

Healthy and Inclusive Neighbourhoods: A Design Research Toolkit for the Promotion of Healthy Behaviours





Abstract
1. Introduction
1.1. Urban Health, Neighbourhoods, and the Built Environment
- The “Lifetime Neighbourhoods” [33] approach proposes a checklist of questions to understand how to enhance a neighbourhood’s quality, listen to residents’ needs, design accessible and linked environments, promote social networks, and support home quality.
- Forsyth et al. [23] provide checklists based on principles for understanding (i) the process (i.e., exploring neighbourhoods, understanding the needed changes, and implementing the changes) and (ii) the components (i.e., planning for vulnerable people, fostering multiple health dimensions, making places accessible, connecting places, and reducing hazard exposures) to make places healthier.
- The healthy street approach also provides a checklist based on a framework for understanding how to improve the quality of transport through the built environment [16,17]. Ten sets of indicators are presented that focus on observing and analysing aspects of streets, such as the possibility for pedestrians to walk safely, enjoy contexts with things to see, breathe clean air, easily find seats to rest, or be able to cross busy streets safely, just to name a few. All of these aspects are presented as measurable and assessable in both a qualitative way and a quantitative way.
- The City of London Street Accessibility Tool (CoLSAT) [37] provides a series of instructions for designing more comfortable streets based on twelve needs profile segments based on disability categories.
- London [38] introduces the “diagram of seven health targets” as a checklist for understanding how to plan to improve health. They work at the scale of urban planning that should follow the seven health targets (i.e., clean air, contact with nature, social interaction, feeling safe, living somewhere healthy, peace and tranquillity, and regular exercise).
