Abstract
(1) Background: The purpose of this systematic review was to determine the prevalence of bone bruises in patients with anterior cruciate ligament (ACL) injuries and the location of the bruises relative to the tibia and femur. Understanding the relative positions of these bone bruises could enhance our comprehension of the knee loading patterns that occur during an ACL injury. (2) Methods: The MEDLINE, EMBASE, and the Cochrane Library databases were searched for studies that evaluated the presence of bone bruises following ACL injuries. Study selection, data extraction, and a systematic review were performed. (3) Results: Bone bruises were observed in 3207 cases (82.8%) at the lateral tibia plateau (LTP), 1608 cases (41.5%) at the medial tibia plateau (MTP), 2765 cases (71.4%) at the lateral femoral condyle (LFC), and 1257 cases (32.4%) at the medial femoral condyle (MFC). Of the 30 studies, 11 were able to assess the anterior to posterior direction. The posterior LTP and center LFC were the most common areas of bone bruises. Among the 30 studies, 14 documented bone bruises across all four sites (LTP, MTP, LFC, and MFC). The most common pattern was bone bruises appearing at the LTP and LFC. (4) Conclusions: The most frequently observed pattern of bone bruises was restricted to the lateral aspects of both the tibia and femur. In cases where bone bruises were present on both the lateral and medial sides, those on the lateral side exhibited greater severity. The positioning of bone bruises along the front–back axis indicated a forward shift of the tibia in relation to the femur during ACL injuries.
1. Introduction
The anterior cruciate ligament (ACL) is essential for knee stabilization, preventing the tibia from moving forward relative to the femur, especially during activities requiring abrupt stops and directional changes [1,2]. The ACL plays a pivotal role in knee stability, working in conjunction with the posterior cruciate ligament to form an X-shaped structure inside the knee [1,2]. This configuration is essential in limiting excessive the forward movement of the tibia and contributing to the knee’s rotational equilibrium, especially under side-to-side (varus or valgus) stresses [3,4,5,6]. An ACL tear is among the most frequently observed and severe injuries in sports [7,8]. ACL tears are among the most prevalent ligament injuries of the knee in the United States, with an estimated annual occurrence rate of 68.6 per 100,000 people [9]. In Norway, there were 34 ACL injuries per 100,000 individuals [10], while Denmark reported 38 ACL injuries per 100,000 people [11], and Sweden saw 32 ACL injuries per 100,000 people [12]. The number of ACL tears in South Korea is increasing [13]. The expense of surgical repair, the duration of recovery, and the potential for lasting impairment have sparked considerable interest in preventing ACL injuries [14,15,16]. To prevent these injuries, it is essential to understand the mechanisms behind ACL injuries and to identify their risk factors [17,18].
Bone bruising, also known as subchondral bone marrow edema or edema-like marrow signal intensity, is detected via MRI scans in more than 80% of acute ACL injury cases [19,20]. Such bruises are thought to emerge from inflammation, swelling, and tiny fractures within the bone’s trabeculae due to the compressive forces between the femur and tibia during injury [21]. These bruises on the tibiofemoral joint serve as a ‘footprint’ that reflects the dynamics within the joint at the moment of the ACL tear, offering clues to the movements leading to the injury [22]. Femoral and tibial bone bruises are believed to mark the point of impact at the moment of injury, providing clues on how an ACL injury occurs [23,24].
The literature frequently documents the pattern of these bruises in cases of ACL injuries, often associating them with a mix of anterior tibial displacement, valgus stress, and either an internal or external rotation of the tibia [25,26,27]. Earlier research showed that bone bruises associated with ACL injuries occur most frequently in the lateral compartment, suggesting that a valgus force is the main cause of such injuries [28]. Alternatively, some studies have suggested that the primary mechanism behind an ACL injury could be the anterior translation of the tibia with minimal bending of the knee, as inferred from bone bruises found on the back of the tibia and the front of the femur [26,29].
While numerous investigations have explored the locations of bone bruises on the femur and tibia in individuals with ACL tears, studies have typically addressed the prevalence and sites of bone bruises on the tibia and femur in isolation for patients with ACL injuries [26,29]. There is limited knowledge about the comparative locations of bone bruises on the tibia and femur [26,29]. Additionally, most studies only focus on the medial to lateral direction of the tibia and femur at the bone bruise location, and there is a lack of research on the anterior to posterior direction [27,30]. Understanding the relative positions of these bone bruises could enhance our comprehension of the loading patterns during an ACL injury [27]. The purpose of this systematic review was to determine the prevalence of bone bruises in patients with ACL injuries and the common knee loading patterns that occur during ACL injuries based on the location of the bone bruises on the tibia and femur.
2. Materials and Methods
This study was performed following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement (S1 PRISMA Checklist) [31].
