Dai, F.T.; Anwar, A.; Yu, X.J. Nanofibrous Nerve Conduits with Nerve Growth Factors and Bone Marrow Stromal Cells Pre-Cultured in Bioreactors for Peripheral Nerve Regeneration. ACS Appl. Mater. Interfaces 2020, 12, 16168–16177. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; He, Y.; Jin, L.; Zhang, Y.; Guastaldi, F.P.; Albashari, A.A.; Hu, F.; Wang, X.; Wang, L.; Xiao, J.; et al. Application of bioactive hydrogels combined with dental pulp stem cells for the repair of large gap peripheral nerve injuries. Bioact. Mater. 2021, 6, 638–654. [Google Scholar] [CrossRef] [PubMed]
- Lavorato, A.; Raimondo, S.; Boido, M.; Muratori, L.; Durante, G.; Cofano, F.; Vincitorio, F.; Petrone, S.; Titolo, P.; Tartara, F.; et al. Mesenchymal Stem Cell Treatment Perspectives in Peripheral Nerve Regeneration: Systematic Review. Int. J. Mol. Sci. 2021, 22, 572. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Jeon, J.; Kim, B.; Lee, M.S.; Park, S.; Lim, J.; Yi, J.; Lee, H.; Yang, H.S.; Lee, J.Y. Electrically Conductive Hydrogel Nerve Guidance Conduits for Peripheral Nerve Regeneration. Adv. Funct. Mater. 2020, 30, 2003759. [Google Scholar] [CrossRef]
- Chu, X.L.; Song, X.Z.; Li, Q.; Li, Y.R.; He, F.; Gu, X.S.; Ming, D. Basic mechanisms of peripheral nerve injury and treatment via electrical stimulation. Neural Regen. Res. 2022, 17, 2185–2193. [Google Scholar] [CrossRef]
- Song, S.; McConnell, K.W.; Amores, D.; Levinson, A.; Vogel, H.; Quarta, M.; Rando, T.A.; George, P.M. Electrical stimulation of human neural stem cells via conductive polymer nerve guides enhances peripheral nerve recovery. Biomaterials 2021, 275, 120982. [Google Scholar] [CrossRef]
- He, L.; Xiao, Q.; Zhao, Y.; Li, J.; Reddy, S.; Shi, X.; Su, X.; Chiu, K.; Ramakrishna, S. Engineering an Injectable Electroactive Nanohybrid Hydrogel for Boosting Peripheral Nerve Growth and Myelination in Combination with Electrical Stimulation. ACS Appl. Mater. Interfaces 2020, 12, 53150–53163. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yin, X.; Wang, H.; Qiu, W.; Li, L.; Li, F.; Shan, Y.; Zhao, Z.; Li, Z.; Guo, J.; et al. Engineering a wirelessly self-powered and electroconductive scaffold to promote peripheral nerve regeneration. Nano Energy 2023, 107, 108145. [Google Scholar] [CrossRef]
- Wang, Q.Q.; Wang, H.; Ma, Y.; Cao, X.D.; Gao, H.C. Effects of electroactive materials on nerve cell behaviors and applications in peripheral nerve repair. Biomater. Sci. 2022, 10, 6061–6076. [Google Scholar] [CrossRef] [PubMed]



| Therapeutic Regimen | Methods | Objectives | Advantages | Disadvantages |
|---|---|---|---|---|
| Nonsurgical treatment |
| Relieve the pain symptoms of patients |
|
|
| Surgical treatment |
|
|
|
|
| Tissue-engineered materials |
|
|
| Development of a nerve repair material that aligns with the microenvironment of peripheral nerve regeneration, which requires further exploration |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wan, T.; Li, Q.-C.; Qin, M.-Y.; Wang, Y.-L.; Zhang, F.-S.; Zhang, X.-M.; Zhang, Y.-C.; Zhang, P.-X. Strategies for Treating Traumatic Neuromas with Tissue-Engineered Materials. Biomolecules 2024, 14, 484. https://doi.org/10.3390/biom14040484
Wan T, Li Q-C, Qin M-Y, Wang Y-L, Zhang F-S, Zhang X-M, Zhang Y-C, Zhang P-X. Strategies for Treating Traumatic Neuromas with Tissue-Engineered Materials. Biomolecules. 2024; 14(4):484. https://doi.org/10.3390/biom14040484
Chicago/Turabian StyleWan, Teng, Qi-Cheng Li, Ming-Yu Qin, Yi-Lin Wang, Feng-Shi Zhang, Xiao-Meng Zhang, Yi-Chong Zhang, and Pei-Xun Zhang. 2024. "Strategies for Treating Traumatic Neuromas with Tissue-Engineered Materials" Biomolecules 14, no. 4: 484. https://doi.org/10.3390/biom14040484
APA StyleWan, T., Li, Q.-C., Qin, M.-Y., Wang, Y.-L., Zhang, F.-S., Zhang, X.-M., Zhang, Y.-C., & Zhang, P.-X. (2024). Strategies for Treating Traumatic Neuromas with Tissue-Engineered Materials. Biomolecules, 14(4), 484. https://doi.org/10.3390/biom14040484