- The Italian Ministry of Health introduced a framework for urban planning with a health lens [39] based on criteria that work as urban planning strategies [7,8,40]. The ministry, by taking suggestions from previous research (cf. [40]), provides criteria to be assessed for understanding how providing an urban health strategy. The criteria are divided into macro-areas: “environment” (air and smells, water, acoustic noise pollution, and ionizing and non-ionizing radiation); “soil and subsoil” (land consumption, soil permeability and water management, geological, hydro-geological, and seismic risk, contaminated sites, and areas with high environmental risk); “sustainability and hygiene of the built environment” (solid waste collection, urban waste collection and disposal, energy, and reduction in emissions); “urban and social development” (residential density, functional and social mixitè, universal design, and social inclusion); “mobility and transport” (street infrastructure network and parking systems, public transportation, and pedestrian and cycling path systems); “outdoor spaces” (outdoor space systems, urban green systems, lighting, and visual comfort).
- The UN-Habitat Urban Lab provides a toolkit [41] for understanding how to design a sustainable neighbourhood where health is an implicit topic.
- The Inclusive Healthy Places Framework [42] proposes drivers and indicators based on four principles focused on the context, process, design and programmes, and fostering conditions.
- The England National Health Service [43] provided the “Putting Health into Place” guidelines to create healthier communities using ten principles divided into sections for understanding the following: (i) citizen needs; (ii) things to design for improving health through places; (iii) developing and providing health care services.