2.1. Data and Literature Sources
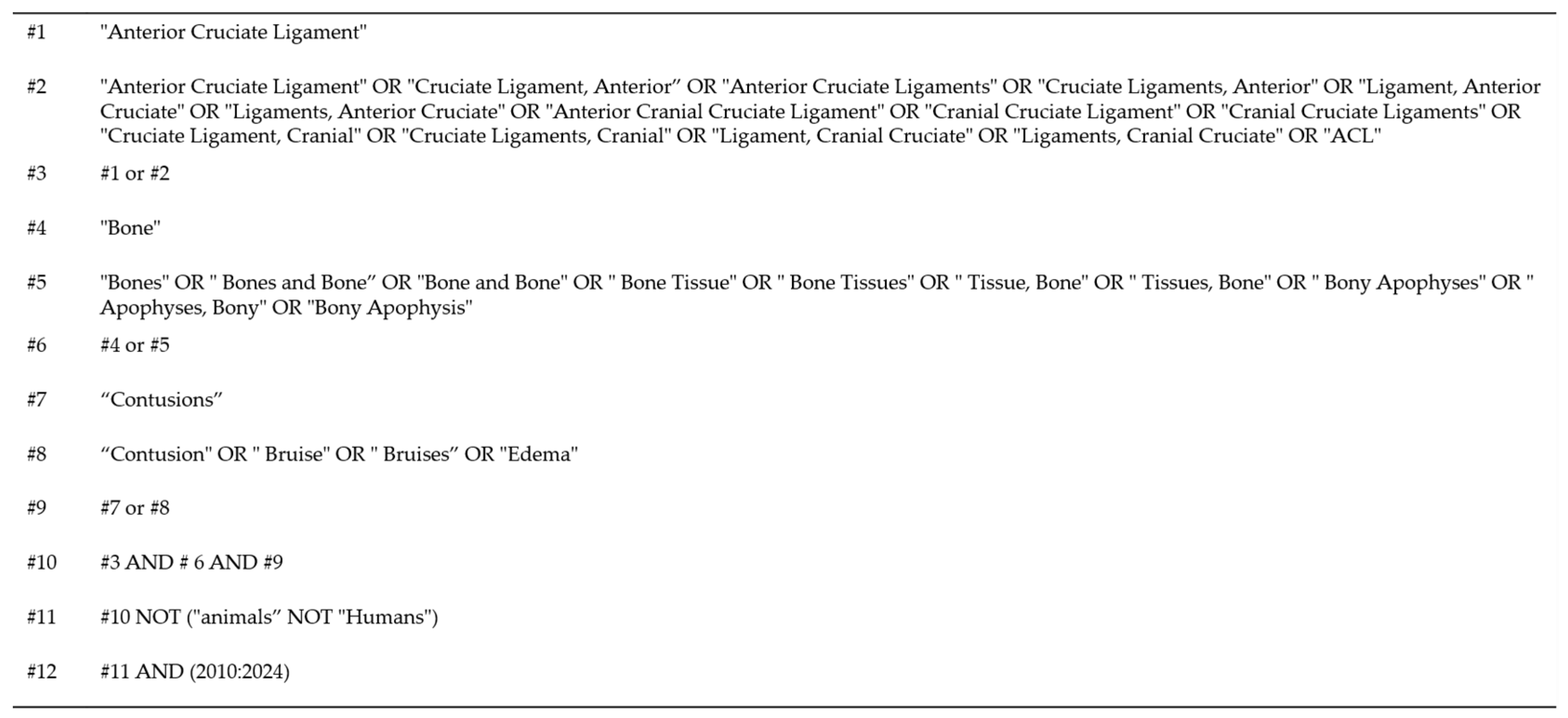
This study was performed in accordance with the Cochrane Review’s methods. Multiple comprehensive databases (MEDLINE, EMBASE, and the Cochrane Library) were searched in January 2024 for studies in English that evaluated bone bruises following ACL injuries (S1 Search Strategy). The search terms were as follows: “(bone OR osseous) AND (bruise OR contusion OR lesion OR edema) AND (anterior cruciate ligament OR ACL)” (Figure 1). Following the initial electronic search, reference lists and bibliographies of the discovered articles, including pertinent reviews and meta-analyses, were manually searched to identify trials potentially overlooked in the electronic search. Each identified article was then evaluated individually for inclusion.
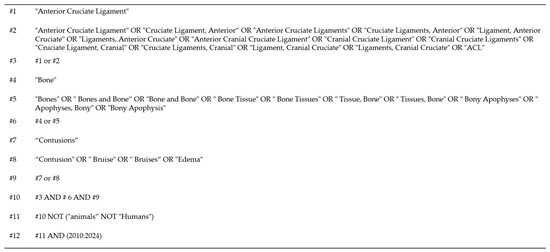
Figure 1.
Search strategy for systematic review of bone bruise patterns following anterior cruciate ligament tears.
2.2. Study Selection
Study inclusion was independently assessed by two reviewers in accordance with the established selection criteria. Titles and abstracts were initially reviewed for relevance. When there was uncertainty, the complete article was examined to decide its eligibility. Any differences in opinion were settled through discussion. The articles were included based on the following criteria: the research must have involved more than 15 human participants with ACL injuries; utilized MRI technology to evaluate bone bruises; documented the location of these bruises in at least one of the following compartments: the medial or lateral compartment of the femur, specifically the medial femoral condyle (MFC) or lateral femoral condyle (LFC), and the medial or lateral compartment of the tibia, specifically the medial tibial plateau (MTP) or lateral tibial plateau (LTP); and provided details on the prevalence of such injuries. All ACL injuries were included regardless of the ACL injury mechanism. Additionally, only articles written in English and published between 2010 and 2023 were eligible. The exclusion criteria eliminated case studies, systematic reviews without original data, research that only indicated the maximum occurrence and prevalence of bone bruises without identifying the specific knee compartment, and studies that used cadaveric models to investigate ACL injuries.
2.3. Data Extraction
Two reviewers independently extracted data from each study using a standardized data extraction form. Disagreements were resolved via discussion, and those unresolved through discussion were reviewed by a third reviewer. The following variables were included: the first author, publication year, country, study type, timing of MRI relative to injury, MRI intensity, total ACL injury sample size, and bone bruise sample size. The bone bruise pattern was primarily characterized by distinguishing between the medial and lateral compartments of the tibia and femur, denoted as LTP, MTP, LFC, and MFC. Additionally, in cases where bone bruises could be identified from the anterior to the posterior direction, they were categorized as anterior, central, or posterior. Given that bone bruises can appear in one or multiple locations, the number of occurrence sites was recorded (from one to four areas, encompassing LTP, MTP, LFC, and MFC). We attempted to contact the study authors for supplementary information when there were insufficient or missing data in the articles. The third senior investigator was consulted to resolve any disagreement during data extraction.
