Abstract
This investigation aimed to scrutinise the kinematic and spatio-temporal characteristics of free and Nordic walking (NW) in older adults, utilising both traditional and biosensor-integrated mechatronic poles. The hypothesis was that including biosensors for gait analysis in NW poles would not disrupt the walking pattern of older adults compared to standard poles. The study involved seniors aged 65–74 who were amateur Nordic Walking (NW) practitioners. They were instructed to traverse a 100-m distance three times: without poles, with traditional NW poles, and with mechatronic poles. The MyoMOTION MR3 system was used to gather biomechanical data. The study revealed differences in eight kinematic parameters and stride time between free walking and walking with poles. However, no statistically significant differences were observed in any of the parameters, regardless of the pole type used. The findings suggest that older NW practitioners tend to employ free walking patterns even when using poles.
1. Introduction
Human gait kinematic and spatio-temporal parameters change with age [1,2,3,4]. In particular, there is a reduction in the range of motion (ROM) in the joints of the limbs and spine and reduced muscle activity when walking. The time for double support is longer, the stride length is shortened, and the stride width is increased. Also, the walking speed is reduced by around 0.8–1.2 m/s, and the gait cadence is increased [1,2,5,6], related to a safer walking strategy, limiting the risk of losing balance and, consequently, dangerous falls in older adults [7]. These changes are associated with the involution of the musculoskeletal system, including muscle weakness, limited ROM in the joints, and poorer coordination and stability of body posture. They can also be affected by diseases more common in old age. For older adults, gait is an activity that requires good balance control. It decreases with age, resulting in changes in the gait pattern and limiting the duration of the phases and gait cycles associated with gait disturbance [1,8,9,10]. There is also an additional phenomenon occurring in the gait. Age is associated with more significant intra-individual gait variability for most gait measures [3,6], which may severely influence the power of statistical tests while investigating different gait patterns.
Nordic walking (NW) has been suggested as a method for preventing degenerative changes and increasing the functional effectiveness of the musculoskeletal system, influencing older adults’ gait [11]. Using poles while walking increases the ROM in the joints of the limbs and the involvement of muscles, especially the upper limbs [12]. In older individuals, NW resulted in longer strides and increased times of both double and single support compared to walking freely (without poles). During the NW gait, these people also had a lower walking speed and reduced step rate [13]. The literature demonstrates that NW reduces the load of the lumbar spine and lower limb joints and increases energy expenditure in comparison with recreational walking in older adults [14]. In addition, the beneficial effects of NW on different health parameters, such as resting heart rate, blood pressure, exercise capacity, and maximal oxygen consumption, have been established in elderly populations [15,16]. Other studies report improvements in muscle strength and flexibility in both upper and lower limbs along with enhanced general endurance among healthy older adults [17,18]. It should be emphasised that studies on the NW gait pattern among older people are sparse. Most concern the gait examination of pathological gaits or the use of NW during rehabilitation [11].
Having the correct walking technique with poles is essential to achieve the benefits of NW. With classic poles, learning this technique is difficult, especially for older adults. Mastering the correct gait style would be easier with the help of poles that are equipped with systems analysing the kinematic and spatio-temporal parameters of the gait in real time, informing the user about any gait abnormalities through a voice or light signal [19]. The paucity of studies on such systems necessitates further research [19]. In light of the results from other researchers and our prior observations, a model of NW mechatronic poles (classic NW poles equipped with sensors analysing the biomechanics of gait) was developed, which would allow for feedback on the NW gait technique with the possibility of its correction in real time [20]. In the mobile system of mechatronic NW poles, we have developed measures, records, and processes for selected kinematic values that allow for the assessment of the correctness of gait during NW walking in field conditions. The sensors are placed in the poles and in special inserts placed in the shoes. The measurement system is equipped with the necessary data recorders and user interfaces so that the acquired information can be easily analysed. The system is also equipped with a wireless communication module that sends the measured walking parameters to a mobile device (smartphone/tablet). A dedicated application is installed on the mobile device, enabling online/offline monitoring and analysis of the patient’s NW gait by a trainer/physiotherapist [21]. However, before using mechatronic poles in the study of gait biomechanics, it is essential to investigate whether equipping classic NW poles with sensors would cause changes in the gait pattern.
Therefore, the study aimed to compare the biomechanics of free walking of older adults while practising Nordic Walking (NW) using both classic poles and mechatronic ones. It was hypothesised that equipping classic NW poles with sensors would not cause a change in the gait pattern compared to classic NW poles. The study seeks to address a gap in the literature regarding the use of NW for gait improvement in older adults, particularly regarding the effects of mechatronic NW poles on gait patterns. The study also highlights the potential benefits of real-time feedback for improving gait technique, particularly for older adults who may have difficulty learning correct gait techniques without assistance. The study provides vital information for healthcare professionals, researchers, and technology developers and contributes to the development of evidence-based interventions for improving gait and mobility in the older population.
2. Materials and Methods
This was a cross-sectional study with purposive sampling targeting a specific age group (65–75 years) and specific activity levels of amateur NW practitioners.
2.1. Material
The older participants were recruited from a group of University of the Third Age students. Initially, the study group consisted of 11 participants (8 women and 3 men). However, only 7 participants had complete results on three repeated gait measurements out of the individuals enrolled in this study. Exclusion reasons included balance maintenance issues (1 participant), fatigue or weakness (2 participants), and difficulties in using poles properly despite instructions (1 participant). Ultimately, the tests were performed on 7 older adults without a medical history of musculoskeletal injuries causing pain, weakness, decreased ROM, or loss of coordination (5 women and 2 men) aged 65 to 74 (the average age was 70.6), who finally qualified for the study with no comorbidities that could cause gait disturbances and were fit and healthy on the day of the study. They either did not participate regularly in NW classes or had limited experience with NW. The characteristics of the participants are presented in Table 1.