- The “restorative cities” perspective [44] offers a view of how urban design can favour mental health and wellbeing through restorative environments made by equal accesses (inclusive), nature at the core (green), access to water (blue), five senses immersing (sensory), social cohesion (neighbourly), wellbeing through mobility (active), and creativity and play (playable).
Design Thinking, Collaborative Design, and Health
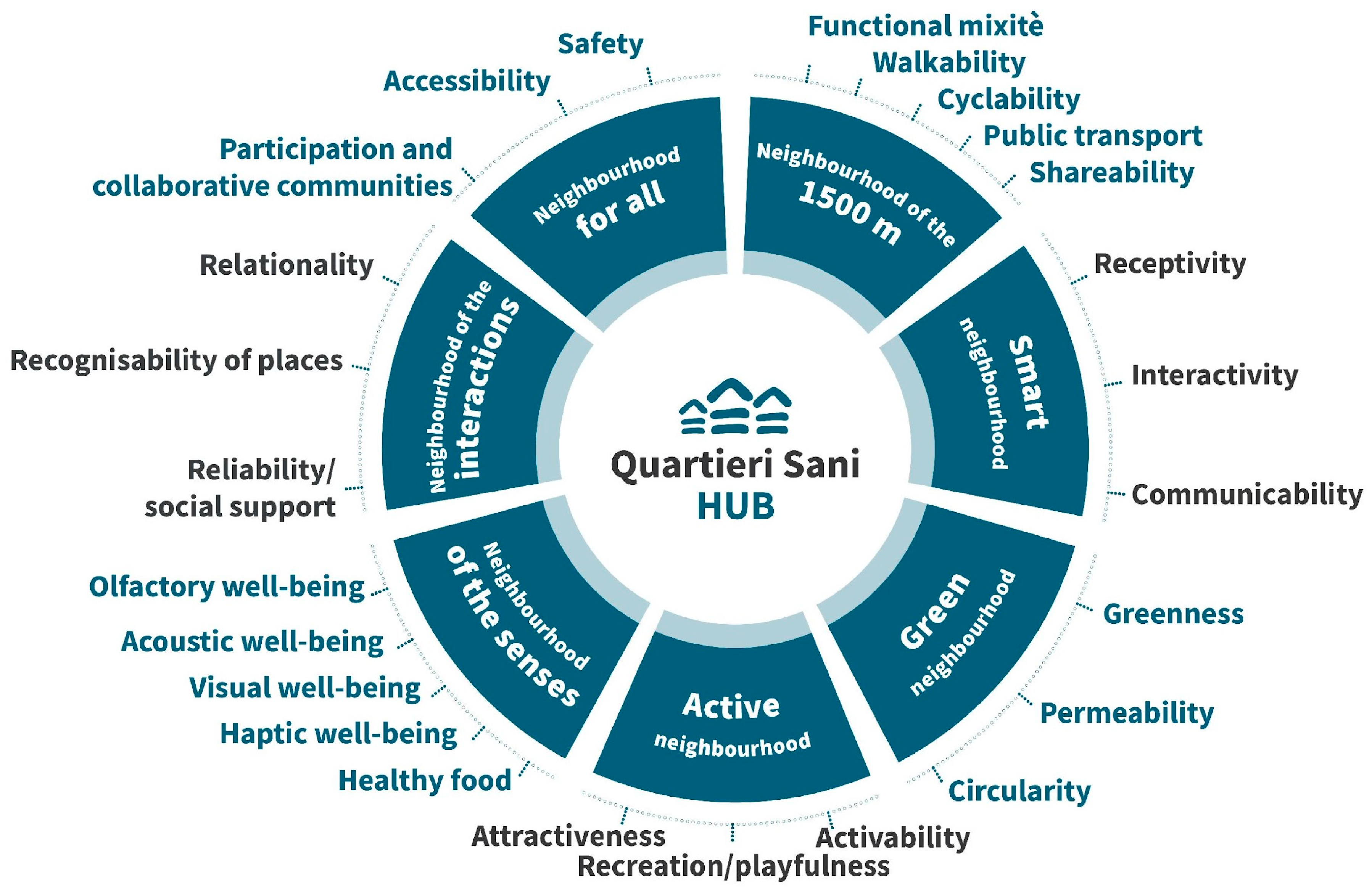
1.2. The HNH Framework
1.3. Significance of the Paper
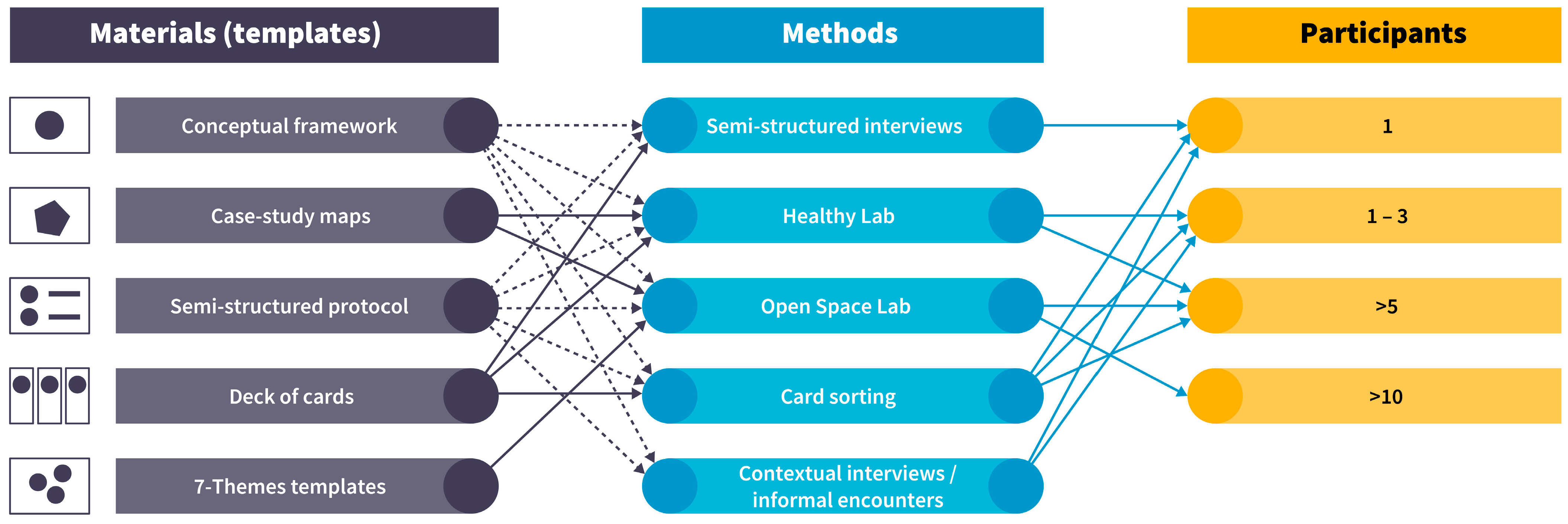
2. Methodological Approach
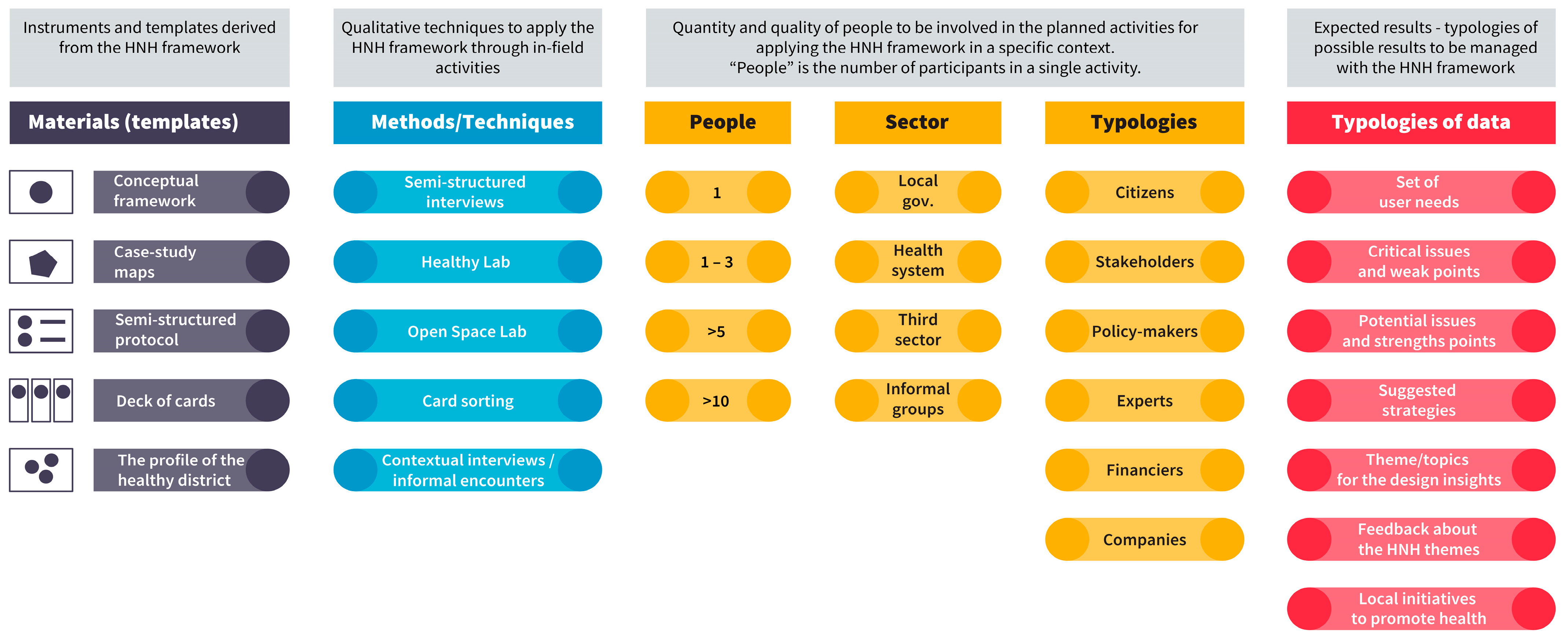
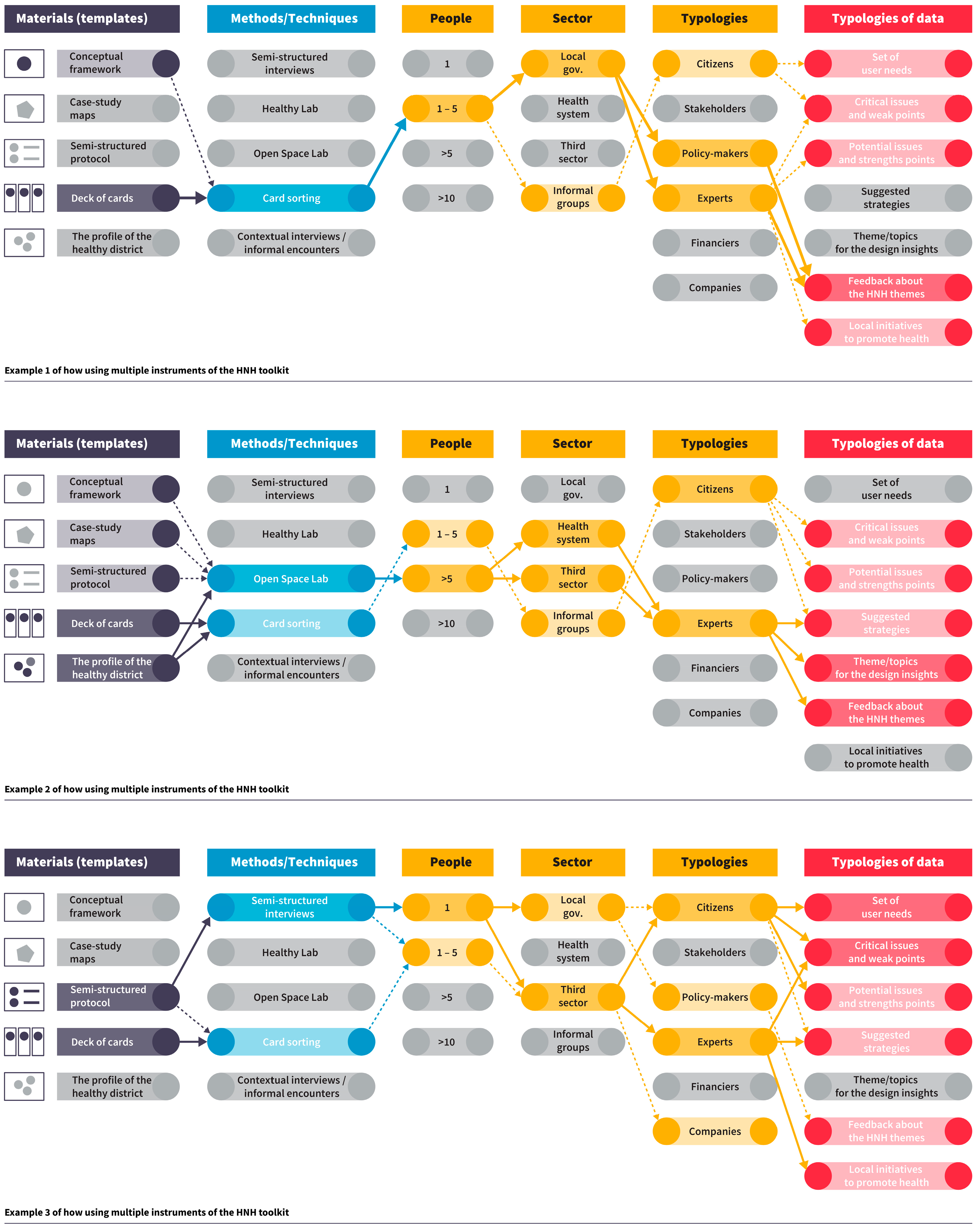
2.1. The HNH Framework as a Design Research Tool
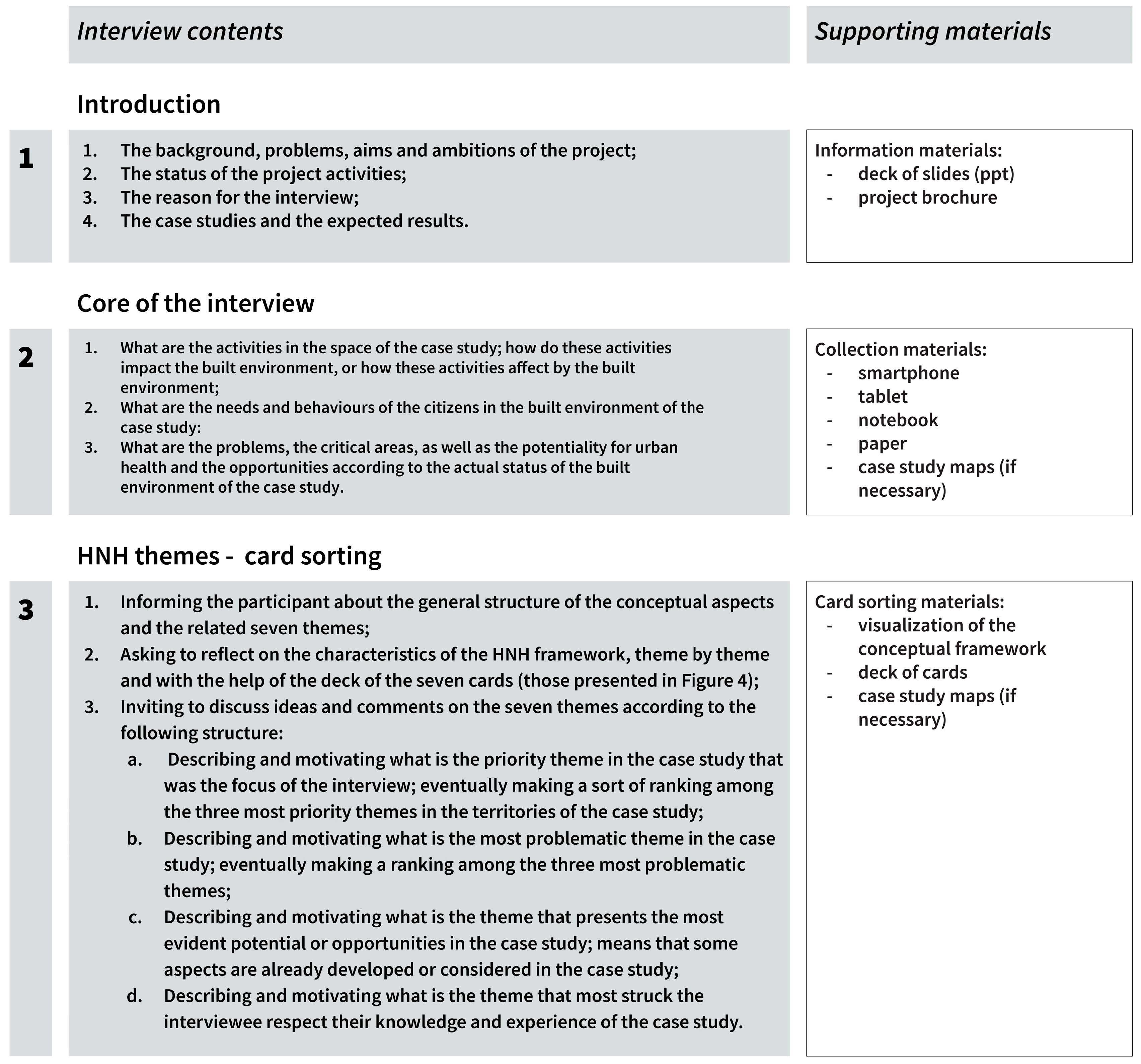
2.1.1. Protocol Design for In-the-Field Activities
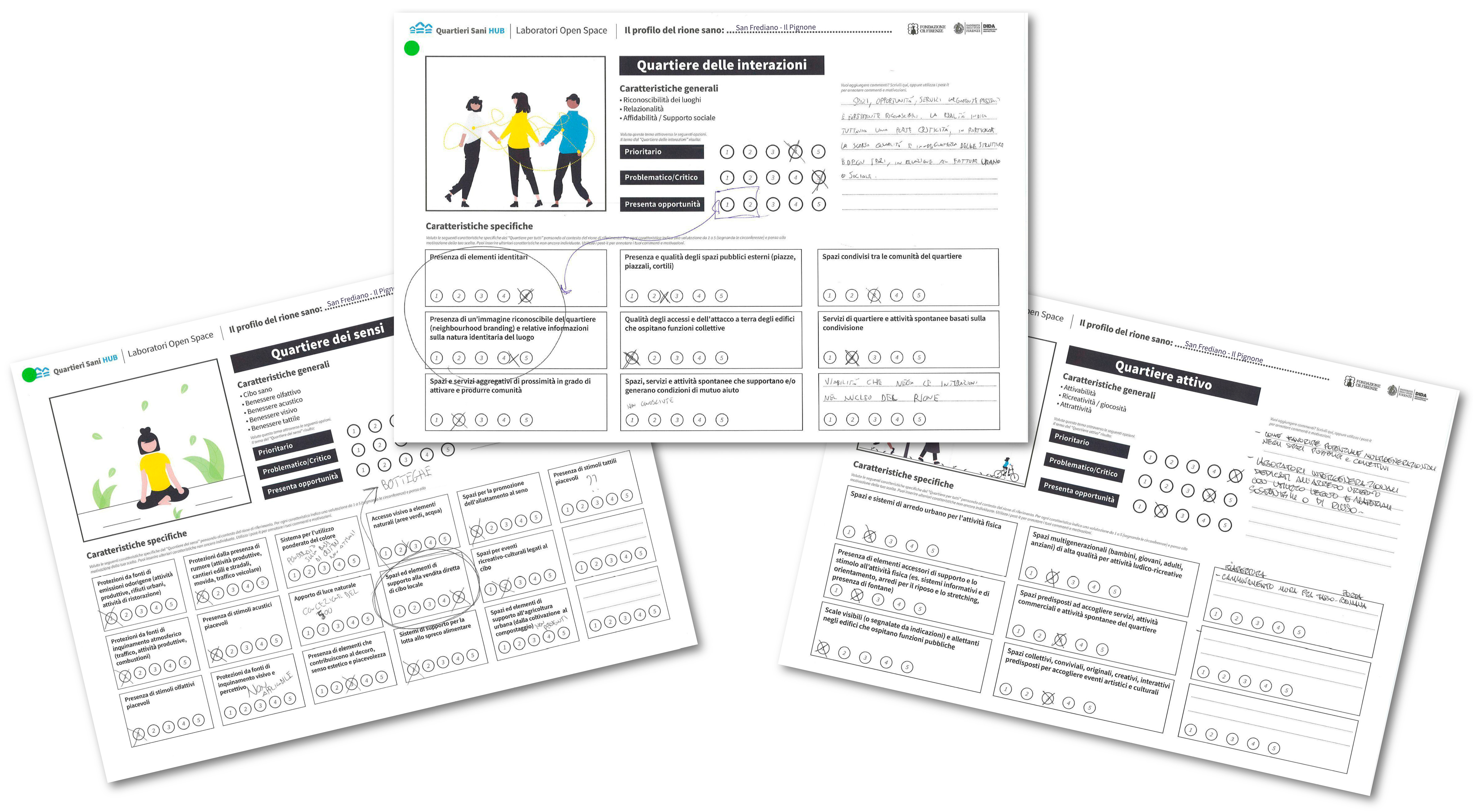
2.1.2. Card Sorting Design
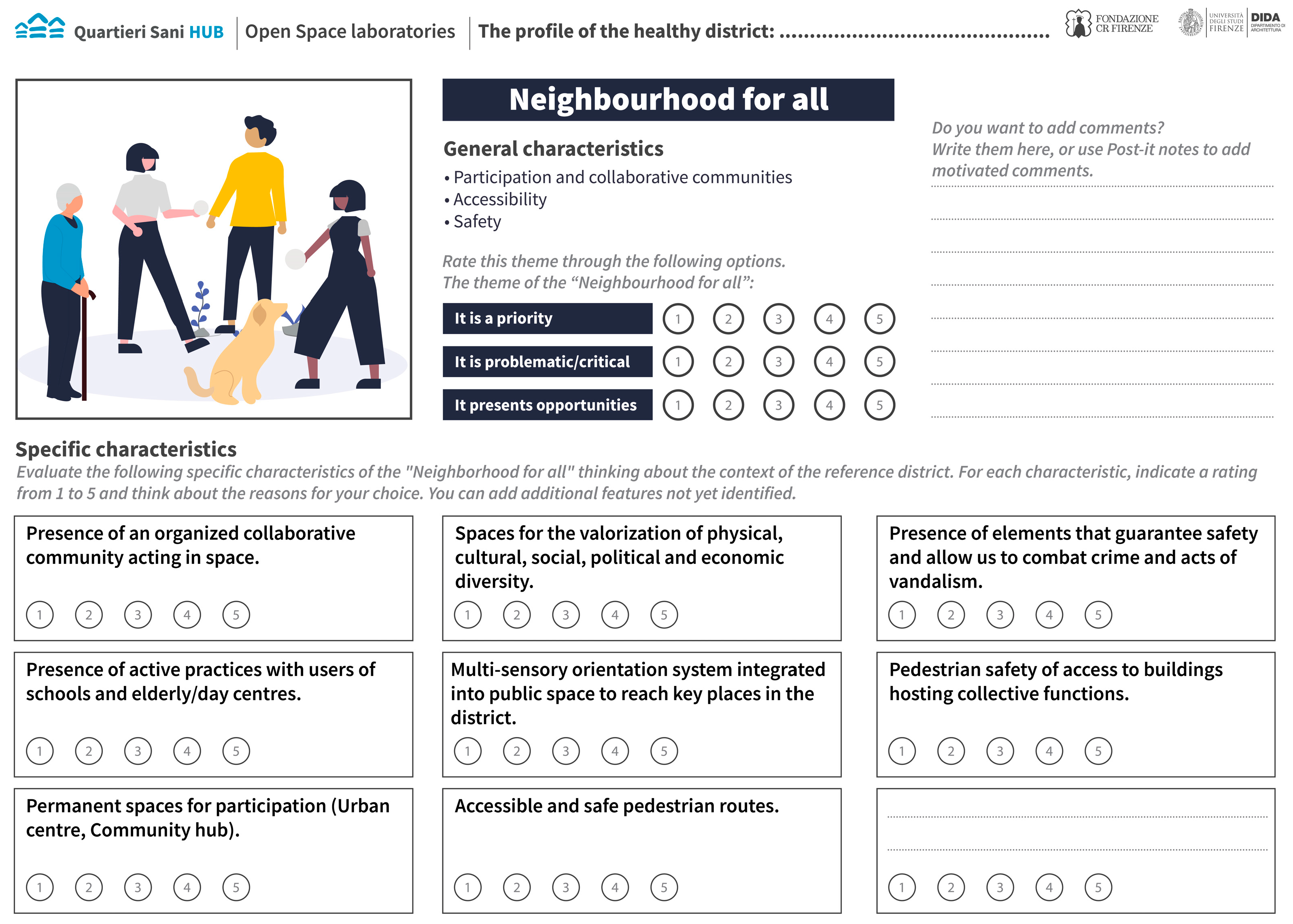
2.1.3. Templates Design for Collaborative Activities
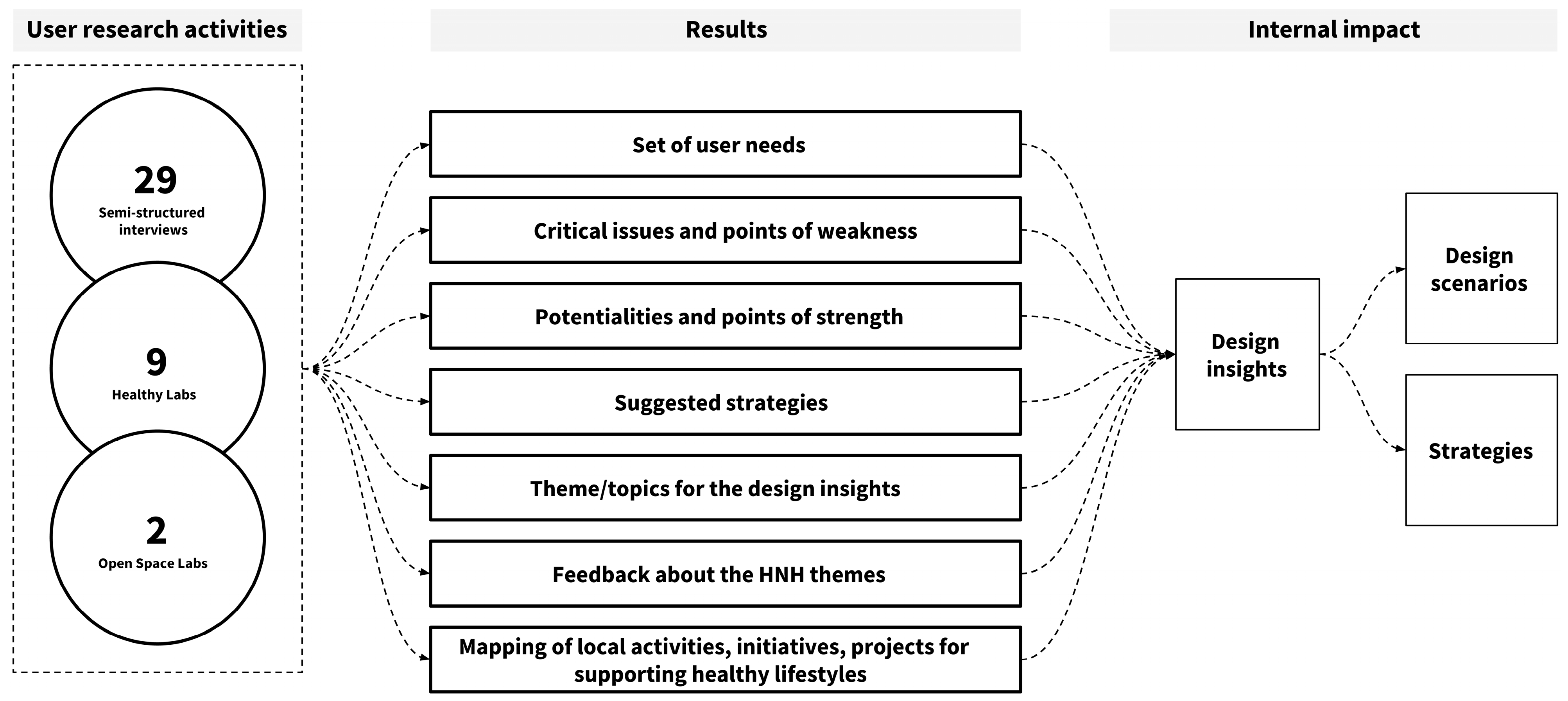
2.2. Application of the HNH Framework and Data Collection
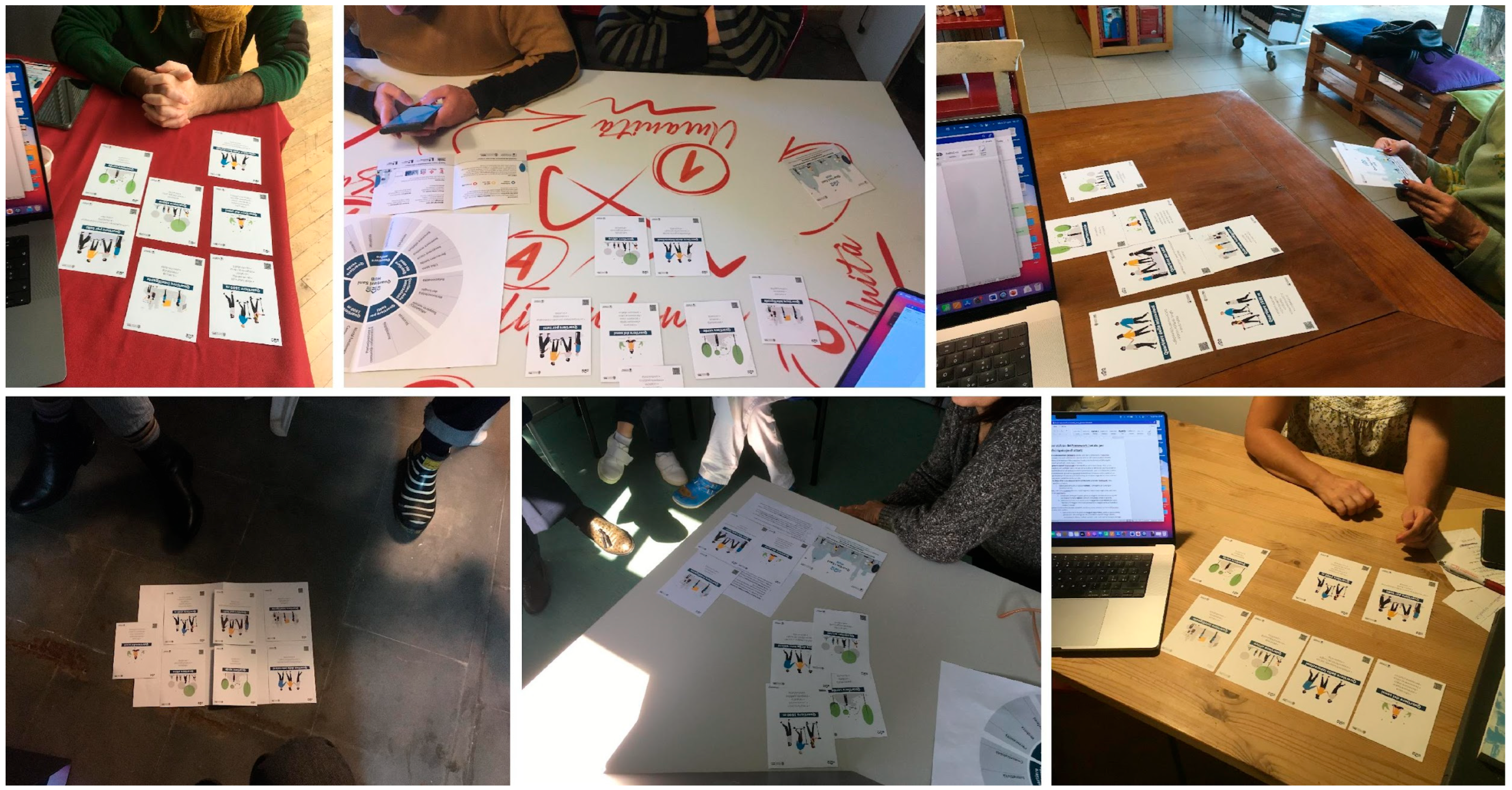
2.2.1. Semi-Structured Interviews and Card Sorting
- They live or work in one of the HNH project case study areas;
- They facilitate activities for or with citizens who live or work in one of the HNH project case study areas;
- They are in a position to know the expectations, activities, problems, and opportunities of/for the citizens that live or work in one of the HNH project case study areas.
2.2.2. Healthy Labs
2.2.3. Open Space Labs
- Ice-breaking to get to know each other and create a good atmosphere.
- Presentation of the specific tasks, topics, and the materials to be used.
- Discussion with all the group members about their reflections on the previous steps.
- Collective discussion about problems, opportunities, critical and potential areas for development, as well as solutions for the built environment in the case study area, using a shared map of the district. Here, participants were invited to draw, mark with post-it notes or dots, and localise the previously discussed aspects.
