

Analysis of Visual Risk Factors of Anterior Cruciate Ligament Injury of Knee Joint
 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Statement of Informed Consent and Ethical Board Approval
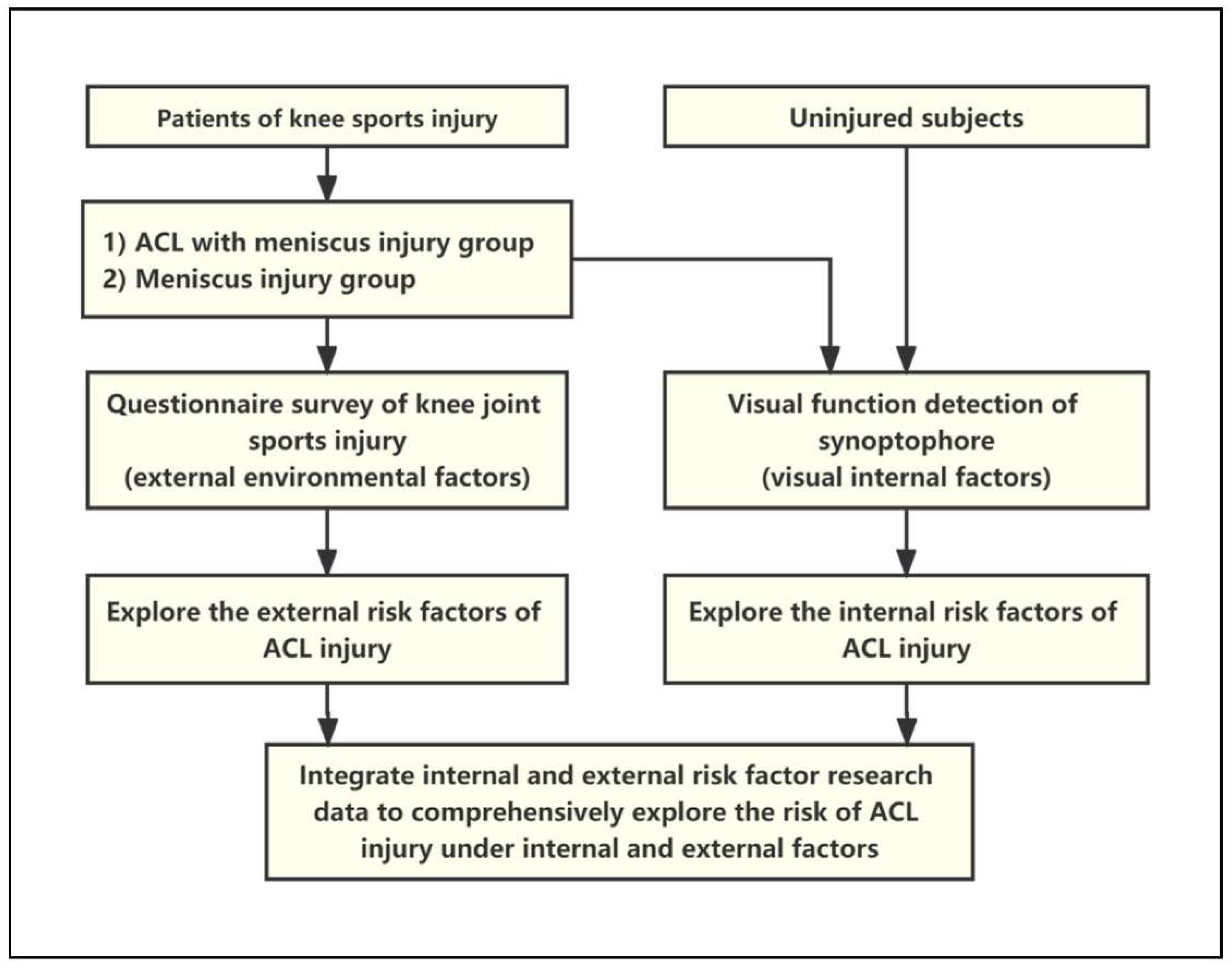
2.2. Study Design and Data Collection
2.3. Statistical Analysis
3. Results
3.1. Eye Disease Is a Major Risk Factor of ACL Injury from Questionnaires
3.2. Low Visual Fusion Range Is a Major Risk Factor for ACL Injury from Visual Examination
3.3. Low Visual Fusion Range Combined with Extrinsic Factors Increases the Risk of ACL Injury
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Janssen, K.W.; Orchard, J.W.; Driscoll, T.R.; van Mechelen, W. High incidence and costs for anterior cruciate ligament reconstructions performed in Australia from 2003–2004 to 2007–2008: Time for an anterior cruciate ligament register by Scandinavian model? Scand. J. Med. Sci. Sports 2012, 22, 495–501. [Google Scholar] [CrossRef] [PubMed]
- von Porat, A.; Roos, E.M.; Roos, H. High prevalence of osteoarthritis 14 years after an anterior cruciate ligament tear in male soccer players: A study of radiographic and patient relevant outcomes. Ann. Rheum. Dis. 2004, 63, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Lohmander, L.S.; Englund, P.M.; Dahl, L.L.; Roos, E.M. The long-term consequence of anterior cruciate ligament and meniscus injuries: Osteoarthritis. Am. J. Sports Med. 2007, 35, 1756–1769. [Google Scholar] [CrossRef] [PubMed]
- Atik, O.S.; Kaya, I. Is it possible to prevent ACL injury? Jt. Dis. Relat. Surg. 2022, 33, 263–264. [Google Scholar] [CrossRef] [PubMed]
- Hodel, S. Introducing the Lateral Femoral Condyle Index as a Risk Factor for Anterior Cruciate Ligament Injury: Response. Am. J. Sports Med. 2020, 48, NP42–NP43. [Google Scholar] [CrossRef]
- O’Connor, S.; McCaffrey, N.; Whyte, E.F.; Fop, M.; Murphy, B.; Moran, K. Can the Y balance test identify those at risk of contact or non-contact lower extremity injury in adolescent and collegiate Gaelic games? J. Sci. Med. Sport 2020, 23, 943–948. [Google Scholar] [CrossRef]
- Horoupian, D.S.; Kress, Y.; Yen, S.H.; Gaskin, F. Nickel-induced changes and reappraisal of Rosenthal fibers in focal CNS lesions. J. Neuropathol. Exp. Neurol. 1982, 41, 664–675. [Google Scholar] [CrossRef]
- Alsubaie, S.F.; Abdelbasset, W.K.; Alkathiry, A.A.; Alshehri, W.M.; Azyabi, M.M.; Alanazi, B.B.; Alomereni, A.A.; Asiri, F.Y. Anterior cruciate ligament injury patterns and their relationship to fatigue and physical fitness levels—A cross-sectional study. Medicine 2021, 100, e24171. [Google Scholar] [CrossRef]