Table 1.
Characteristics of the study group.
The participants were informed about the aims and methodology used in the experiment and gave written informed consent to participate in the investigation. The experiment was approved by the local ethics committee and conducted in accordance with the Declaration of Helsinki.
The participants were equipped with standard NW poles and mechatronic poles. All the poles were individually adjusted to the height of each person. In particular, the pole length was adjusted for flat terrain. Individually adjusting NW pole length involved several steps: (1) Standing up straight with arms relaxed at the sides. (2) Placing the poles on the ground with the handles pointing up. (3) Grasping the handles of the poles and lifting them off the ground. (4) Bending elbows at a 90-degree angle. (5) Adjust the poles’ length until the forearms are parallel to the ground. Participants wore trainers or hiking boots during the experiment. Participants were instructed and trained in the principles of walking with NW poles and performed practice walks with an instructor. Before taking the measurements, all of them reported that they felt comfortable enough with the poles to take part in the study.
The design of the mechatronic poles has been described in our previous studies [20,21]. In short: the classic NW poles have two nine-axis inertial sensors (a three-axis gyroscope, an accelerometer, and a magnetometer). The foot of the pole has a pressure sensor that measures the force along the axis of the pole, and the handle has a contact sensor. In addition, the pole also featured distance sensors, two optical and two ultrasonic, and one sensor of each type at the foot and handle. The conducted signal tests from the inertial, pressure, contact, and distance sensors confirmed sufficient accuracy for the study of gait biomechanics [20,21].
2.2. Methods
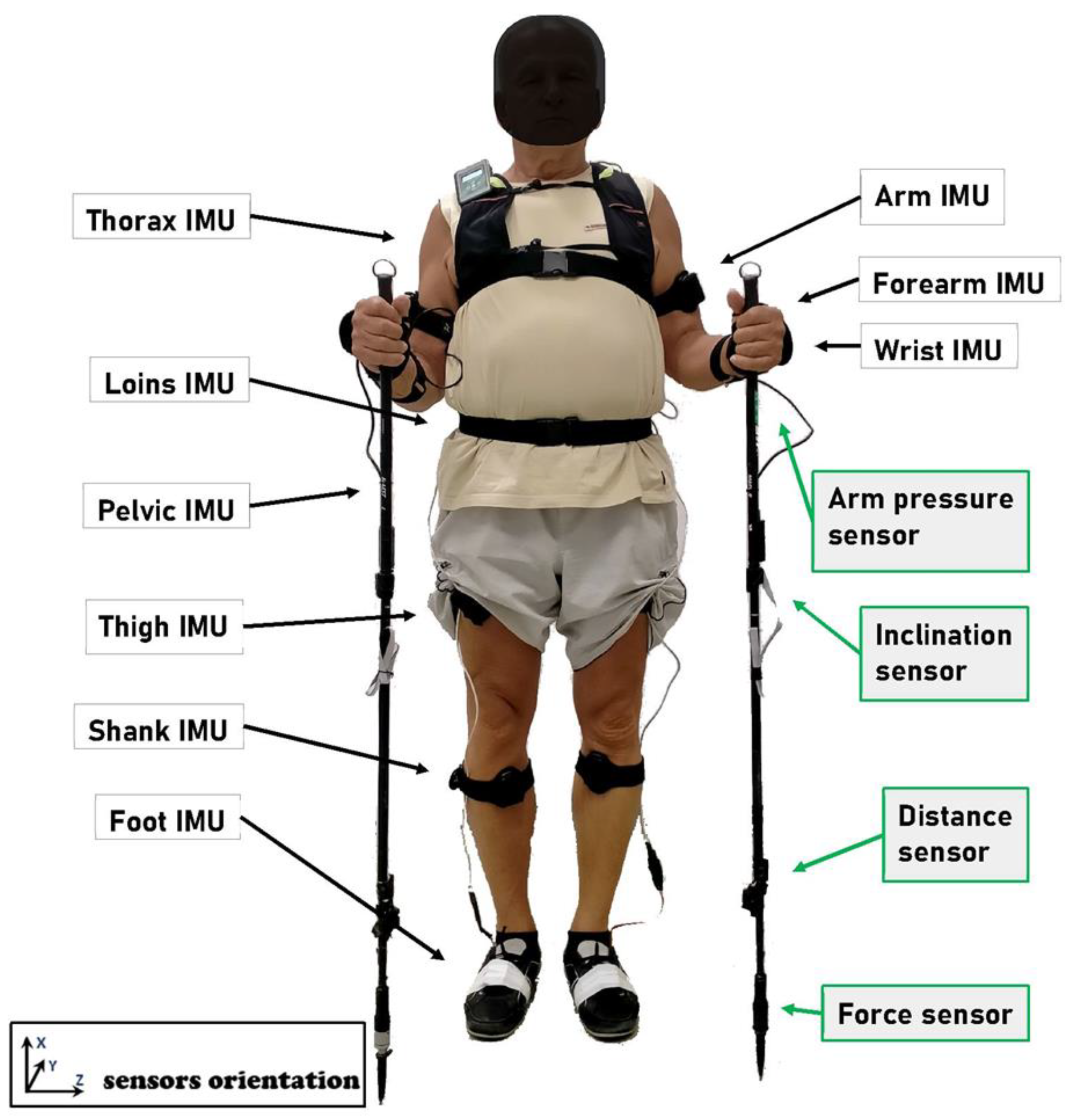
The MyoMOTION MR3 motion analysis system (Noraxon Inc., Scottsdale, AZ, USA) was used to collect the kinematic gait variables. It is a set for three-dimensional motion evaluation using an inertial measurement unit (IMU). The system combines the technology of wireless data transmission and IMU sensors, enabling the assessment of any movement in three-dimensional space (e.g., changes in angles between segments, linear acceleration). Each sensor in the set combines an accelerometer, a gyroscope, and a sensor for measuring the Earth’s magnetic field. The IMU sensors were affixed to the participant’s body following a schema that aligns with the MR3 software’s (version 3.18) requirements. This setup facilitated not only the capture of data but also its thorough analysis, employing a sampling rate of 200 Hz throughout the testing phase. For the purpose of acquiring exhaustive gait metrics, a sum of 15 sensors was utilised—allocating three sensors per extremity (both right and left), along with three sensors positioned along the spinal region (specifically on the spinous processes of the 7th cervical vertebra and 7th thoracic vertebra, as well as within the sacral region), and a single sensor was positioned on the forehead (as illustrated in Figure 1). Prior to every data gathering session, the IMU sensors underwent calibration to ascertain body orientation, employing a stance where the arms were held parallel to the torso, thus establishing a zero-degree angle benchmark for the reference posture.