- Conclusive discussion about proposals and solutions for addressing the aforementioned issues.
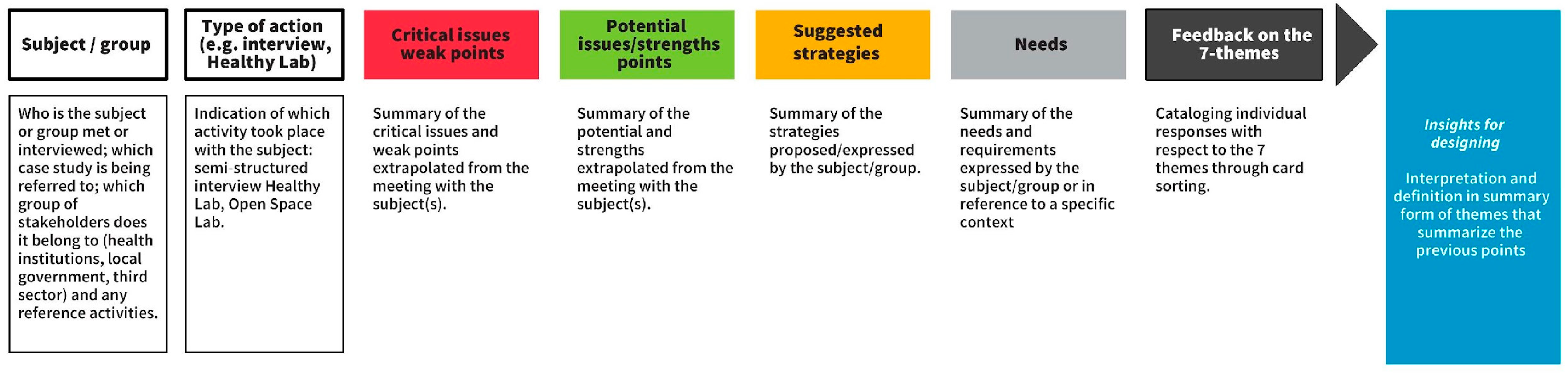
2.3. Data Analysis
3. Results
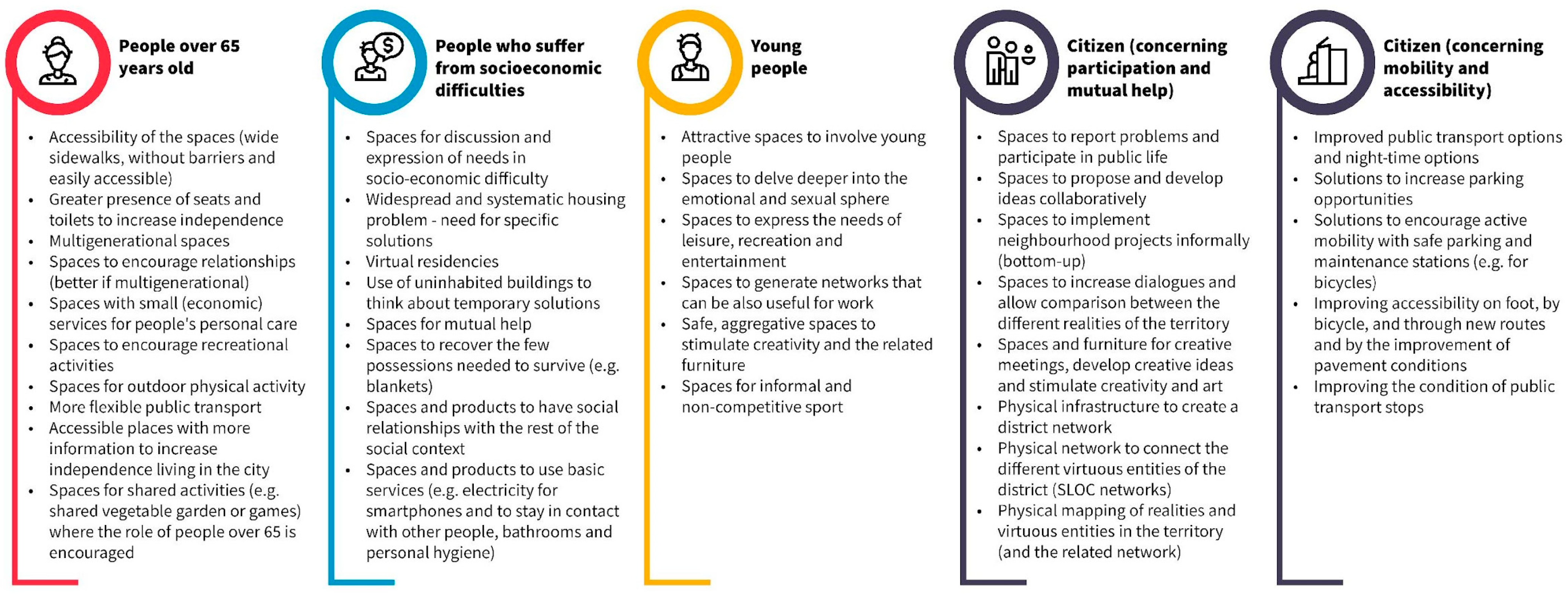
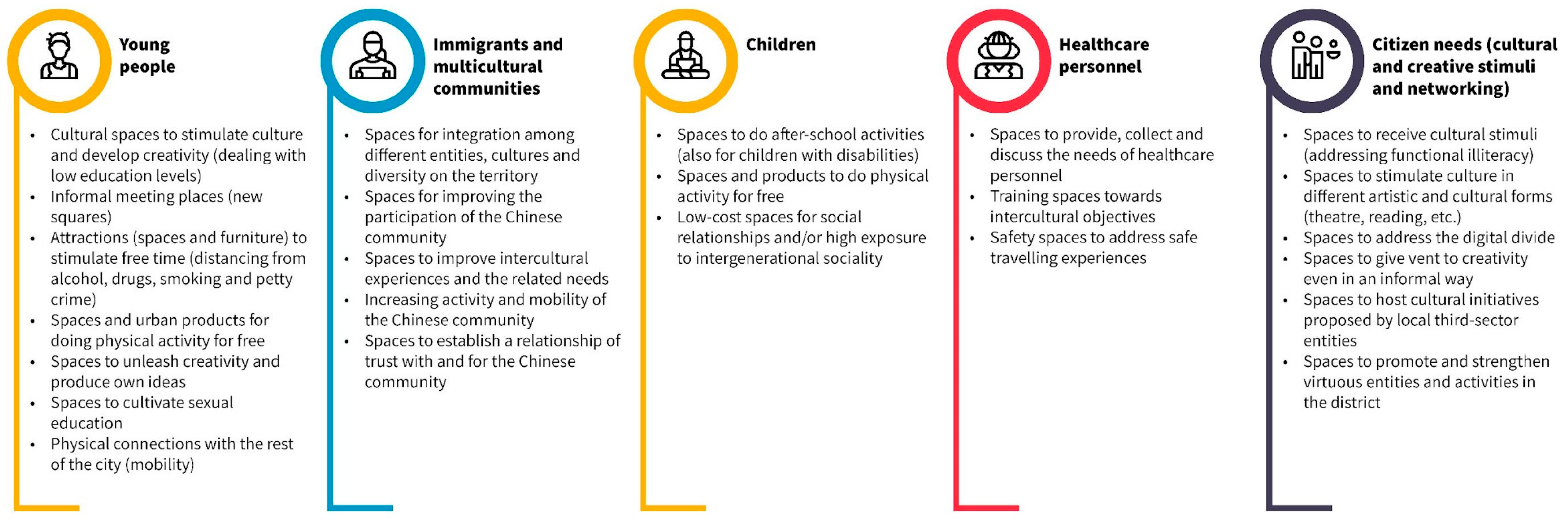
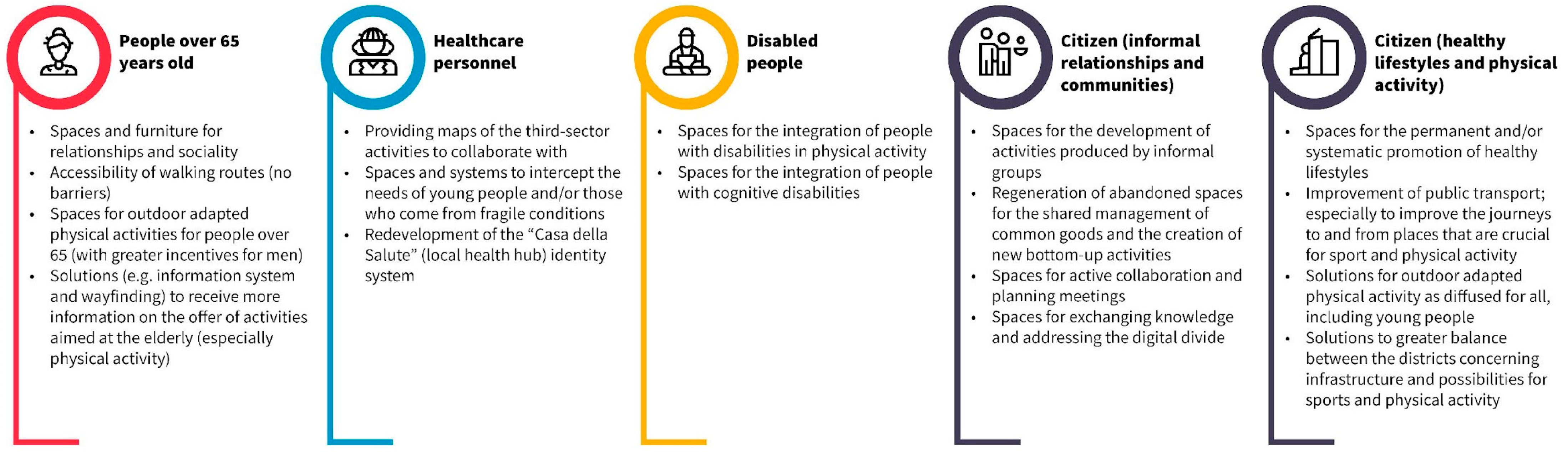
3.1. User Needs
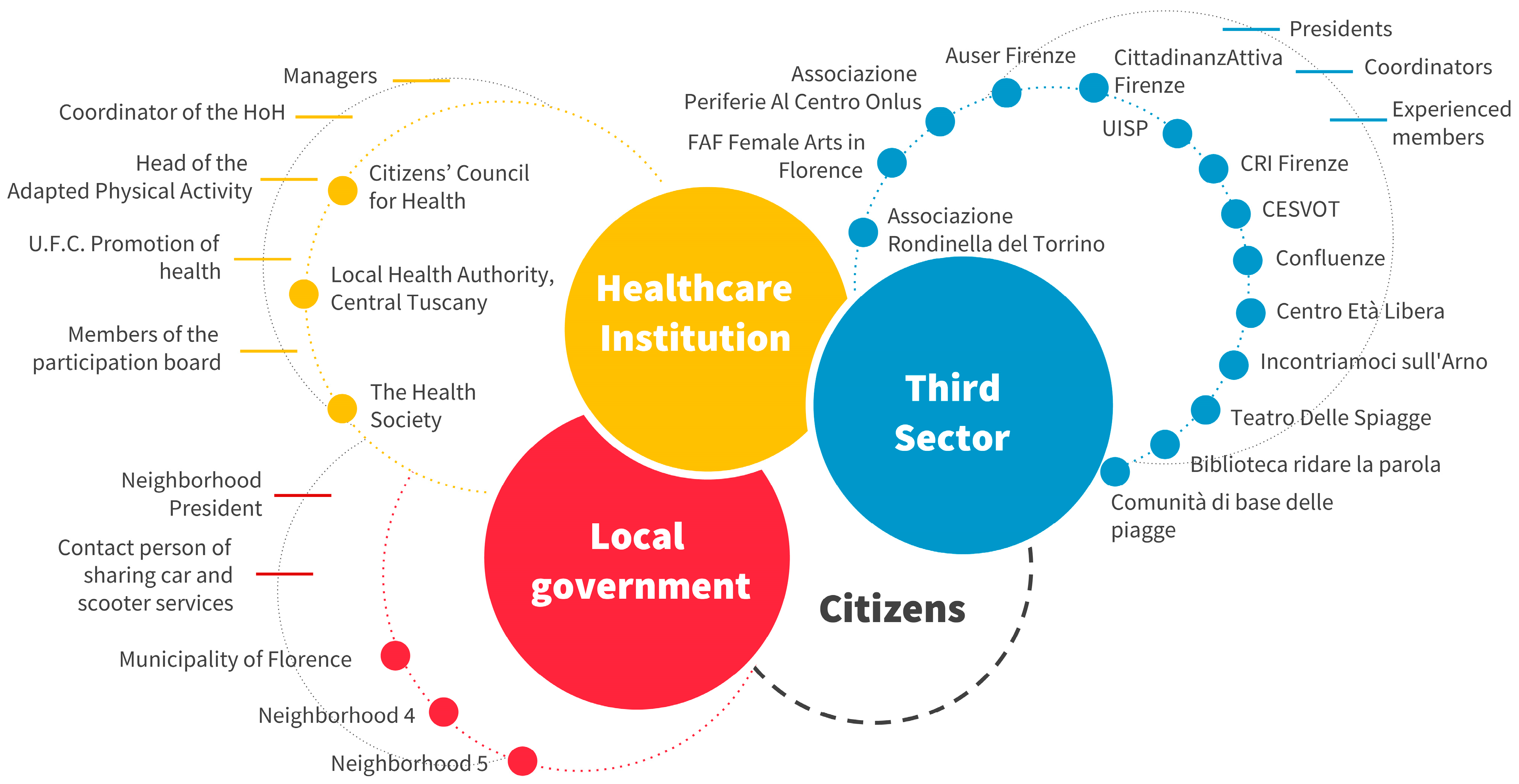
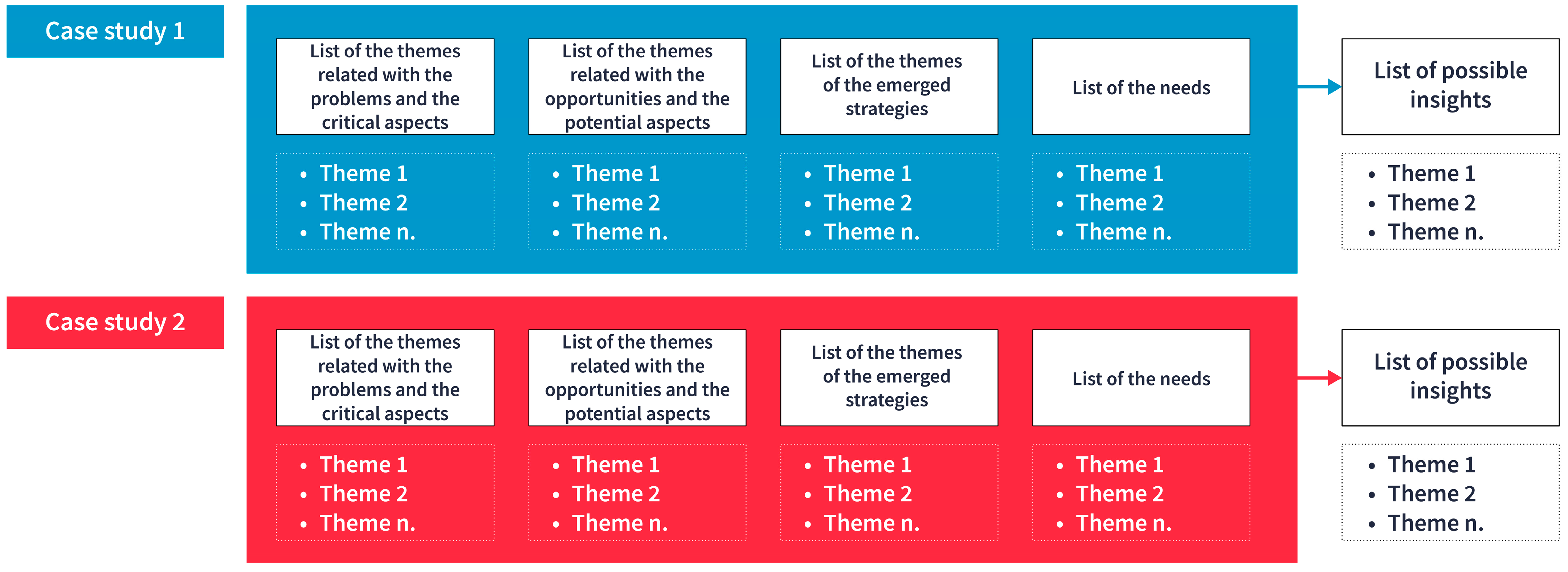
3.2. Insights from the Stakeholder’s Involvement
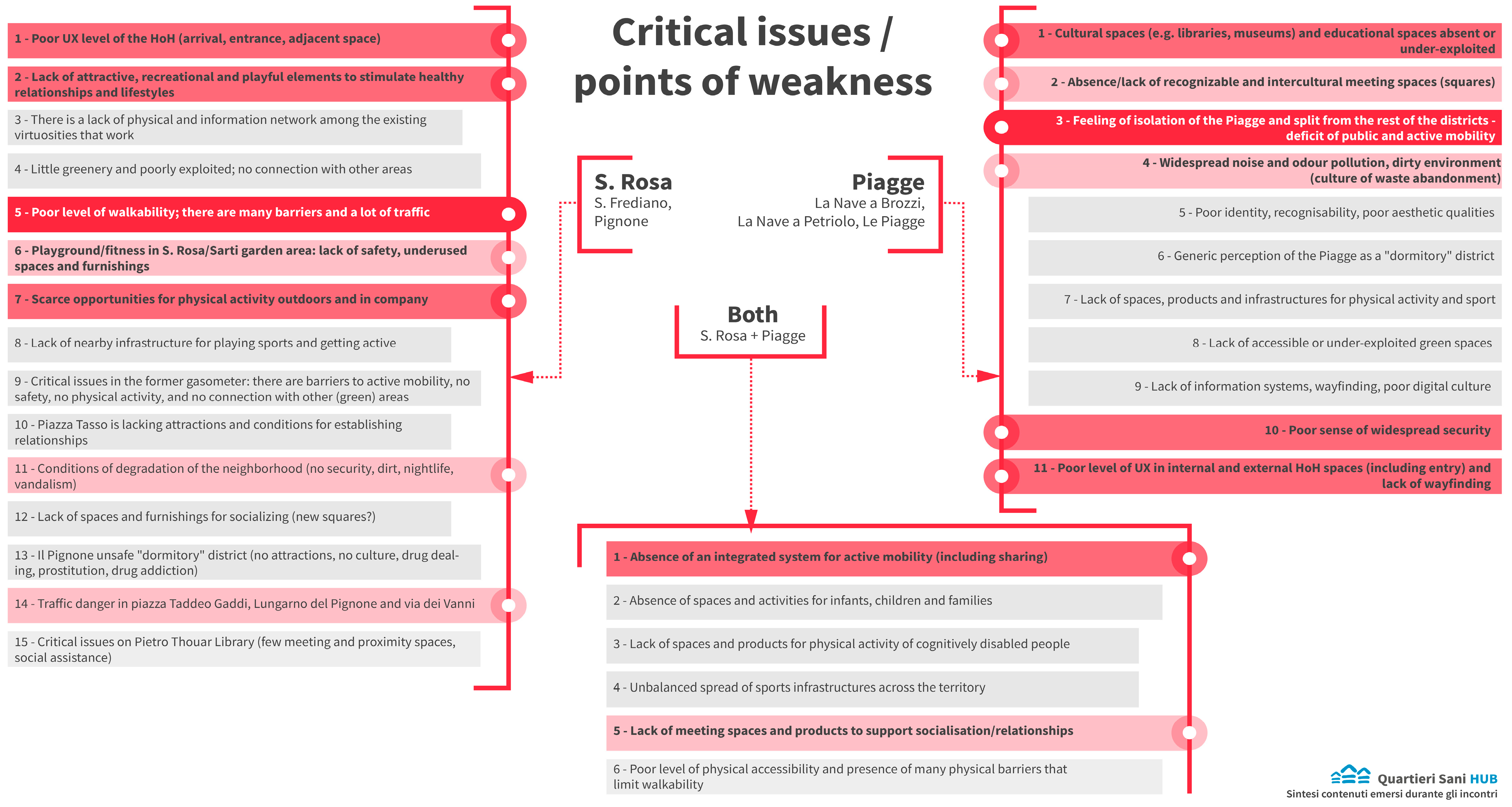
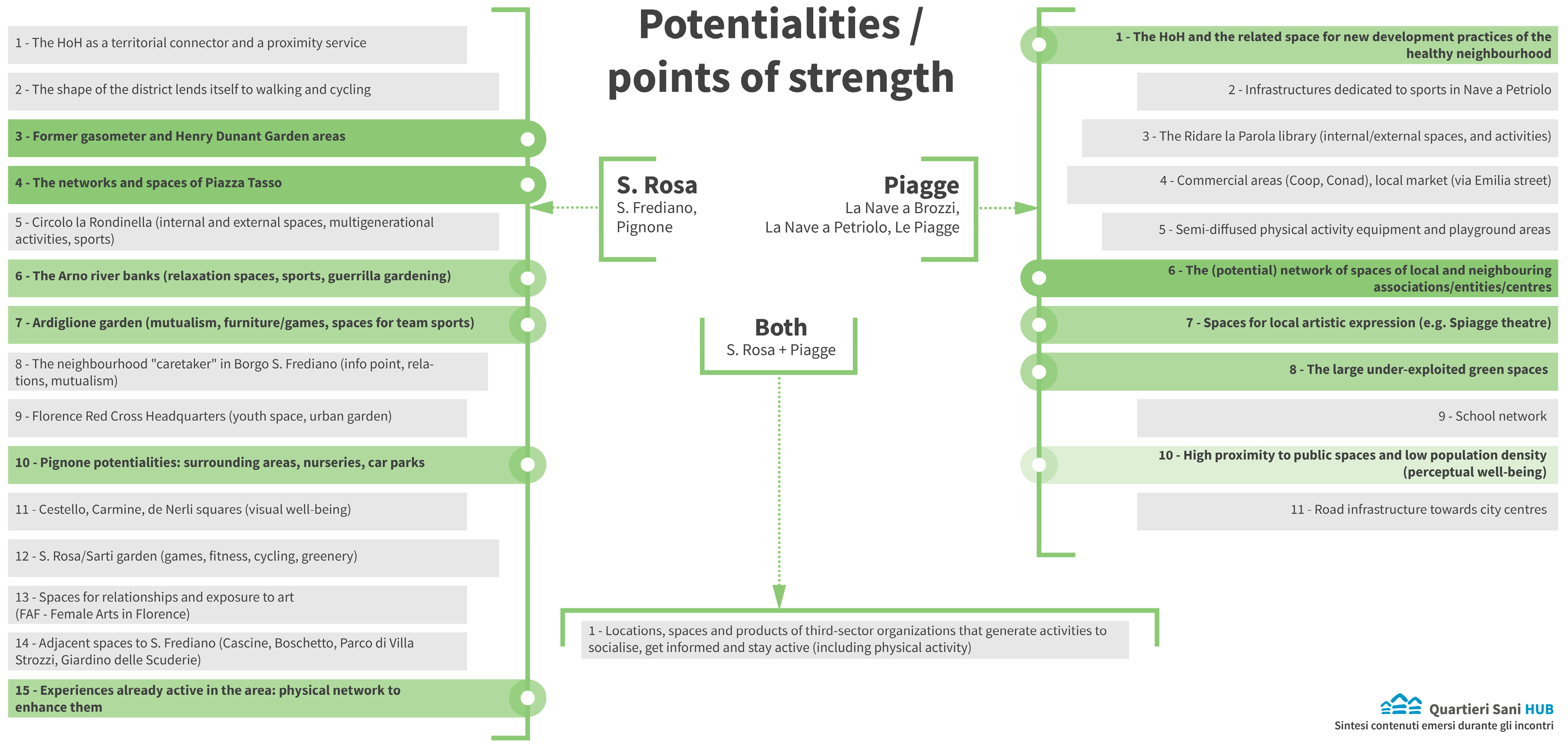
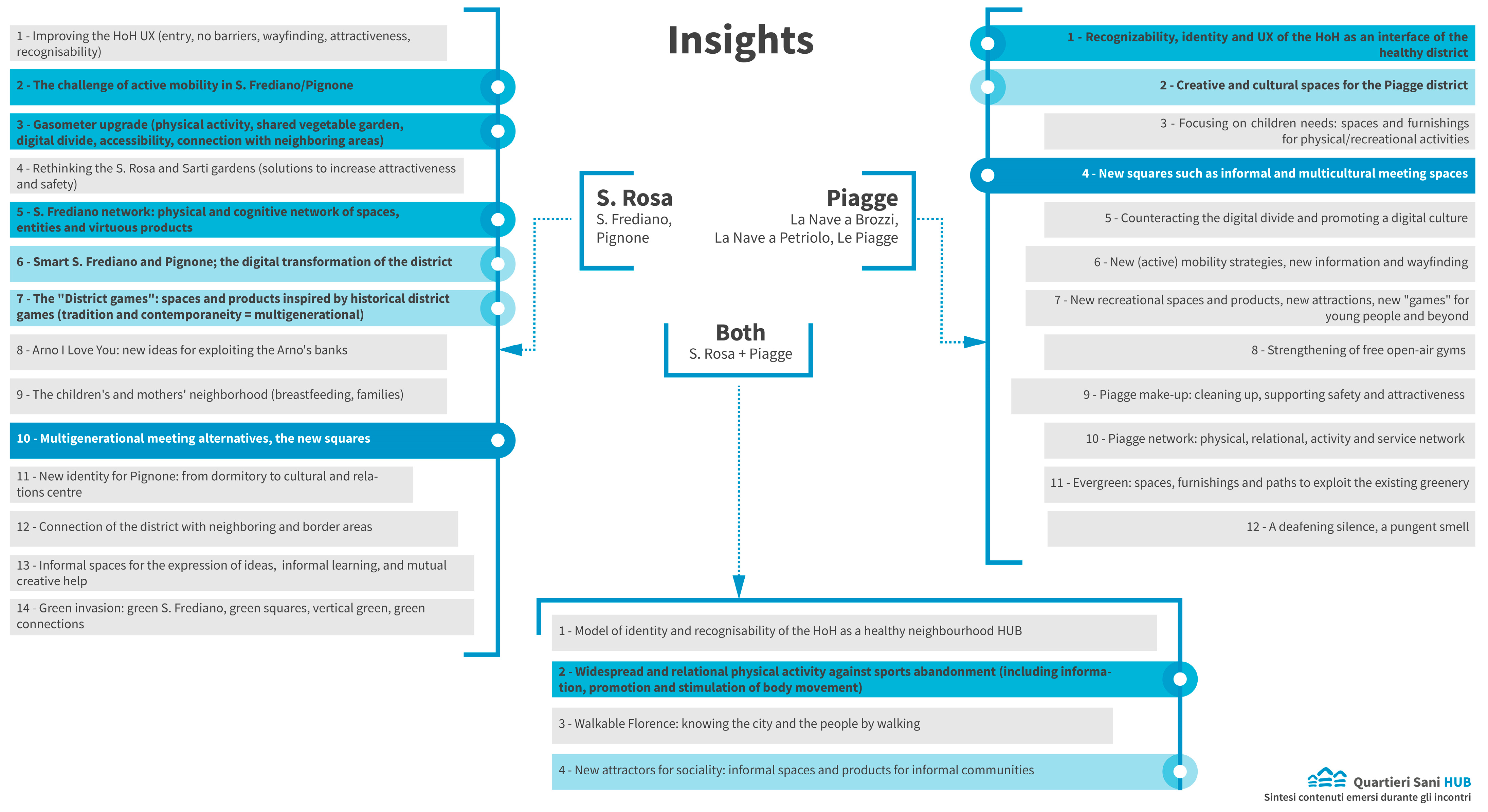
3.2.1. The Most Pressing Themes and Insights for Case Study 1
3.2.2. The Most Pressing Themes and Insights for Case Study 2
3.2.3. The Most Pressing Themes and Insights for Both Case Studies
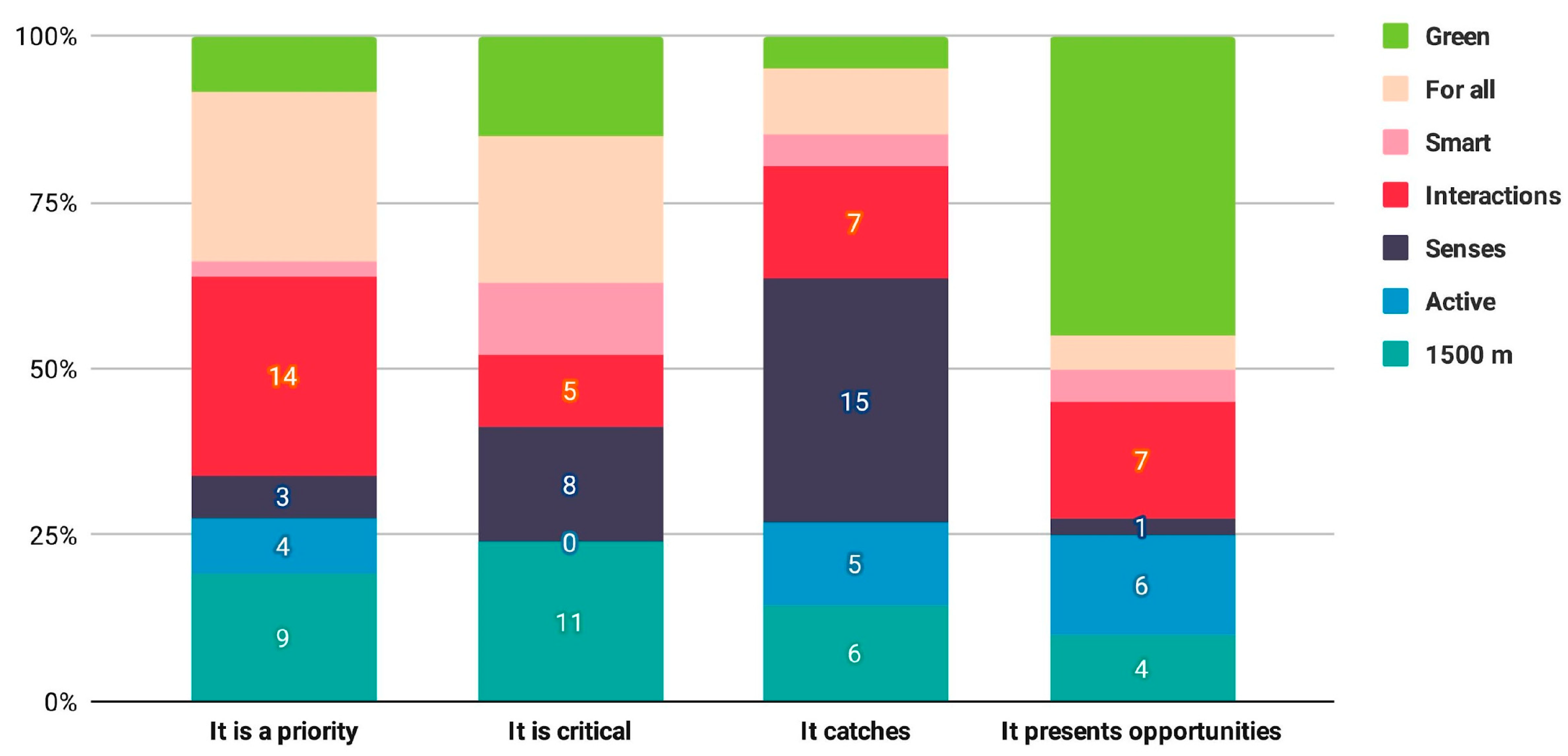
3.3. Feedback about the HNH Themes
3.4. Mapping of Local Activities, Initiatives, and Projects for Supporting Healthy Lifestyles
- Promoting body movement activities (e.g., walking, cycling, doing physical exercises).
- Informing citizens about healthy lifestyles and contrasting harmful habits such as the use of alcohol, smoking, unhealthy foods, and sedentary lifestyle.
- Promoting a sense of belonging and community with cultural projects.
- Promoting cultural events (e.g., art) to create social networking, community, and caring for the territory (e.g., walking experiences through the city art and cultural heritage).
- Creating educational events to raise public awareness about accessibility and inclusion regarding the needs of the most vulnerable population groups.
3.5. Emerging Thoughts for Applying the HNH Framework
- Increasing opportunities for socialisation, through places and urban products that support spontaneous encounters, community activities, citizen discussions, and systematic action planning for promoting healthy lifestyles; these aspects are requirements for developing healthy and inclusive places, promoting healthy lifestyles and behaviours.
- Creating connections among already-existing spaces, entities, and key district points through physical and cognitive infrastructures; these are crucial aspects in ensuring citizens’ healthy lifestyles; they should be made through both physical developments (e.g., wayfinding systems, urban furniture) and cognitive developments (e.g., services, initiatives).