3. Results
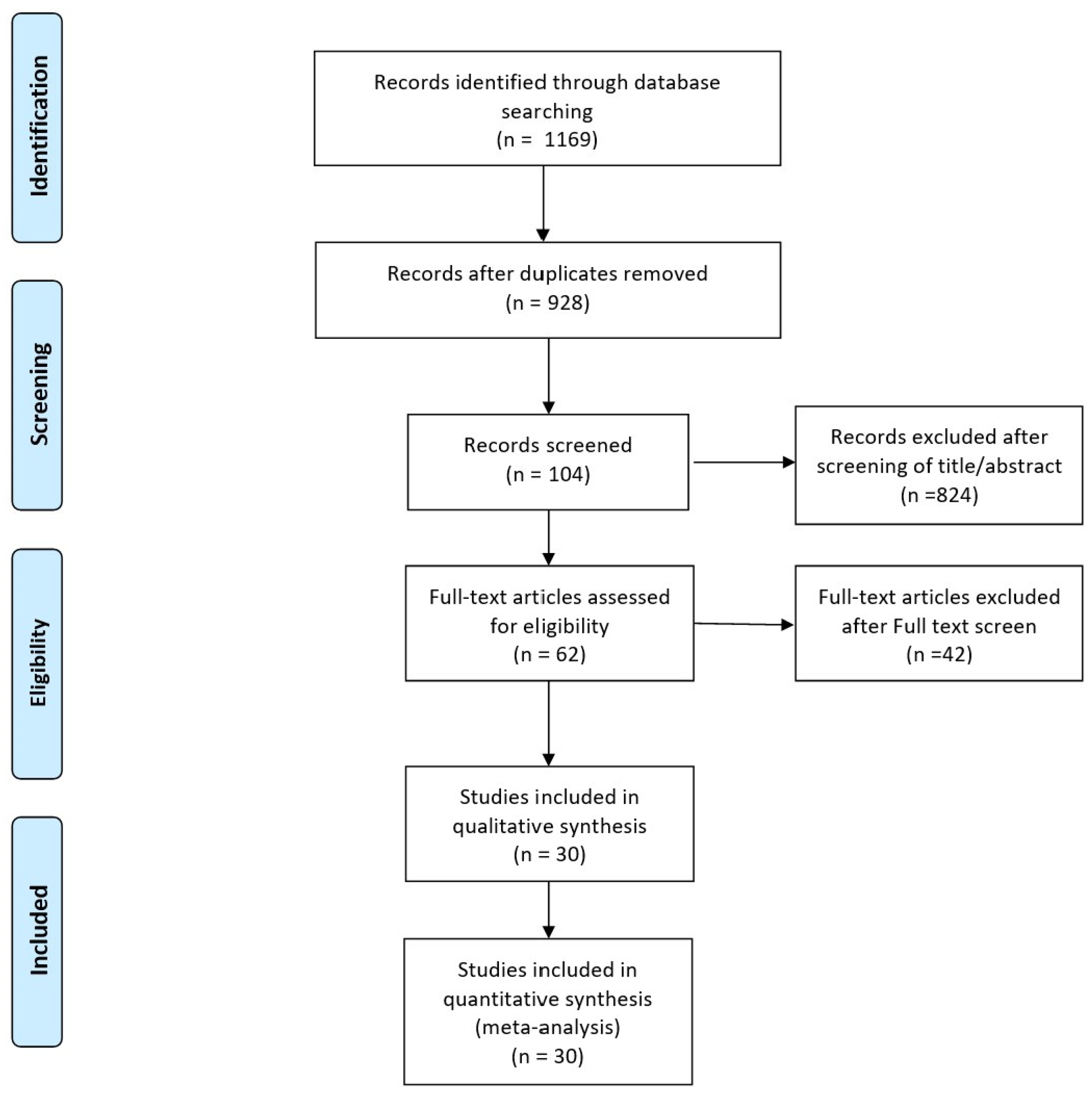
A study flow diagram showing the process for study identification, inclusion, and exclusion is provided (Figure 2). The initial electronic search yielded 1169 studies. Three additional publications were obtained through manual searching. In total, 104 potentially eligible studies were assessed for inclusion after screening the titles and abstracts. After we reviewed the full texts, an additional 42 studies were excluded, leaving 30 studies for the final analysis.
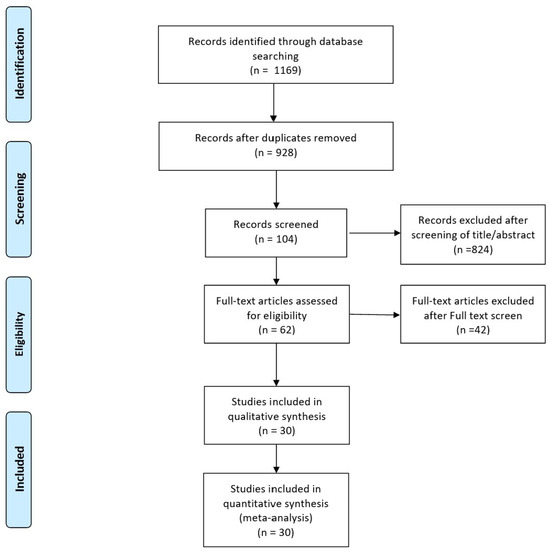
Figure 2.
Flowchart illustrating the literature search process.
The study characteristics are summarized in Table 1. All studies were retrospective, and most were conducted in the United States or China. The shortest time from injury to MRI measurement was 3 weeks, while the longest was 90 days or 3 months. The total ACL sample size was 3872, of which 3288 cases had bone bruises (84.9%).

Table 1.
Characteristics of included studies.