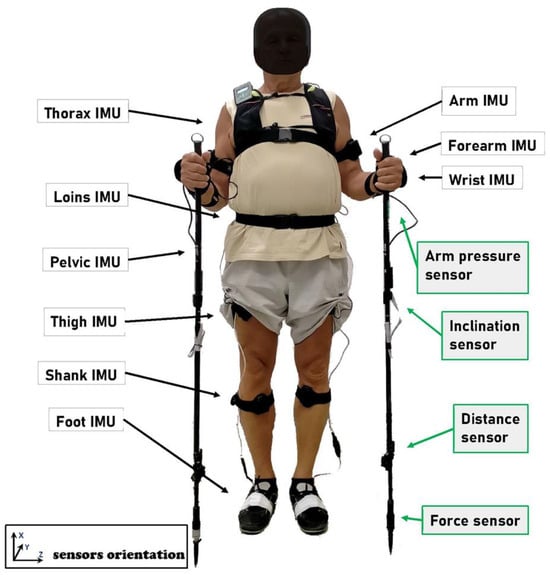
Figure 1.
Illustration of sensors’ placement on the body and the poles. The image was taken upon receiving written permission from the participant.
The participants’ task was to cover a 100-m distance thrice with three types of gait (1) free walking (walking without poles), (2) walking with classic NW poles, and (3) walking with mechatronic poles. The distance was determined based on the literature and resulted from the length of a single and double step (gait cycle) of an adult human [22]. The order of the gait types was randomised to avoid any potential order effects. Before the experiment, each participant was allowed to warm up and stretch for 10 min. The experiment was performed continuously, with no breaks between the different types of gait. The movement with NW poles took place after an NW instructor had given specific instructions. The walk occurred on an artificial surface with participants’ habitual (preferred) walking speed. Two passes were made for each gait type, which allowed for an average of 70 complete gait cycles per pass.
Following the International Society of Biomechanics recommendations [23,24,25], the following parameters were documented for both the right (RT) and left (LT) extremities:
- (a)
- Fifteen spatio-temporal metrics delineating the step cycle structure: Step cadence, measured in steps per minute, which reflects the average step frequency; Stride time duration (s), the interval between the initial contacts of two successive steps by the same foot, indicating the average cycle duration; Step time duration (s), the time from the initial contact of one foot to the initial contact of the opposing foot; The proportions of stance and swing phase durations expressed as a percentage (%) of stride time, representing the stance time as a percentage of the total stride time; The percentage of single support duration (%), the period during which only one foot is in contact with the ground, calculated from the termination of contact by the opposing foot to the initial contact by the same foot, normalised to stride time; Double support (%) signifies the cumulative duration of both feet being in simultaneous contact with the ground, occurring twice at the beginning and end of the stance phase; The loading response (%), also referred to as “foot flat”, quantifies the double support phase from the initial contact until the contralateral foot lifts off the ground (contralateral toe-off); Pre-swing (%) measures the double support phase from the contact of the contralateral foot until the ipsilateral foot lifts off.
- (b)
- The average ROM throughout the cycle, expressed in angular degrees (deg), described the trunk and upper and lower limbs’ movements in relation to the global coordination system:
- regarding the thorax, thoracic movements included flexion-extension, which is the anterior or posterior displacement along the sagittal plane; lateral flexion, which denotes sideways displacement within the frontal plane; and internal-external (axial) rotation, representing rotational movement around the transversal axis.
- regarding the lumbar region, lumbar dynamics encompass flexion-extension, indicating anterior or posterior movement along the sagittal axis; lateral flexion, which refers to sideways movement in the frontal plane; and internal-external (axial) rotation, describing rotational movement around the transversal axis.
- regarding the pelvis, movements were categorised as pelvic tilt, involving anterior or posterior displacement in the sagittal plane; pelvic obliquity, which is the upward or downward movement in the frontal plane; and pelvic (axial) rotation, detailing internal or external rotation within the transverse plane.