- Developing a diffused sense of belonging and emotional experiences through spaces and furniture to create positive stimuli for the human senses, not only protecting them (e.g., solutions for noise pollution); healthy lifestyles are favoured when pleasurable physical environments enable one to favour healthier psychophysical conditions; furniture and architectural design may help in creating attractive spaces that favour a holistic perpetuation of health, security, belonging, inclusion, and community.
4. Discussion
4.1. Contribution to Design Practice and Research: Comparison with the Hypothesis and Discussion of the Obtained Results
4.2. Contribution to the Urban Health Approach: A Comparison with the Literature
4.3. Strengths and Challenges of the HNH as a Research Tool
4.4. Implications for Developing a Healthy Design Culture
4.5. Design Knowledge and Design Research for Health Promotions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barton, H. A health map for urban planners. Built Environ. 2005, 31, 339–355. [Google Scholar] [CrossRef]
- Barton, H.; Grant, M. A health map for the local human habitat. J. R. Soc. Promot. Health 2006, 126, 252–253. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization & UN-Habitat. Integrating Health in Urban and Territorial Planning: A Sourcebook; UN-HABITAT and World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Tang, X. Research on Urban Furniture Design in Communities from a Health Promotion Perspective. J. Humanit. Arts Soc. Sci. 2023, 7, 1451–1459. [Google Scholar] [CrossRef]
- Szewczenko, A.; Lach, E.; Bursiewicz, N.; Chuchnowska, I.; Widzisz-Pronobis, S.; Sanigórska, M.; Elsner, K.; Bal, D.; Sutor, M.; Włodarz, J.; et al. Urban Therapy—Urban Health Path as an Innovative Urban Function to Strengthen the Psycho-Physical Condition of the Elderly. Int. J. Environ. Res. Public Health 2023, 20, 6081. [Google Scholar] [CrossRef] [PubMed]
- Capolongo, S.; Lemaire, N.; Oppio, A.; Buffoli, M.; Gall, A.R.L. Action planning for healthy cities: The role of multi-criteria analysis, developed in Italy and France, for assessing health performances in land-use plans and urban development projects. Epidemiol. Prev. 2016, 40, 257–264. [Google Scholar] [PubMed]