In the 30 studies included in this research, all recorded the prevalence of bone bruises in the LTP, MTP, LFC, and MFC. Among 3872 cases of ACL injury, bone bruises were observed in 3207 at the LTP (82.8%), 1608 at the MTP (41.5%), 2765 at the LFC (71.4%), and 1257 at the MFC (32.4%). The highest occurrence of bone bruises was noted at the LTP, while the lowest was at the MFC (Table 2). Of the 30 studies, 11 were able to assess the anterior to posterior direction. In total, 1115 bone bruises were reported to have occurred in the lateral compartment of the tibial plateau. Among these, 37 (3.3%) occurred in the anterior section, 136 (12.3%) in the central section, and 942 (84.4%) in the posterior section. Similarly, 568 bone bruises in the medial compartment of the tibial plateau were noted in the same set of studies, with 35 (6.1%) in the anterior, 56 (9.9%) in the central, and 477 (84.0%) in the posterior sections. Furthermore, 994 bone bruises in the LFC were documented in the selected studies, with 107 (10.8%) in the anterior, 844 (84.9%) in the central, and 43 (4.3%) in the posterior sections. Additionally, the MFC had 649 reported bone bruises, with 52 (8.0%) in the anterior, 520 (80.1%) in the central, and 77 (11.9%) in the posterior sections (Table 3).
Table 2.
Bone bruise prevalence in medial and lateral compartments of femur and tibia.
Table 3.
Bone bruise prevalence in the anterior and posterior directions in the medial and lateral compartments of the femur and tibia.
Among the 30 studies, 14 documented bone bruises across all four sites (LTP, MTP, LFC, and MFC). The most commonly occurring event was bone bruising in two of the four sites (857 cases), followed by occurrences in three sites (439 cases), one site (382 cases), and all four sites (366 cases). Among cases where bone bruising appeared in only one site, there were 152 cases at the LTP, 144 cases at the LFC, 37 cases at the MTP, and 49 cases at the MFC. The most frequent occurrence of bone bruising in two sites was observed in the LTP and LFC (541 cases), followed by the MFC and MTP (129 cases) and the LTP and MTP (114 cases). When bone bruises were found in three sites, they occurred predominantly in the LTP, LFC, and MTP (340 cases), and in the LTP, LFC, and MFC (81 cases) (Table 4).
Table 4.
Summary of the distribution of bone bruises in the medial and lateral compartments of the femur and tibia.
4. Discussion
The findings of this study offer insights into the locations of bone bruises, in particular, sections of the tibia and femur. Our data indicate that the most prevalent pattern of bone bruising was on the lateral aspects of both the femur and tibia, which could enhance our comprehension of the loading dynamics involved in ACL injuries.
Bone bruises were most common in the LTP and LFC, and when examined in the antero-posterior direction, the posterior LTP and center LFC showed the most frequent occurrence of bone bruises. This suggests that collisions between the LFC and the LTP are more common than those between the MFC and the MTP at the time of injury. The predominance of lateral compartment bruising over medial compartment bruising in ACL injuries observed in this study corroborates the results of earlier studies on ACL bone bruises [18,20,30,35,37,40,44,46,51,53,55]. The higher incidence of bone bruises in the lateral compartments could indicate the application of valgus force during an ACL injury, leading to an “opening” effect on the medial side. This observation aligns with prior research indicating that a valgus load is the main cause of ACL injuries [22,28,37].
The findings of this study indicate that an anterior translation of the tibia in relation to the femur occurs during ACL injuries, as evidenced by the frequency and placement of bone bruises. The data reveal that, in all the predominant bone bruise patterns identified in this study, bruises on the tibia were located in the posterior region, while those on the femur were found in the central region, aligning with previous studies that utilized MRI to examine bone bruise patterns [56]. These outcomes imply that, during injury, the central or front part of the femoral condyle likely made contact with the posterior part of the tibial plateau, suggesting significant anterior movement of the tibia relative to the femur during ACL injury [57,58]. For such high-energy contact to occur, the posterior part of the tibia must move forward relative to the femur on both sides. This pattern of bruising in the sagittal plane aligns with findings from previous studies that have documented the anterior translation of the tibia [18,26,48].
Furthermore, recent studies have recorded considerable anterior movement of the tibia in patients at the presumed moment of injury [22,59]. Given the ACL’s role as a primary barrier against anterior shear stress, significant anterior movement of the tibia could generate substantial anterior shear forces, leading to an ACL injury [27]. Thus, these combined findings indicate that anterior shear force in the sagittal plane may be a critical risk factor for ACL injuries [27].
The variation in bruising patterns along the sagittal plane of the MFC and LFC sheds light on the tibia’s rotation, either internally or externally, during injury [18,21,26,60]. While the exact position of the tibia relative to that of the femur (internally or externally rotated) at the time of injury cannot be directly deduced from the bone bruise locations, the uneven distribution in the front–back direction between the lateral and medial sides implies that there was rotation of the tibia around its long axis during the ACL injury [26,60]. Bone bruises in the anterior portion of the LFC are not significantly more frequently observed than are those in the anterior portion of the MFC, but they do occur more often. If the tibia were to translate anteriorly without any rotation, we would expect to see similar bruising patterns on the MFC and LFC [18,26]. However, anterior translation combined with internal rotation of the tibia leads to contact of the posterior region of the LTP with the LFC more anteriorly compared with the interaction between the MTP and the MFC. This is because the internal rotation of the tibia brings the posterior part of the LTP forward [18,21,26,60]. However, since the frequency difference is not substantial, it cannot be conclusively determined that the internal rotation of the tibia is one of the main mechanisms [61]. This study’s outcomes indicate that the pattern of ACL injury is intricate, involving a complex, multi-directional loading pattern rather than a simple, single-plane loading pattern [61].