- regarding the context of the upper extremity, shoulder movements were classified as flexion-extension, the anterior or posterior movement of the humerus relative to the thorax in the sagittal plane; abduction-adduction: the lateral movement of the humerus relative to the thorax in the frontal plane; and internal-external rotation: the rotational movement of the humerus in the transverse plane. Elbow movements included flexion-extension, the movement of the forearm in relation to the humerus across the transversal axis; wrist dynamics involve flexion-extension, the movement in relation to the radius along the transversal axis, measured between upper arm and hand sensors; wrist radial-ulnar deviation: the sideward movement in relation to the radius, assessed between the upper arm and hand sensors; and wrist supination-pronation: the rotational movement around the axis, quantified between the upper arm and hand sensors.
- regarding the lower extremity, hip movements encompass flexion-extension, the movement of the femur in the sagittal plane around the mediolateral axis; abduction-adduction, the lateral movement of the femur in relation to the pelvis in the frontal plane; and hip rotation, the rotational movement around the proximal-distal axis in the transverse plane. Knee dynamics include flexion-extension: the movement of the tibia in relation to the femur in the sagittal plane. Ankle movements were categorised as dorsi-plantar flexion, the movement of the foot in relation to the tibia in the sagittal plane; ab-adduction, the lateral movement in the transverse (global) plane; and inversion-eversion, the sideward movement in the frontal (global) plane.
For each gait parameter for each participant, the mean and standard deviation were calculated and averaged over the gait cycles.
2.3. Statistical Analysis
Multiple imputation techniques were employed to ensure the robustness of the statistical analyses. Any missing values or outliers in the dataset were identified and imputed using the expectation-maximization algorithm, which utilises the observed data to estimate missing values. Basic descriptive statistics were calculated for all variables, and the distribution’s normality was checked using the Shapiro–Wilk test. The differences between the parameters measured in three measurements during free walking and walking with standard and mechatronic poles were checked by repeated-measurements ANOVA, taking into account the right and left sides of the measurement as a possible differentiating factor allowing for the examination of interactions between walking conditions and laterality. Several precautions were taken to ensure the study’s internal and external validity. We utilised standardised procedures and tools to collect and analyse data and recruited participants with specific inclusion criteria to reduce the risk of bias. Additionally, we conducted a thorough data analysis to identify any potential confounding variables or sources of error. For a two-way ANOVA, critical statistical power was set at 80% and an effect size of at least 0.25 (RMSSE—Root Mean Square Standardized Effect), the estimated minimum sample size was 40 [26]. The Box’s M test verified homogeneity of variances, sphericity by Mauchly’s test, Greenhouse–Geisser correction, and multivariate tests with Wilks’ lambda were used if necessary. Tukey’s post hoc test was used for multiple comparisons. In the case of violation of the ANOVA assumptions, the Friedman test and the Dunn–Bonferroni post hoc test were used. These methods enabled the researchers to delve into subgroup analyses and interactions. In addition to the primary statistical analyses, sensitivity analyses were conducted to assess the robustness of our findings. These analyses involved varying key assumptions and parameters, such as the inclusion and exclusion criteria for participants and the handling of missing data and outliers, to evaluate their impact on the study’s outcomes. All analyses were performed using Statistica 13.3.0 (TIBCO Software Inc., Palo Alto, CA, USA). The statistical significance of the results was accepted at p < 0.05.
3. Results
3.1. Spatio-Temporal Parameters
The results of all the analysed kinematic parameters of gait across three measurements: without poles (1), with standard poles (2), and with mechatronic poles (3) were presented for a group of seven participants as mean ± standard deviation (M ± SD). Regarding spatio-temporal parameters, the only observed difference was the stride time between free walking and walking with standard walking poles (Table 2). For all spatio-temporal, as in the case of ranges of motion, no significant asymmetry was found between the right and left sides of the measurement, regardless of the use of poles and their type (p > 0.05).