- Capolongo, S.; Rebecchi, A.; Dettori, M.; Appolloni, L.; Azara, A.; Buffoli, M.; Capasso, L.; Casuccio, A.; Oliveri Conti, G.; D’Amico, A.; et al. Healthy design and urban planning strategies, actions, and policy to achieve salutogenic cities. Int. J. Environ. Res. Public Health 2018, 15, 2698. [Google Scholar] [CrossRef]
- Capolongo, S.; Buffoli, M.; Brambilla, A.; Rebecchi, A. Healthy urban planning and design strategies to improve urban quality and attractiveness of places. TECHNE-J. Technol. Archit. Environ. 2020, 19, 271–279. [Google Scholar]
- Sallis, J.F.; Glanz, K. The role of built environments in physical activity, eating, and obesity in childhood. Future Child. 2006, 16, 89–108. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Floyd, M.F.; Rodríguez, D.A.; Saelens, B.E. Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation 2012, 125, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Bull, F.; Burdett, R.; Frank, L.D.; Griffiths, P.; Giles-Corti, B.; Stevenson, M. Use of science to guide city planning policy and practice: How to achieve healthy and sustainable future cities. Lancet 2016, 388, 2936–2947. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Li, M.; Perez, M.A.; Wang, C.H. Plan for healthy neighborhoods to improve mental wellbeing: A pilot study in Fresno, California. Comput. Urban Sci. 2022, 2, 26. [Google Scholar] [CrossRef]
- Krieger, J.; Jacobs, D.E. Healthy homes. In Making Healthy Places: Designing and Building for Health, Well-Being, and Sustainability; Dannenberg, A.L., Frumkin, H., Jackson, R.J., Eds.; Island Press: Washington, DC, USA, 2011; pp. 170–187. [Google Scholar]
- Reddy, A.L.; Gomez, M.; Dixon, S.L. The New York State Healthy Neighborhoods Program. J. Public Health Manag. Pract. 2017, 23, 210–218. [Google Scholar] [CrossRef]
- Burden, D.; Davis, D.; Sprowls, S.; Zykofsky, P.; Wallwork, M. Street Design Guidelines for Healthy Neighborhoods; Center for Livable Communities: Sacramento, CA, USA, 2002. [Google Scholar]
- Transport for London. Healthy Streets for London: Prioritising Walking, Cycling and Public Transport to Create a Healthy City; Transport for London: London, UK, 2017. Available online: https://content.tfl.gov.uk/healthy-streets-for-london.pdf (accessed on 23 January 2024).