Additionally, the bone bruise patterns highlighted in this review suggest knee hyperextension as another potential mechanism for non-contact ACL injuries. The data revealed that 3.5% of bone bruises in the LTP and 6.8% in the MTP were in the anterior regions, hinting at possible knee hyperextension in some ACL injury scenarios. It is plausible that some of the anterior femoral condyle bone bruises reported in the included studies could be attributed to this mechanism of injury [23,62]. There is relatively limited literature on hyperextension injuries associated with ACL injuries and bone bruise patterns [23,62]. However, several authors suggest that the typical pattern involves anterior tibial bruises, sometimes accompanied by anterior femoral bruises, which occur due to direct impact of the structures during the injury. These injuries may occur as a result of actions such as extreme force on the tibia with a planted foot or a forceful kick [23].
Despite the thorough comparisons and analyses, this study faced several constraints. First, a widespread issue with systematic reviews is that the caliber of the original data can restrict the overall quality of the research. All studies were retrospective. Hence, there is a need for more prospective research in this field. Second, the inclusion of only published data might introduce a reporting bias, given that negative outcomes are less frequently disclosed. Third, there is the issue of population diversity among the studies reviewed. Although all studies provided data on bone bruises in subjects with ACL injuries, many studies also included subjects who experienced concurrent injuries to ligaments and the meniscus. As a result, the ability of any given study to determine whether bone contusions are solely due to ACL injury or whether concurrent ligamentous and/or meniscus injuries may influence the injury pattern is limited. Fourth, only research results from 2010 onwards were included. It is believed that more appropriate results can be obtained if results prior to 2010 are included [21,27]. Finally, no classification was made regarding gender (men and women) [44], age (pediatrics and adults) [32,33], or injury type (contact or non-contact injury) [19]. Although these factors can have a significant impact on the pattern of bone bruising, they could not be distinguished clearly using the data included in this study, so they were expressed in an integrated manner.
5. Conclusions
The most frequently observed pattern of bone bruises was restricted to the lateral aspects of both the tibia and femur. In cases where bone bruises were present on both the lateral and medial sides, those on the lateral side exhibited greater severity. The positioning of bone bruises along the front–back axis indicated a forward shift of the tibia in relation to the position of the femur during an ACL injury. Knee valgus can occur during an ACL injury, yet the peak occurrence of knee valgus takes place following a significant forward movement of the tibia in comparison to the position of the femur, which is enough to result in an ACL injury.
Author Contributions
M.S.K. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis; concept and design: S.S. and M.S.K.; acquisition, analysis, and interpretation of data: S.M.A. and B.J.H.; drafting of the manuscript: S.S. and M.S.K.; critical revision of the manuscript for important intellectual content: all authors; administrative, technical, and material support: S.M.A. and B.J.H.; supervision: M.S.K. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (RS-2023-00215891) and Research Fund of Seoul St. Mary’s Hospital, The Catholic University of Korea.
Institutional Review Board Statement
Review articles do not require Institutional Review Board (IRB) approval if the data reviewed are public.
Informed Consent Statement
Informed consent was not required.
Data Availability Statement
The data presented in this study are available in the main article.
Conflicts of Interest
There are no relevant conflicts of interest for all authors. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Duthon, V.B.; Barea, C.; Abrassart, S.; Fasel, J.H.; Fritschy, D.; Ménétrey, J. Anatomy of the anterior cruciate ligament. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Krakowski, P.; Nogalski, A.; Jurkiewicz, A.; Karpiński, R.; Maciejewski, R.; Jonak, J. Comparison of diagnostic accuracy of physical examination and MRI in the most common knee injuries. Appl. Sci. 2019, 9, 4102. [Google Scholar] [CrossRef]
- Bae, B.S.; Yoo, S.; Lee, S.H. Ramp lesion in anterior cruciate ligament injury: A review of the anatomy, biomechanics, epidemiology, and diagnosis. Knee Surg. Relat. Res. 2023, 35, 23. [Google Scholar] [CrossRef]
- Helito, C.P.; da Silva, A.G.M.; Guimarães, T.M.; Sobrado, M.F.; Pécora, J.R.; Camanho, G.L. Functional results of multiple revision anterior cruciate ligament with anterolateral tibial tunnel associated with anterolateral ligament reconstruction. Knee Surg. Relat. Res. 2022, 34, 24. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.M.; Bi, A.S.; Kaplan, D.J.; Alaia, M.J.; Strauss, E.J.; Jazrawi, L.M. An eponymous history of the anterolateral ligament complex of the knee. Knee Surg. Relat. Res. 2022, 34, 45. [Google Scholar] [CrossRef]