Table 2.
Differences between the measurements of the spatio-temporal parameters of gait: “without a pole” (1) vs. “with a standard pole” (2) vs. “with a mechatronic pole” (3) in the group of older adults (n = 7).
3.2. Kinematic Gait Parameters
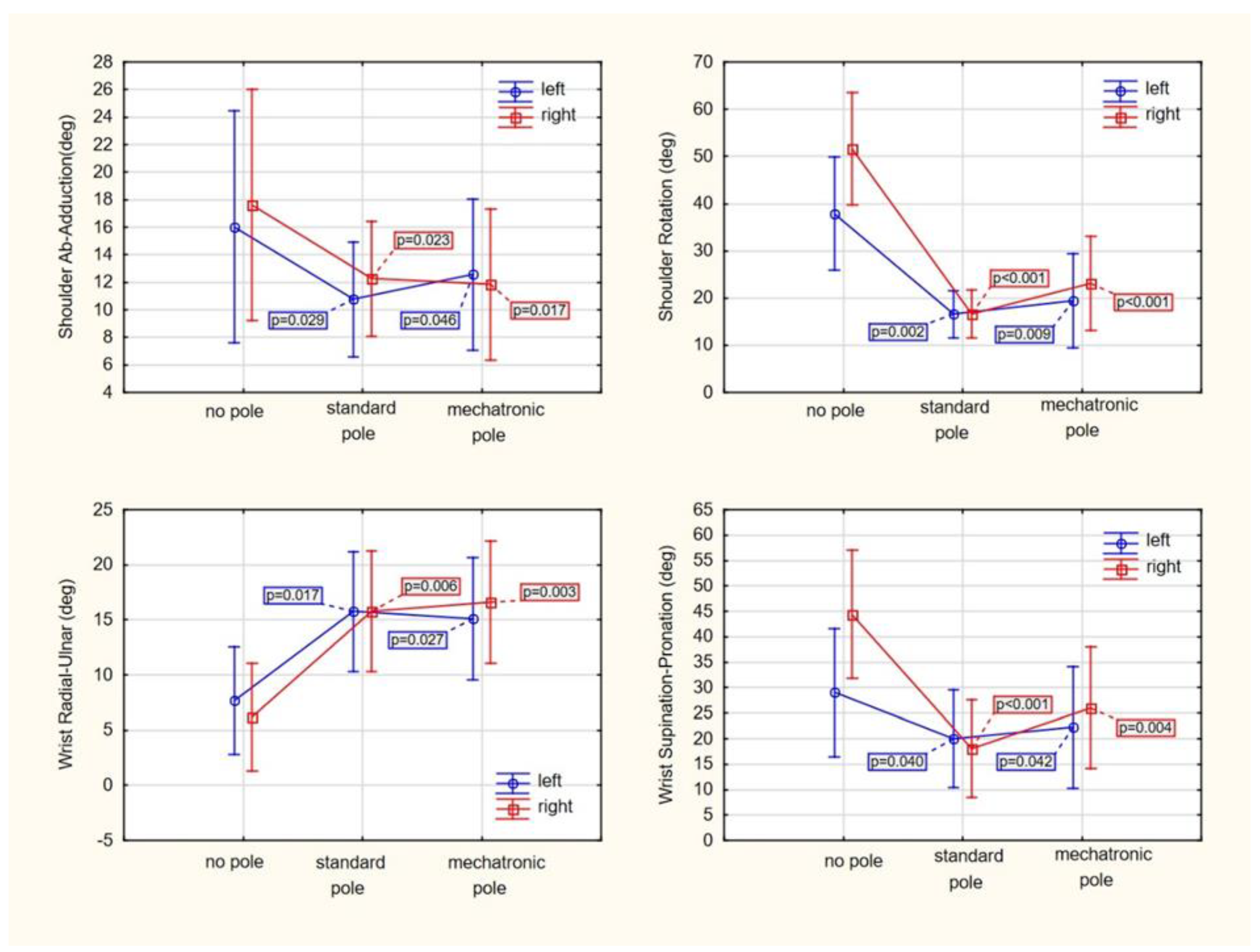
As depicted in Table 3, the outcomes related to the kinematic variables involved in mobility measurement are presented. For the majority of the ROM parameters, no noticeable distinctions among individual measurements were observed, except for shoulder abduction-adduction LT and RT, shoulder internal-external rotation LT and RT, wrist radial-ulnar LT and RT, and wrist supination-pronation LT and RT. These specific variables, as illustrated in Figure 2, only demonstrated visible dissimilarities between free walking and pole walking, irrespective of the left or right side of the measurement. Intriguingly, the type of poles utilised did not induce any changes. During the act of walking with poles, a reduction in the angles of arm abduction and rotation, as well as wrist supination, was observed. This reduction was estimated to be approximately 20–30%, with no significant variations between the left and right limbs or between the types of poles. In addition, a significant (more than double) increase in the wrist radial-ulnar value was noted. However, the interactions between the side of measurement (left versus right) and the type of pole (standard versus mechatronic), as depicted in the individual graphs of Figure 2, were not statistically significant (p > 0.05).
Table 3.
Differences between the measurements of the kinematic parameters of gait: “without a pole” (1) vs. “with a standard pole” (2) vs. “with a mechatronic pole” (3) among participants of the University of the Third Age (n = 7).
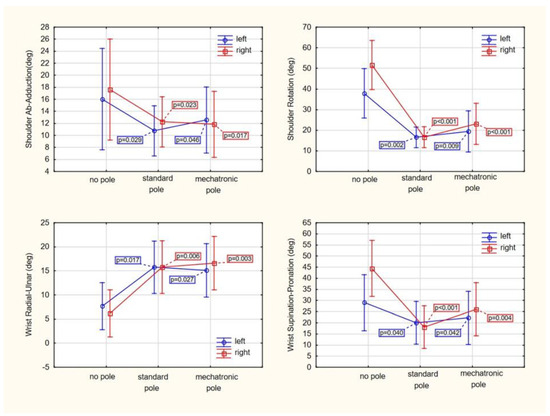
Figure 2.
The utilisation of either standard or mechatronic poles leads to alterations in selected gait kinematic parameters. It’s important to note that the p-values derived from Tukey’s post hoc analysis signify variances in walking with poles as compared to standard walking without poles. The mean values, represented by points with vertical segments, hold a 95% confidence level, indicating their statistical significance.
4. Discussion
The literature lacks studies comparing the free gait with the NW gait of healthy elderly individuals, which would allow the development of an NW gait pattern. Most studies focus on the use of NW as a training method to improve the efficiency of elderly individuals or for specific conditions stemming from functional deficits associated with circulatory, vascular, locomotor, and nervous system diseases. This limits the possibility of comparing the results of our research with those of other authors.
The authors’ research showed only statistically significant differences in 4 out of 37 analysed kinematic parameters and one (stride time) statistically significant difference in spatio-temporal parameters of free walking, walking with classic NW poles, and mechatronic poles among elderly individuals with no prior experience in NW.
In our study, there were no changes characteristic of the NW gait compared to the free walking shown in the studies of other authors: greater stride length, shorter cadence, greater mobility ranges in the joints of the upper and lower limbs, and muscle involvement, especially in the hip and ankle joints [12,27].
Our previous research on the gait of NW instructors with classic and mechatronic poles revealed most of the significant differences in time parameters (stance phase, swing phase, single support, double support, loading response, and pre-swing) between the three types of gait, which differences were not confirmed in older people. The analysis of the kinematic parameters of gait in the group of NW instructors and older people showed significant differences in wrist radial-ulnar and wrist supination-pronation. In the remaining parameters regarding the joints of the upper limb, no significant differences were confirmed among the NW instructors. In the parameters relating to the joints of the lower limb in the group of NW instructors, significant differences were found for hip flexion-extension, ankle ab/adduction, and ankle inversion–eversion. No significant differences in the group of elderly people were confirmed for kinematic parameters of lower limb joints and trunk movements [28].