- Transport for London. Guide to the Healthy Streets Indicators: Delivering the Healthy Streets Approach; Transport for London: London, UK, 2017. Available online: https://content.tfl.gov.uk/guide-to-the-healthy-streets-indicators.pdf (accessed on 23 January 2024).
- Plowden, B. Creating healthy streets for sustainable cities–delivering public health benefits through redesigning London’s streets. Cities Health 2020, 4, 156–161. [Google Scholar] [CrossRef]
- Marshall, J.D.; Brauer, M.; Frank, L.D. Healthy neighborhoods: Walkability and air pollution. Environ. Health Perspect. 2009, 117, 1752–1759. [Google Scholar] [CrossRef] [PubMed]
- Wineman, J.D.; Marans, R.W.; Schulz, A.J.; van der Westhuizen, D.L.; Mentz, G.B.; Max, P. Designing healthy neighborhoods: Contributions of the built environment to physical activity in Detroit. J. Plan. Educ. Res. 2014, 34, 180–189. [Google Scholar] [CrossRef]
- Hohl, B.C.; Kondo, M.C.; Kajeepeta, S.; MacDonald, J.M.; Theall, K.P.; Zimmerman, M.A.; Branas, C.C. Creating safe and healthy neighborhoods with place-based violence interventions. Health Aff. 2019, 38, 1687–1694. [Google Scholar] [CrossRef]
- Capolongo, S.; Buffoli, M.; Mosca, E.I.; Galeone, D.; D’Elia, R.; Rebecchi, A. Public health aspects’ assessment tool for urban projects, according to the urban health approach. In Regeneration of the Built Environment from a Circular Economy Perspective; Della Torre, S., Cattaneo, S., Lenzi, C., Zanelli, A., Eds.; Springer: Cham, Switzerland, 2020; pp. 325–335. [Google Scholar]
- Forsyth, A.; Salomon, E.; Smead, L. Creating Healthy Neighborhoods: Evidence-Based Planning and Design Strategies; Routledge: Abingdon, UK, 2017. [Google Scholar]
- Galea, S.; Vlahov, D. Urban health: Evidence, challenges, and directions. Annu. Rev. Public Health 2005, 26, 341–365. [Google Scholar] [CrossRef] [PubMed]
- Jonek-Kowalska, I. Health Care in Cities Perceived as Smart in the Context of Population Aging—A Record from Poland. Smart Cities 2022, 5, 1267–1292. [Google Scholar] [CrossRef]
- Wielicka-Gańczarczyk, K.; Jonek-Kowalska, I. Involvement of Local Authorities in the Protection of Residents’ Health in the Light of the Smart City Concept on the Example of Polish Cities. Smart Cities 2023, 6, 744–763. [Google Scholar] [CrossRef]
- World Health Organization. Age-Friendly Environments in Europe: Indicators, Monitoring and Assessments; World Health Organization—Regional Office for Europe: København, Denmark, 2016. Available online: https://www.who.int/publications/i/item/9789289052122 (accessed on 23 January 2024).
- World Health Organization. Decade of Healthy Ageing: Baseline Report; World Health Organization (WHO): Geneva, Switzerland, 2020. Available online: https://www.who.int/publications/i/item/9789240017900 (accessed on 23 January 2024).
- Carroll, S.; Jespersen, A.P.; Troelsen, J. Going along with older people: Exploring age-friendly neighbourhood design through their lens. J. Hous. Built Environ. 2020, 35, 555–572. [Google Scholar] [CrossRef]
- Xu, L.; Han, H.; Yang, C.; Liu, Q. The Influence Mechanism of the Community Subjectively Built Environment on the Physical and Mental Health of Older Adults. Sustainability 2023, 15, 13211. [Google Scholar] [CrossRef]
- Burton, E.; Mitchell, L. Inclusive Urban Design: Streets for Life; Routledge: Abingdon, UK, 2006. [Google Scholar]
- Burton, E.; Mitchell, L.; Raman, S. Neighbourhoods for Life: Designing Dementia-Friendly Outdoor Environments. A Findings Leaflet; Oxford Institute for Sustainable Development, Oxford Brookes University: Oxford, UK, 2004. [Google Scholar]
- Bevan, M.; Croucher, K. Lifetime Neighbourhoods. Department for Communities and Local Government. 2011. Available online: https://www.gov.uk/government/publications/lifetime-neighbourhoods--2 (accessed on 23 January 2024).
- The City of New York. The Active Design Guidelines: Promoting Physical Activity through Design; The City of New York: New York, NY, USA, 2010.
- Lee, K.K. Developing and implementing the active design guidelines in New York City. Health Place 2012, 18, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Sport England. Active Design: Planning for Health and Wellbeing through Sport and Physical Activity; Sport England: Loughborough, UK, 2015. [Google Scholar]
- City of London. City of London Street Accessibility Tool. Available online: https://www.cityoflondon.gov.uk/services/streets/city-of-london-street-accessibility-tool (accessed on 23 January 2024).
- London, F. Healthy Placemaking: Wellbeing through Urban Design; Routledge: Abingdon, UK, 2020. [Google Scholar]
- Ministero della Salute. Documento di Indirizzo per la Pianificazione Urbana in Un’ottica di Salute Pubblica [Guidance Document for Urban Planning from a Public Health Perspective]. Direzione Generale della Prevenzione Sanitaria. 2021. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_3125_allegato.pdf (accessed on 23 January 2024).
- Buffoli, M.; Rebecchi, A.; Dell’Ovo, M.; Oppio, A.; Capolongo, S. Transforming the Built Environment through Healthy-Design Strategies. In New Metropolitan Perspectives; Bevilacqua, C., Calabrò, F., Della Spina, L., Eds.; Springer: Cham, Switzerland, 2020; pp. 187–196. [Google Scholar]
- UN-Habitat. MY Neighbourhood. United Nations Human Settlements Programme (UN-Habitat). Available online: https://unhabitat.org/my-neighbourhood (accessed on 23 January 2024).
- Gardner, J.; Marpillero-Colomina, A.; Begault, L. Inclusive Healthy Places: A Guide to Inclusion & Health in Public Space: Learning Globally to Transform Locally; Gehl Institute: New York, NY, USA, 2018. [Google Scholar]
- NHS. Putting Health into Place: Executive Summary. Available online: https://www.england.nhs.uk/publication/putting-health-into-place-executive-summary/ (accessed on 23 January 2024).
- Roe, J.; McCay, L. Restorative Cities: Urban Design for Mental Health and Wellbeing; Bloomsbury Publishing: London, UK, 2021. [Google Scholar]
- Grant, M.; Siri, J.; Gatzweiler, F.; Dora, C.; Aerts, J.; Nandudu, S.; Claeson, A.; Carbajal, P.; Roebbel, N.; Petrella, L.; et al. Supporting a healthy planet, healthy people and health equity through urban and territorial planning. Plan. Pract. Res. 2022, 37, 111–130. [Google Scholar] [CrossRef]
- World Health Organization. Integrating Health in Urban and Territorial Planning: Directory of Resources for Planning Healthy Environments. Available online: https://www.who.int/tools/integrating-health-in-urban-and-territorial-planning--the-directory (accessed on 23 January 2024).
- BC Centre for Disease Control. Healthy Built Environment Linkages Toolkit: Making the Links between Design, Planning and Health; BC Centre for Disease Control–Population & Public Health: Vancouver, BC, Canada, 2018; Available online: http://www.bccdc.ca/pop-public-health/Documents/HBE_linkages_toolkit_2018.pdf (accessed on 23 January 2024).
- Active Neighbourhoods Canada (n.d.). Active Neighbourhoods Canada. Available online: https://participatoryplanning.ca/ (accessed on 23 January 2024).
- AlWaer, H.; Speedie, J.; Cooper, I. Unhealthy Neighbourhood “Syndrome”: A Useful Label for Analysing and Providing Advice on Urban Design Decision-Making? Sustainability 2021, 13, 6232. [Google Scholar] [CrossRef]
- Manzini, E. Design culture and dialogic design. Des. Issues 2016, 32, 52–59. [Google Scholar] [CrossRef]
- Julier, G. From design culture to design activism. Des. Cult. 2013, 5, 215–236. [Google Scholar] [CrossRef]
- Hu, M.; Roberts, J.D. Connections and divergence between public health and built environment—A scoping review. Urban Sci. 2020, 4, 12. [Google Scholar] [CrossRef]
- Manzini, E. Livable Proximity: Ideas for the City That Cares; EGEA Spa: Evanston, IL, USA, 2022. [Google Scholar]
- Benini, J.; Manzini, E.; Parameswaran, L. Care Up-Close and Digital: A Designers’ Outlook on the Pandemic in Barcelona. Des. Cult. 2021, 13, 91–102. [Google Scholar] [CrossRef]
- Boschma, R. Proximity and innovation: A critical assessment. Reg. Stud. 2005, 39, 61–74. [Google Scholar] [CrossRef]
- Moreno, C.; Allam, Z.; Chabaud, D.; Gall, C.; Pratlong, F. Introducing the “15-Minute City”: Sustainability, resilience and place identity in future post-pandemic cities. Smart Cities 2021, 4, 93–111. [Google Scholar] [CrossRef]
- Pozoukidou, G.; Chatziyiannaki, Z. 15-Minute City: Decomposing the new urban planning eutopia. Sustainability 2021, 13, 928. [Google Scholar] [CrossRef]
- Manzini, E. Design, When Everybody Designs: An Introduction to Design for Social Innovation; MIT Press: Cambridge, MA, USA, 2015. [Google Scholar]
- El-Askari, G.; Freestone, J.; Irizarry, C.; Kraut, K.L.; Mashiyama, S.T.; Morgan, M.A.; Walton, S. The Healthy Neighborhoods Project: A local health department’s role in catalyzing community development. Health Educ. Behav. 1998, 25, 146–159. [Google Scholar] [CrossRef] [PubMed]
- Hartman, D. Healthy Neighborhoods: A Collaborative Model. J. High. Educ. Outreach Engagem. 2000, 5, 56–61. [Google Scholar]
- Busciantella-Ricci, D.; Viviani, S.; Kianfar, K.; Rinaldi, A. Healthy and inclusive neighbourhoods: A theoretical framework for hearing excluded city voices. In Include 2022: Unheard Voices Global Conference, Proceedings of the 11th Inclusive Design Conference, Helen Hamlyn Centre for Design, Conference Proceedings, London, UK, 22–23 September 2022; The Helen Hamlyn Centre for Design, The Royal College of Art: London, UK, 2022. [Google Scholar]
- Sullivan, E.; Egli, V.; Donnellan, N.; Smith, M. Policies to enable children’s voice for healthy neighbourhoods and communities: A systematic mapping review and case study. Kōtuitui N. Z. J. Soc. Sci. Online 2021, 16, 18–44. [Google Scholar] [CrossRef]
- Zou, J.; Liu, Z.; Zhao, C. Co-design for active aging: An approach to stimulating creativity of the young elderly in urban China. Des. J. 2024, 27, 1–22. [Google Scholar] [CrossRef]
- Arcaya, M.C.; Schnake-Mahl, A.; Binet, A.; Simpson, S.; Church, M.S.; Gavin, V.; Coleman, B.; Levine, S.; Nielsen, A.; Carroll, L.; et al. Community change and resident needs: Designing a participatory action research study in metropolitan Boston. Health Place 2018, 52, 221–230. [Google Scholar] [CrossRef]
- Daepp, M.I.; Binet, A.; Gavin, V.; Arcaya, M.C.; Healthy Neighborhoods Research Consortium. The moving mapper: Participatory action research with big data. J. Am. Plan. Assoc. 2022, 88, 179–191. [Google Scholar] [CrossRef]
- Ludden, G. Design for healthy behaviour. In Design for Behaviour Change: Theories and Practices of Designing for Change; Niedderer, K., Clune, S., Ludden, G., Eds.; Routledge: Abingdon, UK, 2017; pp. 93–103. [Google Scholar]
- Niedderer, K.; Ludden, G.; Clune, S.; Lockton, D.; MacKrill, J.B.; Morris, A.; Cain, R.; Gardiner, E.; Evans, M.; Gutteridge, R.; et al. Design for behaviour change as a driver for sustainable innovation: Challenges and opportunities for implementation in the private and public sectors. Int. J. Des. 2016, 10, 67–85. [Google Scholar]
- Thaler, R.H.; Sunstein, C.R. Nudge: Improving Decisions about Health, Wealth, and Happiness; Yale University Press: New Haven, CT, USA, 2008. [Google Scholar]
- Raynor, K.E.; Doyon, A.; Beer, T. Collaborative planning, transitions management and design thinking: Evaluating three participatory approaches to urban planning. Aust. Plan. 2017, 54, 215–224. [Google Scholar] [CrossRef]
- Glanville, R. Researching design and designing research. Des. Issues 1999, 15, 80–91. [Google Scholar] [CrossRef]
- Jonas, W. Research through design is more than just a new form of disseminating design outcomes. Constr. Found. 2015, 11, 32–36. [Google Scholar]
- Frayling, C. Research in art and design. R. Coll. Art Res. Pap. 1993, 1, 1–5. [Google Scholar]
- Setola, N.; Rinaldi, A.; Macchi, A.; Busciantella Ricci, D. Healthy and inclusive neighbourhoods in Florence: A new research approach for public urban spaces. In International Conference “Species of Spaces: Fostering Psycho-Physical Well-Being by Design”, SITdA—Environmental Accessibility Cluster; Department of Architecture, University of Florence: Florence, Italy, 2023. [Google Scholar]
- Lingua, V.; Setola, N.; Rinaldi, A.; Morelli, E. Quartieri Sani Hub: Healthy and Inclusive Neighborhoods for the Communities of the Metropolitan City of Florence. In SBEUT-Sustainable Built Environment and Urban Transition Conference. 2023. Available online: https://open.lnu.se/index.php/sbut/article/view/3832/3511 (accessed on 23 January 2024).