- Moran, J.; Katz, L.D.; Schneble, C.A.; Li, D.T.; Kahan, J.B.; Wang, A.; Porrino, J.; Fosam, A.; Cheng, R.; Jokl, P.; et al. A Novel MRI Mapping Technique for Evaluating Bone Bruising Patterns Associated with Noncontact ACL Ruptures. Orthop. J. Sports Med. 2022, 10, 23259671221088936. [Google Scholar] [CrossRef]
- Moon, H.S.; Choi, C.H.; Jung, M.; Yoo, J.H.; Kwon, H.J.; Hong, Y.T.; Kim, S.H. Small Intercondylar Notch Size Is Not Associated with Poor Surgical Outcomes of Anatomical Single-Bundle Anterior Cruciate Ligament Reconstructions. Clin. Orthop. Surg. 2024, 16, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Sundararajan, S.R.; Ramakanth, R.; Jha, A.K.; Rajasekaran, S. Outside-in technique versus inside-out semitendinosus graft harvest technique in ACLR: A randomised control trial. Knee Surg. Relat. Res. 2022, 34, 16. [Google Scholar] [CrossRef]
- Sanders, T.L.; Maradit Kremers, H.; Bryan, A.J.; Larson, D.R.; Dahm, D.L.; Levy, B.A.; Stuart, M.J.; Krych, A.J. Incidence of Anterior Cruciate Ligament Tears and Reconstruction: A 21-Year Population-Based Study. Am. J. Sports Med. 2016, 44, 1502–1507. [Google Scholar] [CrossRef]
- Granan, L.P.; Bahr, R.; Steindal, K.; Furnes, O.; Engebretsen, L. Development of a national cruciate ligament surgery registry: The Norwegian National Knee Ligament Registry. Am. J. Sports Med. 2008, 36, 308–315. [Google Scholar] [CrossRef]
- Lind, M.; Menhert, F.; Pedersen, A.B. The first results from the Danish ACL reconstruction registry: Epidemiologic and 2 year follow-up results from 5,818 knee ligament reconstructions. Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Granan, L.P.; Forssblad, M.; Lind, M.; Engebretsen, L. The Scandinavian ACL registries 2004–2007: Baseline epidemiology. Acta Orthop. 2009, 80, 563–567. [Google Scholar] [CrossRef]
- Chung, K.S.; Kim, J.H.; Kong, D.H.; Park, I.; Kim, J.G.; Ha, J.K. An Increasing Trend in the Number of Anterior Cruciate Ligament Reconstruction in Korea: A Nationwide Epidemiologic Study. Clin. Orthop. Surg. 2022, 14, 220–226. [Google Scholar] [CrossRef]
- Brophy, R.H.; Wright, R.W.; Matava, M.J. Cost analysis of converting from single-bundle to double-bundle anterior cruciate ligament reconstruction. Am. J. Sports Med. 2009, 37, 683–687. [Google Scholar] [CrossRef]
- Prodromos, C.C.; Han, Y.; Rogowski, J.; Joyce, B.; Shi, K. A meta-analysis of the incidence of anterior cruciate ligament tears as a function of gender, sport, and a knee injury-reduction regimen. Arthroscopy 2007, 23, 1320–1325. [Google Scholar] [CrossRef]
- von Porat, A.; Roos, E.M.; Roos, H. High prevalence of osteoarthritis 14 years after an anterior cruciate ligament tear in male soccer players: A study of radiographic and patient relevant outcomes. Ann. Rheum. Dis. 2004, 63, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.G.; Lee, D.W.; Bae, K.C.; Choi, B.C.; Yang, S.J.; Cho, S.I.; Kim, D.H. Correlation of Y Balance with Clinical Scores and Functional Tests after Anterior Cruciate Ligament Reconstruction in Young and Middle-Aged Patients. Clin. Orthop. Surg. 2023, 15, 50–58. [Google Scholar] [CrossRef]
- Shi, H.; Ding, L.; Jiang, Y.; Zhang, H.; Ren, S.; Hu, X.; Liu, Z.; Huang, H.; Ao, Y. Bone Bruise Distribution Patterns after Acute Anterior Cruciate Ligament Ruptures: Implications for the Injury Mechanism. Orthop. J. Sports Med. 2020, 8, 2325967120911162. [Google Scholar] [CrossRef]
- Moran, J.; Lee, M.S.; Kunze, K.N.; Green, J.S.; Katz, L.D.; Wang, A.; McLaughlin, W.M.; Gillinov, S.M.; Jimenez, A.E.; Hewett, T.E.; et al. Examining the Distribution of Bone Bruise Patterns in Contact and Noncontact Acute Anterior Cruciate Ligament Injuries. Am. J. Sports Med. 2023, 51, 1155–1161. [Google Scholar] [CrossRef]
- Vermeijden, H.D.; Yang, X.A.; Mintz, D.N.; Rademakers, M.V.; van der List, J.P.; Kerkhoffs, G.; DiFelice, G.S. Age and Bone Bruise Patterns Predict Tear Location in the Anterior Cruciate Ligament. Arthrosc. Sports Med. Rehabil. 2023, 5, e41–e50. [Google Scholar] [CrossRef]
- Patel, S.A.; Hageman, J.; Quatman, C.E.; Wordeman, S.C.; Hewett, T.E. Prevalence and location of bone bruises associated with anterior cruciate ligament injury and implications for mechanism of injury: A systematic review. Sports Med. 2014, 44, 281–293. [Google Scholar] [CrossRef]
- Kim, S.Y.; Spritzer, C.E.; Utturkar, G.M.; Toth, A.P.; Garrett, W.E.; DeFrate, L.E. Knee Kinematics during Noncontact Anterior Cruciate Ligament Injury as Determined From Bone Bruise Location. Am. J. Sports Med. 2015, 43, 2515–2521. [Google Scholar] [CrossRef]
- Sanders, T.G.; Medynski, M.A.; Feller, J.F.; Lawhorn, K.W. Bone contusion patterns of the knee at MR imaging: Footprint of the mechanism of injury. Radiographics 2000, 20, S135–S151. [Google Scholar] [CrossRef] [PubMed]
- Speer, K.P.; Warren, R.F.; Wickiewicz, T.L.; Horowitz, L.; Henderson, L. Observations on the injury mechanism of anterior cruciate ligament tears in skiers. Am. J. Sports Med. 1995, 23, 77–81. [Google Scholar] [CrossRef]