The observations of other authors, who showed an extension of double and single support during the NW gait of older adults compared to free walking (without poles), have also not been confirmed [13]. This may result from the study of people with various levels of physical fitness and the advancement of their NW technique, which significantly limits the possibility of a reliable comparison of the results obtained by different authors.
On the other hand, the presence of only one statistically significant difference in the spatio-temporal parameters and the lack of significance of the vast majority of kinematic parameters in our study indicate that older people use free walking patterns during NW walking, meaning that they do not make use of the possibilities offered by walking poles. This outcome could be attributed to factors such as habitual walking patterns deeply ingrained over the years, a lack of specific training to effectively use the poles, or possibly the cognitive and physical adaptability required for older adults to modify established motor patterns.
Among the significant differences in kinematic parameters, in our study, higher values of shoulder ab/adduction, shoulder internal-external rotation, and wrist supination-pronation during free walking were found compared to the NW gait, which may indicate that poles constituted a kind of change in the movement pattern, limiting/inhibiting the range of the movements mentioned above in the joints of the upper and lower limbs. They did not support the appropriate phases of gait, and in some way, they even made it difficult to perform them.
Proper cooperation of the upper limbs and lower limbs during walking, which requires the appropriate range of motion in their joints, ensures the required walking speed and balance, reducing the risk of falling [27]. In the case of the older participants, who had no experience in NW, the poles in the initial period of their use could be an aid and even an obstacle during walking. Therefore, at the stage of learning NW, special care should be taken, especially in the case of older people and people with reduced physical fitness. Slightly different results were obtained by Boccia et al. [29]. They found that the NW gait does not increase the complexity of movement control and does not change the coordination of the muscles of the lower limbs, suggesting that it is a physical activity suitable also for people with low motor skills [29]. Perhaps the reason for these differences is the study of different age populations, as the influence of the NW gait on its biomechanics cannot be ruled out, depending on the age of the tested people or measurements performed in different conditions, e.g., at different walking speeds.
On the other hand, higher values of wrist radial-ulnar during NW compared to free gait are perhaps the first and the earliest manifestation of this gait technique by people who have not previously practised walking with poles.
The lack of significant differences in most of the spatio-temporal and kinematic parameters of the NW gait with classic poles and mechatronic poles in older adults indicates that additional sensors mounted on the pole did not constitute a factor that would increase the difficulty of using this pole and change the pattern of movement. Taking into account the previous comments on the limitations of the use of classic NW poles by older adults not prepared for this type of gait, after their elimination, i.e., a basic mastery of the technique of this gait, mechatronic poles could be a reliable method of analysis and information on the biomechanics of NW gait in real time.
5. Limitations of the Conducted Study
The discussed study was performed in a relatively small group of people with a 2-fold majority of women over men. Firstly, a small number of participants increases the risk of statistical error, and sex disproportion may also be a variable confusing the obtained findings. This was influenced by the COVID-19 pandemic, which significantly impeded recruitment for the study, as older adults were at increased risk of infection with the Sars-CoV-2 coronavirus. Nevertheless, in the future, similar studies should be performed on a larger group of people, considering sex as an independent variable.
As a final point, the use of IMU sensors itself may potentially influence gait patterns. To address this concern, we took several precautions to minimise the potential influence of the system sensors. Firstly, we followed standardised procedures for placing the sensors on the body and poles, as recommended by the manufacturer of the system. We also calibrated the system before each participant’s testing session to ensure accurate measurement of motion data. Secondly, we asked all participants to wear comfortable clothing and shoes during the testing session to minimise any additional effects on their gait pattern. Finally, we acknowledge that previous studies [30,31] and our own studies [32,33] have shown that the presence of IMU sensors does not interfere with natural movement nor alter gait patterns, and any differences in joint angle measurement can be attributed to the variability in the anatomical models used for calculations. The MyoMOTION MR3 sensors used in our study are small, lightweight, and wireless and are attached directly to the body and poles.
6. Conclusions
In light of our findings and in comparison with other studies, it is evident that the expected biomechanical advantages of the NW gait, such as reduced cadence and enhanced joint mobility, were not observed in our cohort of older adults. This discrepancy suggests that without specific training and adaptation, older individuals may not automatically derive the potential biomechanical benefits of NW, underscoring the critical need for tailored training programs that focus on the correct utilization of NW techniques for this demographic. Furthermore, the study found no significant differences in gait patterns between classic NW poles and mechatronic NW poles equipped with sensors for biomechanical analysis and feedback. The study also observed no significant differences in the involvement of upper and lower limbs between the NW gait and free walking in older adults, suggesting that they did not fully utilise the potential benefits of the NW gait. Finally, the study found that spatio-temporal and kinematic parameters were symmetric between the right and left sides in classic and mechatronic NW gait in older adults. These findings contribute to a better understanding of the potential benefits of NW for older adults and highlight the importance of mastering the correct gait technique to realise these benefits fully.