- Ostroff, E. Universal design: An evolving paradigm. In Universal Design Handbook, 2nd ed.; Preiser, W.F.E., Smith, K.H., Eds.; McGraw-Hill: New York, NY, USA, 2011; pp. 34–42. [Google Scholar]
- Clarkson, P.J.; Coleman, R. History of inclusive design in the UK. Appl. Ergon. 2015, 46, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Bendixen, K.; Benktzon, M. Design for All in Scandinavia–A strong concept. Appl. Ergon. 2015, 46, 248–257. [Google Scholar] [CrossRef]
- Manzini, E. New design knowledge. Des. Stud. 2009, 30, 4–12. [Google Scholar] [CrossRef]
- Cross, N. Design research: A disciplined conversation. Des. Issues 1999, 15, 5–10. [Google Scholar] [CrossRef]
- Cross, N. Designerly Ways of Knowing; Springer: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- Ayres, L. Semi-Structured Interview. In The Sage Encyclopedia of Qualitative Research Methods; Given, L.M., Ed.; SAGE Publications: Thousand Oaks, CA, USA, 2008; pp. 810–811. [Google Scholar]
- Douglas Caulkins, D. Ethnography. In The SAGE Encyclopedia of Action Research; David, C., Ed.; SAGE Publications: Thousand Oaks, CA, USA, 2014; pp. 309–314. [Google Scholar]
- Roulston, K.J. Probes and probing. In The Sage Encyclopedia of Qualitative Research Methods; Given, L.M., Ed.; Sage: Thousand Oaks, CA, USA, 2008; Volumes 1 and 2, pp. 681–683. [Google Scholar]
- Hanington, B.; Martin, B. Universal Methods of Design Expanded and Revised: 125 Ways to Research Complex Problems, Develop Innovative Ideas, and Design Effective Solutions; Rockport Publishers: Beverly, MA, USA, 2019. [Google Scholar]
- Roy, R.; Warren, J.P. Card-based design tools: A review and analysis of 155 card decks for designers and designing. Des. Stud. 2019, 63, 125–154. [Google Scholar] [CrossRef]
- Marsh, S. User Research: A Practical Guide to Designing Better Products and Services; Kogan Page Publishers: London, UK, 2018. [Google Scholar]
- Dong, H.; McGinley, C.; Nickpour, F.; Cifter, A.S.; Inclusive Design Research Group. Designing for designers: Insights into the knowledge users of inclusive design. Appl. Ergon. 2015, 46, 284–291. [Google Scholar] [CrossRef]
- Olesen, A.R.; Holdgaard, N.; Løvlie, A.S. Co-designing a co-design tool to strengthen ideation in digital experience design at museums. CoDesign 2022, 18, 227–242. [Google Scholar] [CrossRef]
- Mueller, J.; Lu, H.; Chirkin, A.; Klein, B.; Schmitt, G. Citizen Design Science: A strategy for crowd-creative urban design. Cities 2018, 72, 181–188. [Google Scholar] [CrossRef]
- Hodgkinson, I.R.; Mousavi, S.; Hughes, P. New development: Citizen science—Discovering (new) solutions to wicked problems. Public Money Manag. 2022, 42, 133–136. [Google Scholar] [CrossRef]
- Trischler, J.; Dietrich, T.; Rundle-Thiele, S. Co-design: From expert-to user-driven ideas in public service design. Public Manag. Rev. 2019, 21, 1595–1619. [Google Scholar] [CrossRef]
- Pirinen, A. The barriers and enablers of co-design for services. Int. J. Des. 2016, 10, 27–42. [Google Scholar]
- Sanders, E.B.N.; Stappers, P.J. Co-creation and the new landscapes of design. Co-Design 2008, 4, 5–18. [Google Scholar] [CrossRef]
- Nielsen, L. Personas-User Focused Design; Springer: Berlin/Heidelberg, Germany, 2013; Volume 15. [Google Scholar]
- Holden, R.J.; Daley, C.N.; Mickelson, R.S.; Bolchini, D.; Toscos, T.; Cornet, V.P.; Miller, A.; Mirro, M.J. Patient decision-making personas: An application of a patient-centered cognitive task analysis (P-CTA). Appl. Ergon. 2020, 87, 103107. [Google Scholar] [CrossRef] [PubMed]
- Ali Amer Jid Almahri, F.; Bell, D.; Arzoky, M. Personas design for conversational systems in education. Informatics 2019, 6, 46. [Google Scholar] [CrossRef]
- Chun, J.S.; Larrick, R.P. The power of rank information. J. Personal. Soc. Psychol. 2022, 122, 983. [Google Scholar] [CrossRef] [PubMed]
- AlWaer, H.; Cooper, I. Changing the focus: Viewing design-led events within collaborative planning. Sustainability 2020, 12, 3365. [Google Scholar] [CrossRef]
- Roulston, K.; Choi, M. Qualitative interviews. In The SAGE Handbook of Qualitative Data Collection; SAGE Publications Ltd.: London, UK, 2018; pp. 233–249. [Google Scholar]
- Bekele, W.B.; Ago, F.Y. Sample size for interview in qualitative research in social sciences: A guide to novice researchers. Res. Educ. Policy Manag. 2022, 4, 42–50. [Google Scholar] [CrossRef]
- Guest, G.; Bunce, A.; Johnson, L. How many interviews are enough? An experiment with data saturation and variability. Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Garvin, E.; Branas, C.; Keddem, S.; Sellman, J.; Cannuscio, C. More than just an eyesore: Local insights and solutions on vacant land and urban health. J. Urban Health 2013, 90, 412–426. [Google Scholar] [CrossRef]
- Krueger, R.A. Focus Groups: A Practical Guide for Applied Research; Sage Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Bruseberg, A.; McDonagh-Philp, D. Focus groups to support the industrial/product designer: A review based on current literature and designers’ feedback. Appl. Ergon. 2002, 33, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Heidi, J. Content analysis. In The Sage Encyclopedia of Qualitative Research Methods; Given, L.M., Ed.; Sage Publications: Thousand Oaks, CA, USA, 2008; pp. 120–122. [Google Scholar]
- Archer, B. The nature of research. Co-Des. J. 1995, 2, 6–13. [Google Scholar]
- Archer, B. A View of the Nature of Design Research. In Design: Science: Method; Jacques, R., Powell, J., Eds.; Westbury House: Guildford, UK, 1981; pp. 30–47. [Google Scholar]
- Findeli, A.; Brouillet, D.; Martin, S.; Moineau, C.; Tarrago, R. Research through design and transdisciplinarity: A tentative contribution to the methodology of design research. In «Focused» Current Design Research Projects and Methods, Symposium Conducted at the Meeting of Swiss Design Network 2008; Swiss Design Network: Zürich, Switzerland, 2008; pp. 67–91. [Google Scholar]
- Cross, N. Designerly ways of knowing. Des. Stud. 1982, 3, 221–227. [Google Scholar] [CrossRef]
- Cross, N. Designerly ways of knowing: Design discipline versus design science. Des. Issues 2001, 17, 49–55. [Google Scholar] [CrossRef]
- Krogh, P.G.; Koskinen, I. Drifting by Intention: Four Epistemic Traditions from within Constructive Design Research; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Design Council. Design Methods for Developing Services. An Introduction to Service Design and a Selection of Service Design Tools. Design Council. 2015. Available online: https://www.designcouncil.org.uk/fileadmin/uploads/dc/Documents/DesignCouncil_Design%2520methods%2520for%2520developing%2520services.pdf (accessed on 23 January 2024).
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed]























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Critical Issues and Points of Weakness | Potentialities and Points of Strength | Suggested Strategies | Insights (Conceptual Themes to be Developed for the Co-design Phases) | |
|---|---|---|---|---|
| Case study 1 | 15 | 15 | 18 | 14 |
| Case study 2 | 11 | 11 | 13 | 12 |
| Both cases | 6 | 1 | 7 | 4 |
| Total | 32 | 27 | 38 | 30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Busciantella-Ricci, D.; Macchi, A.; Viviani, S.; Rinaldi, A. Healthy and Inclusive Neighbourhoods: A Design Research Toolkit for the Promotion of Healthy Behaviours. Sustainability 2024, 16, 3059. https://doi.org/10.3390/su16073059
Busciantella-Ricci D, Macchi A, Viviani S, Rinaldi A. Healthy and Inclusive Neighbourhoods: A Design Research Toolkit for the Promotion of Healthy Behaviours. Sustainability. 2024; 16(7):3059. https://doi.org/10.3390/su16073059
Chicago/Turabian StyleBusciantella-Ricci, Daniele, Alessia Macchi, Sara Viviani, and Alessandra Rinaldi. 2024. "Healthy and Inclusive Neighbourhoods: A Design Research Toolkit for the Promotion of Healthy Behaviours" Sustainability 16, no. 7: 3059. https://doi.org/10.3390/su16073059
APA StyleBusciantella-Ricci, D., Macchi, A., Viviani, S., & Rinaldi, A. (2024). Healthy and Inclusive Neighbourhoods: A Design Research Toolkit for the Promotion of Healthy Behaviours. Sustainability, 16(7), 3059. https://doi.org/10.3390/su16073059