- Shi, H.; Ding, L.; Ren, S.; Jiang, Y.; Zhang, H.; Hu, X.; Huang, H.; Ao, Y. Prediction of Knee Kinematics at the Time of Noncontact Anterior Cruciate Ligament Injuries Based on the Bone Bruises. Ann. Biomed. Eng. 2021, 49, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Viskontas, D.G.; Giuffre, B.M.; Duggal, N.; Graham, D.; Parker, D.; Coolican, M. Bone bruises associated with ACL rupture: Correlation with injury mechanism. Am. J. Sports Med. 2008, 36, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Hacke, J.D.; Garrett, W.E.; Liu, H.; Yu, B. Bone Bruises Associated with Anterior Cruciate Ligament Injury as Indicators of Injury Mechanism: A Systematic Review. Sports Med. 2019, 49, 453–462. [Google Scholar] [CrossRef]
- Mazzocca, A.D.; Nissen, C.W.; Geary, M.; Adams, D.J. Valgus medial collateral ligament rupture causes concomitant loading and damage of the anterior cruciate ligament. J. Knee Surg. 2003, 16, 148–151. [Google Scholar]
- Wittstein, J.; Vinson, E.; Garrett, W. Comparison between Sexes of Bone Contusions and Meniscal Tear Patterns in Noncontact Anterior Cruciate Ligament Injuries. Am. J. Sports Med. 2014, 42, 1401–1407. [Google Scholar] [CrossRef]
- Aravindh, P.; Wu, T.; Chan, C.X.; Wong, K.L.; Krishna, L. Association of Compartmental Bone Bruise Distribution with Concomitant Intra-articular and Extra-articular Injuries in Acute Anterior Cruciate Ligament Tears after Noncontact Sports Trauma. Orthop. J. Sports Med. 2018, 6, 2325967118767625. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.D.; Zhang, J.; Li, Y.; Li, Z.; Yan, W.; Ao, Y. Classification of Bone Bruises in Pediatric Patients with Anterior Cruciate Ligament Injuries. Orthop. J. Sports Med. 2023, 11, 23259671221144780. [Google Scholar] [CrossRef]
- Orringer, M.; Lau, J.; Feeley, B.; Pandya, N. Bone Bruise Patterns Associated with Pediatric and Adult Anterior Cruciate Ligament Tears Are Different. Arthrosc. Sports Med. Rehabil. 2023, 5, e151–e157. [Google Scholar] [CrossRef] [PubMed]
- Mester, B.; Kröpil, P.; Ohmann, T.; Schleich, C.; Güthoff, C.; Praetorius, A.; Dudda, M.; Schoepp, C. The influence of distribution, severity and volume of posttraumatic bone bruise on functional outcome after ACL reconstruction for isolated ACL injuries. Arch. Orthop. Trauma Surg. 2023, 143, 6261–6272. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Mao, Y.; Wang, D.; Fu, W.; Li, Q.; Tang, X.; Chen, G.; Chen, X.; Yao, L.; You, M.; et al. Correlation between the Location and Distance of Kissing Contusions and Knee Laxity in Acute Noncontact ACL Injury. Am. J. Sports Med. 2023, 51, 3179–3189. [Google Scholar] [CrossRef]
- Galloway, C.; Ward, H.; Higbie, S.; Kleihege, J.; Kumaravel, M.; Lowe, W.R.; Bailey, L. Relationship between Bone Bruise Volume and Patient Outcomes after ACL Reconstruction. Orthop. J. Sports Med. 2023, 11, 23259671221146205. [Google Scholar] [CrossRef] [PubMed]
- Dai, R.; Wu, Y.; Jiang, Y.; Huang, H.; Yan, W.; Shi, H.; Meng, Q.; Ren, S.; Ao, Y. Comparison of Bone Bruise Pattern Epidemiology between Anterior Cruciate Ligament Rupture and Patellar Dislocation Patients-Implications of Injury Mechanism. Bioengineering 2023, 10, 1366. [Google Scholar] [CrossRef]
- D’Hooghe, P.; Grassi, A.; Villa, F.D.; Alkhelaifi, K.; Papakostas, E.; Rekik, R.; Marin, T.; Tosarelli, F.; Zaffagnini, S. The injury mechanism correlation between MRI and video-analysis in professional football players with an acute ACL knee injury reveals consistent bone bruise patterns. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 121–132. [Google Scholar] [CrossRef]
- Brophy, R.H.; Baker, J.C.; Crain, J.M.; Herzog, M.M.; Stollberg, B.; Wojtys, E.M.; Mack, C.D. MRI Findings Associated with Anterior Cruciate Ligament Tears in National Football League Athletes. Orthop. J. Sports Med. 2023, 11, 23259671231169190. [Google Scholar] [CrossRef]
- Kim, Y.; Kubota, M.; Sato, T.; Inui, T.; Ohno, R.; Ishijima, M. A bone bruise at the lateral and medial tibial plateau with an anterior cruciate ligament injury is associated with a meniscus tear. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 2298–2306. [Google Scholar] [CrossRef]
- Byrd, J.M.; Colak, C.; Yalcin, S.; Winalski, C.; Briskin, I.; Farrow, L.D.; Jones, M.H.; Miniaci, A.A.; Parker, R.D.; Rosneck, J.T.; et al. Posteromedial Tibial Bone Bruise after Anterior Cruciate Ligament Injury: An MRI Study of Bone Bruise Patterns in 208 Patients. Orthop. J. Sports Med. 2022, 10, 23259671221120636. [Google Scholar] [CrossRef] [PubMed]
- Agostinone, P.; Di Paolo, S.; Lucidi, G.A.; Dal Fabbro, G.; Grassi, A.; Zaffagnini, S. Severe bicompartmental bone bruise is associated with rotatory instability in anterior cruciate ligament injury. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 1725–1732. [Google Scholar] [CrossRef]
- Qiu, L.; Sheng, B.; Li, J.; Xiao, Z.; Yuan, M.; Yang, H.; Lv, F.; Lv, F. Mechanisms of non-contact anterior cruciate ligament injury as determined by bone contusion location and severity. Quant. Imaging Med. Surg. 2021, 11, 3263–3273. [Google Scholar] [CrossRef]