Author Contributions
Conceptualization, A.S., S.W. (Sławomir Winiarski), J.B., R.J., T.N., A.L., S.W. (Sławomir Wudarczyk) and M.W.; methodology, A.S., B.P., R.J., T.N., A.L. and K.L.; software, S.W. (Sławomir Winiarski), S.W. (Sławomir Wudarczyk); validation, M.K., B.P., R.J., T.N., A.L., K.L., S.W. (Sławomir Wudarczyk) and S.W. (Sławomir Winiarski); formal analysis, M.K. and K.L.; investigation, B.P., A.L. and S.W. (Sławomir Wudarczyk); resources, B.P., R.J. and T.N.; data curation, M.K. and K.L.; writing—original draft preparation, A.S. and M.K.; writing—review and editing, A.S. and S.W. (Sławomir Winiarski); visualisation, A.S. and S.W. (Sławomir Winiarski); supervision, M.W. and J.B.; project administration, M.W. and J.B.; funding acquisition, M.W. and J.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Science Centre, Poland (grant number 2016/23/B/NZ7/03310).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the Wroclaw University of Health and Sport Sciences, Mickiewicza 58 Street, 51-684 Wrocław, Poland (Reg. No 40/2019 issued on 15 November 2019).
Informed Consent Statement
Written informed consent has been obtained from all patient(s) to publish this paper (in accordance with PN-EN ISO 9001:2001 procedures).
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this article. The funders had no role in the design of the study; in the collection, analysis, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Alexander, N.B. Gait Disorders in Older Adults. J. Am. Geriatr. Soc. 1996, 44, 434–451. [Google Scholar] [CrossRef]
- Bywalec, R. Gait disorders—One problem, different points of view. Geriatria 2018, 12, 29–34. (In Polish) [Google Scholar]
- Callisaya, M.L.; Blizzard, L.; Schmidt, M.D.; McGinley, J.L.; Srikanth, V.K. Ageing and gait variability—A population-based study of older people. Age Ageing 2010, 39, 191–197. [Google Scholar] [CrossRef]
- Watelain, E.; Barbier, F.; Allard, P.; Thevenon, A.; Angue, J.C. Gait pattern classification of healthy elderly men based on biomechanical data. Arch. Phys. Med. Rehabil. 2000, 81, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Gomeñuka, N.A.; Oliveira, H.B.; Silva, E.S.; Costa, R.R.; Kanitz, A.C.; Liedtke, G.V.; Schuch, F.B.; Peyré-Tartaruga, L.A. Effects of Nordic walking training on quality of life, balance and functional mobility in elderly: A randomized clinical trial. PLoS ONE 2019, 14, e0211472. [Google Scholar] [CrossRef] [PubMed]
- Ostrosky, K.M.; VanSwearingen, J.M.; Burdett, R.G.; Gee, Z. A comparison of gait characteristics in young and old subjects. Phys. Ther. 1994, 74, 637–644. [Google Scholar] [CrossRef]
- Jiménez-García, J.D.; Ortega-Gómez, S.; Martínez-Amat, A.; Álvarez-Salvago, F. Associations of Balance, Strength, and Gait Speed with Cognitive Function in Older Individuals over 60 Years: A Cross-Sectional Study. Appl. Sci. 2024, 14, 1500. [Google Scholar] [CrossRef]
- Gomeñuka, N.A.; Oliveira, H.B.; da Silva, E.S.; Passos-Monteiro, E.; da Rosa, R.G.; Carvalho, A.R.; Costa, R.R.; Paz, M.C.R.; Pellegrini, B.; Peyré-Tartaruga, L.A. Nordic walking training in elderly, a randomized clinical trial. Part II: Biomechanical and metabolic adaptations. Sport Med.-Open 2020, 6, 3. [Google Scholar] [CrossRef]
- Pirker, W.; Katzenschlager, R. Gait disorders in adults and the elderly. Wien. Klin. Wochenschr. 2017, 129, 81–95. [Google Scholar] [CrossRef]
- Satoh, Y.; Yamada, T.; Shimamura, R.; Ohmi, T. Comparison of foot kinetics and kinematics during gait initiation between young and elderly participants. J. Phys. Ther. Sci. 2019, 31, 498–503. [Google Scholar] [CrossRef]
- Rodrigues, I.B.; Ponzano, M.; Butt, D.A.; Bartley, J.; Bardai, Z.; Ashe, M.C.; Chilibeck, P.D.; Thabane, L.; Wark, J.D.; Stapleton, J.; et al. The Effects of Walking or Nordic Walking in Adults 50 Years and Older at Elevated Risk of Fractures: A Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2021, 29, 886–899. [Google Scholar] [CrossRef]
- Roy, M.; Grattard, V.; Dinet, C.; Soares, A.V.; Decavel, P.; Sagawa, Y.J. Nordic walking influence on biomechanical parameters: A systematic review. Eur. J. Phys. Rehabil. Med. 2020, 56, 607–615. [Google Scholar] [CrossRef]
- Dalton, C.M.; Nantel, J. Substantiating Appropriate Motion Capture Techniques for the Assessment of Nordic Walking Gait and Posture in Older Adults. J. Vis. Exp. 2016, 111, e53926. [Google Scholar] [CrossRef]
- Takeshima, N.; Islam, M.M.; Rogers, M.E.; Rogers, N.L.; Sengoku, N.; Koizumi, D.; Kitabayashi, Y.; Imai, A.; Naruse, A. Effects of Nordic Walking Compared to Conventional Walking and Band-Based Resistance Exercise on Fitness in Older Adults. J. Sports Sci. Med. 2013, 12, 422–430. [Google Scholar] [PubMed]