- Kim-Wang, S.Y.; Scribani, M.B.; Whiteside, M.B.; DeFrate, L.E.; Lassiter, T.E.; Wittstein, J.R. Distribution of Bone Contusion Patterns in Acute Noncontact Anterior Cruciate Ligament-Torn Knees. Am. J. Sports Med. 2021, 49, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Gurry, M.; Hurley, E.T.; Withers, D.; Vioreanu, M.; Moran, R. Posterior tibial bone bruising associated with posterior-medial meniscal tear in patients with acute anterior cruciate ligament injury. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 3633–3637. [Google Scholar] [CrossRef]
- Bordoni, V.; di Laura Frattura, G.; Previtali, D.; Tamborini, S.; Candrian, C.; Cristallo Lacalamita, M.; Del Grande, F.; Filardo, G. Bone Bruise and Anterior Cruciate Ligament Tears: Presence, Distribution Pattern, and Associated Lesions in the Pediatric Population. Am. J. Sports Med. 2019, 47, 3181–3186. [Google Scholar] [CrossRef]
- Novaretti, J.V.; Shin, J.J.; Albers, M.; Chambers, M.C.; Cohen, M.; Musahl, V.; Fu, F.H. Bone Bruise Patterns in Skeletally Immature Patients with Anterior Cruciate Ligament Injury: Shock-Absorbing Function of the Physis. Am. J. Sports Med. 2018, 46, 2128–2132. [Google Scholar] [CrossRef]
- Lattermann, C.; Jacobs, C.A.; Reinke, E.K.; Scaramuzza, E.A.; Huston, L.J.; Dunn, W.R.; Spindler, K.P. Are Bone Bruise Characteristics and Articular Cartilage Pathology Associated with Inferior Outcomes 2 and 6 Years after Anterior Cruciate Ligament Reconstruction? Cartilage 2017, 8, 139–145. [Google Scholar] [CrossRef]
- Berger, N.; Andreisek, G.; Karer, A.T.; Bouaicha, S.; Naraghi, A.; Manoliu, A.; Seifert, B.; Ulbrich, E.J. Association between traumatic bone marrow abnormalities of the knee, the trauma mechanism and associated soft-tissue knee injuries. Eur. Radiol. 2017, 27, 393–403. [Google Scholar] [CrossRef]
- Song, G.Y.; Zhang, H.; Wang, Q.Q.; Zhang, J.; Li, Y.; Feng, H. Bone Contusions after Acute Noncontact Anterior Cruciate Ligament Injury Are Associated with Knee Joint Laxity, Concomitant Meniscal Lesions, and Anterolateral Ligament Abnormality. Arthroscopy 2016, 32, 2331–2341. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Tentoni, F.; Andriolo, L.; Di Martino, A.; Busacca, M.; Di Matteo, B.; Marcacci, M. Anterior cruciate ligament injury: Post-traumatic bone marrow oedema correlates with long-term prognosis. Int. Orthop. 2016, 40, 183–190. [Google Scholar] [CrossRef]
- Bisson, L.J.; Kluczynski, M.A.; Hagstrom, L.S.; Marzo, J.M. A prospective study of the association between bone contusion and intra-articular injuries associated with acute anterior cruciate ligament tear. Am. J. Sports Med. 2013, 41, 1801–1807. [Google Scholar] [CrossRef]
- Yoon, K.H.; Yoo, J.H.; Kim, K.I. Bone contusion and associated meniscal and medial collateral ligament injury in patients with anterior cruciate ligament rupture. J. Bone Jt. Surg. Am. 2011, 93, 1510–1518. [Google Scholar] [CrossRef]
- Jelić, D.; Masulović, D. Bone bruise of the knee associated with the lesions of anterior cruciate ligament and menisci on magnetic resonance imaging. Vojnosanit. Pregl. 2011, 68, 762–766. [Google Scholar] [CrossRef]
- Shi, H.; Ding, L.; Jiang, Y.; Zhang, H.; Ren, S.; Hu, X.; Liu, Z.; Huang, H.; Ao, Y. Comparison between Soccer and Basketball of Bone Bruise and Meniscal Injury Patterns in Anterior Cruciate Ligament Injuries. Orthop. J. Sports Med. 2021, 9, 2325967121995844. [Google Scholar] [CrossRef]
- Fayad, L.M.; Parellada, J.A.; Parker, L.; Schweitzer, M.E. MR imaging of anterior cruciate ligament tears: Is there a gender gap? Skeletal. Radiol. 2003, 32, 639–646. [Google Scholar] [CrossRef]
- Kaplan, P.A.; Walker, C.W.; Kilcoyne, R.F.; Brown, D.E.; Tusek, D.; Dussault, R.G. Occult fracture patterns of the knee associated with anterior cruciate ligament tears: Assessment with MR imaging. Radiology 1992, 183, 835–838. [Google Scholar] [CrossRef]
- Murphy, B.J.; Smith, R.L.; Uribe, J.W.; Janecki, C.J.; Hechtman, K.S.; Mangasarian, R.A. Bone signal abnormalities in the posterolateral tibia and lateral femoral condyle in complete tears of the anterior cruciate ligament: A specific sign? Radiology 1992, 182, 221–224. [Google Scholar] [CrossRef]
- Owusu-Akyaw, K.A.; Kim, S.Y.; Spritzer, C.E.; Collins, A.T.; Englander, Z.A.; Utturkar, G.M.; Garrett, W.E.; DeFrate, L.E. Determination of the Position of the Knee at the Time of an Anterior Cruciate Ligament Rupture for Male Versus Female Patients by an Analysis of Bone Bruises. Am. J. Sports Med. 2018, 46, 1559–1565. [Google Scholar] [CrossRef]
- Pringle, L.; Wissman, R.D. Imaging of Noncontact Anterior Cruciate Ligament Injuries and Associated Bone Marrow Contusion Patterns. J. Knee Surg. 2022, 35, 475–481. [Google Scholar] [CrossRef]
- Quatman, C.E.; Kiapour, A.; Myer, G.D.; Ford, K.R.; Demetropoulos, C.K.; Goel, V.K.; Hewett, T.E. Cartilage pressure distributions provide a footprint to define female anterior cruciate ligament injury mechanisms. Am. J. Sports Med. 2011, 39, 1706–1713. [Google Scholar] [CrossRef]
- Deangelis, J.P.; Spindler, K.P. Traumatic Bone Bruises in the Athlete’s Knee. Sports Health 2010, 2, 398–402. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).