- Bullo, V.; Gobbo, S.; Vendramin, B.; Duregon, F.; Cugusi, L.; di Blasio, A.; Bocalini, D.S.; Zaccaria, M.; Bergamin, M.; Ermolao, A. Nordic Walking Can Be Incorporated in the Exercise Prescription to Increase Aerobic Capacity, Strength, and Quality of Life for Elderly: A Systematic Review and Meta-Analysis. Rejuvenation Res. 2018, 21, 141–161. [Google Scholar] [CrossRef] [PubMed]
- Cokorilo, N.; Ruiz-Montero, P.J.; González-Fernández, F.T.; Martín-Moya, R. An Intervention of 12 Weeks of Nordic Walking and Recreational Walking to Improve Cardiorespiratory Capacity and Fitness in Older Adult Women. J. Clin. Med. 2022, 11, 2900. [Google Scholar] [CrossRef]
- Sengoku, N.; Koizumi, D.; Takeshima, N. Effects of Nordic walking on functional fitness in older adults. Jpn. J. Phys. Educ. Health Sports Sci. 2012, 5, 449–454. [Google Scholar] [CrossRef]
- Fujita, E.; Yakushi, K.; Takeda, M.; Islam, M.M.; Nakagaichi, M.; Taaffe, D.R.; Takeshima, N. Proficiency in pole handling during Nordic walking influences exercise effectiveness in middle-aged and older adults. PLoS ONE 2018, 13, e0208070. [Google Scholar] [CrossRef]
- Mocera, F.; Aquilino, G.; Somà, A. Nordic Walking Performance Analysis with an Integrated Monitoring System. Sensors 2018, 18, 1505. [Google Scholar] [CrossRef]
- Wudarczyk, S.; Lewandowski, B.; Niebudek, T.; Szrek, J.; Mróz, S.F.; Woźniewski, M.; Bałchanowski, J.; Jasiński, R. Research on the mechatronic gait monitoring system with Nordic Walking poles. In Proceedings of the 15th International Conference Mechatronic Systems and Materials, MSM 2020, Bialystok, Poland, 1–3 July 2020; IEEE Cop.: Piscataway, NJ, USA, 2020; pp. 1–6. [Google Scholar]
- Wudarczyk, S.; Wozniewski, M.; Szpala, A.; Winiarski, S.; Bałchanowski, J. Mechatronic Pole System for Monitoring the Correctness of Nordic Walking. Sensors 2023, 23, 8436. [Google Scholar] [CrossRef]
- Park, S.K.; Yang, D.J.; Kang, Y.H.; Kim, J.H.; Uhm, Y.H.Y.; Lee, Y.S. Effects of Nordic walking and walking on spatiotemporal gait parameters and ground reaction force. J. Phys. Ther. Sci. 2015, 27, 2891–2893. [Google Scholar] [CrossRef]
- Wu, G.; Cavanagh, P.R. ISB recommendations for standardization in the reporting of kinematic data. J. Biomech. 1995, 28, 1257–1261. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; van der Helm, F.C.T.; Veeger, H.E.J.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. Available online: http://www.jstor.org/stable/20182143 (accessed on 23 November 2023). [CrossRef]
- Trzaskoma, Z.; Molik, B.; Morgulec-Adamowicz, N.; Truszczyńska-Baszak, A.; Ogonowska-Słodownik, A.; Marszałek, J.; Stępień, A.; Krawczyk, M.; Wójcik, A. Identification of the forces developed by upper limbs in various forms of human physical activity and in manual techniques used by physiotherapists—A brief review. Adv. Rehabil. 2017, 31, 59–70. [Google Scholar] [CrossRef]
- Szpala, A.; Winiarski, S.; Kołodziej, M.; Pietraszewski, B.; Jasiński, R.; Niebudek, T.; Lejczak, A.; Lorek, K.; Bałchanowski, K.J.; Wudarczyk, S.; et al. No influence of mechatronic poles on the movement pattern of professional Nordic walkers. Int. J. Environ. Res. Public Health 2023, 20, 163. [Google Scholar] [CrossRef] [PubMed]
- Boccia, G.; Zoppirolli, C.; Bortolan, L.; Schena, F.; Pellegrini, B. Shared and task-specific muscle synergies of Nordic walking and conventional walking. Scand. J. Med. Sci. Sports 2018, 28, 905–918. [Google Scholar] [CrossRef] [PubMed]
- Cottam, D.S.; Campbell, A.C.; Davey, M.P.C.; Kent, P.; Elliott, B.C.; Alderson, J.A. Measurement of uni-planar and sport specific trunk motion using magneto-inertial measurement units: The concurrent validity of Noraxon and Xsens systems relative to a retro-reflective system. Gait Posture 2022, 92, 129–134. [Google Scholar] [CrossRef]
- Mundt, M.; Thomsen, W.; David, S.; Dupré, T.; Bamer, F.; Potthast, W.; Markert, B. Assessment of the measurement accuracy of inertial sensors during different tasks of daily living. J. Biomech. 2019, 84, 81–86. [Google Scholar] [CrossRef]
- Szpala, A.; Kołodziej, M.; Struzik, A.; Jasiński, R.; Bałchanowski, K.J.; Pietraszewski, B.; Woźniewski, M. Selected spatiotemporal and joint angle parameters in normal gait and Nordic walking with classical and mechatronic poles in aspects of sex differences. BioMed Res. Int. 2022, 2022, 7905120. [Google Scholar] [CrossRef] [PubMed]
- Szpala, A.; Winiarski, S.; Kołodziej, M.; Pietraszewski, B.; Jasiński, R.; Niebudek, T.; Lejczak, A.; Kałka, D.; Lorek, K.; Bałchanowski, K.J.; et al. Do mechatronic poles change the gait technique of Nordic walking in patients with ischemic heart disease? Appl. Bionics Biomech. 2023, 2023, 1135733. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).