- Tomomitsu, M.S.; Alonso, A.C.; Morimoto, E.; Bobbio, T.G.; Greve, J.M. Static and dynamic postural control in low-vision and normal-vision adults. Clinics 2013, 68, 517–521. [Google Scholar] [CrossRef]
- Helbostad, J.L.; Vereijken, B.; Hesseberg, K.; Sletvold, O. Altered vision destabilizes gait in older persons. Gait Posture 2009, 30, 233–238. [Google Scholar] [CrossRef]
- Adamek, B.; Karczewicz, D. The dependence of the range of fusion on some selected functions of the visual system. Part I: Study on convergent and divergent fusion. Klin Oczna 2006, 108, 163–166. [Google Scholar] [PubMed]
- Parker, A.J.; Smith, J.E.; Krug, K. Neural architectures for stereo vision. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2016, 371, 20150261. [Google Scholar] [CrossRef] [PubMed]
- Bridge, H. Effects of cortical damage on binocular depth perception. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2016, 371, 20150254. [Google Scholar] [CrossRef] [PubMed]
- Banstola, S.; Hanna, K.; O’Connor, A. Changes to Visual Parameters Following Virtual Reality Gameplay. Br. Ir. Orthopt. J. 2022, 18, 57–64. [Google Scholar] [CrossRef]
- Ngatuvai, M.S.; Yang, J.; Kistamgari, S.; Collins, C.L.; Smith, G.A. Epidemiological Comparison of ACL Injuries on Different Playing Surfaces in High School Football and Soccer. Orthop. J. Sports Med. 2022, 10, 23259671221092321. [Google Scholar] [CrossRef]
- Loughran, G.J.; Vulpis, C.T.; Murphy, J.P.; Weiner, D.A.; Svoboda, S.J.; Hinton, R.Y.; Milzman, D.P. Incidence of Knee Injuries on Artificial Turf Versus Natural Grass in National Collegiate Athletic Association American Football: 2004–2005 Through 2013–2014 Seasons. Am. J. Sports Med. 2019, 47, 1294–1301. [Google Scholar] [CrossRef]
- Balazs, G.C.; Pavey, G.J.; Brelin, A.M.; Pickett, A.; Keblish, D.J.; Rue, J.P. Risk of Anterior Cruciate Ligament Injury in Athletes on Synthetic Playing Surfaces: A Systematic Review. Am. J. Sports Med. 2015, 43, 1798–1804. [Google Scholar] [CrossRef]
- Johnson, W.R.; Mian, A.; Donnelly, C.J.; Lloyd, D.; Alderson, J. Predicting athlete ground reaction forces and moments from motion capture. Med. Biol. Eng. Comput. 2018, 56, 1781–1792. [Google Scholar] [CrossRef]
- Cronstrom, A.; Creaby, M.W.; Ageberg, E. Do knee abduction kinematics and kinetics predict future anterior cruciate ligament injury risk? A systematic review and meta-analysis of prospective studies. BMC Musculoskelet. Disord. 2020, 21, 563. [Google Scholar] [CrossRef]
- Arendt, E.; Dick, R. Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. Am. J. Sports Med. 1995, 23, 694–701. [Google Scholar] [CrossRef]
- Arendt, E.A.; Agel, J.; Dick, R. Anterior cruciate ligament injury patterns among collegiate men and women. J. Athl. Train. 1999, 34, 86–92. [Google Scholar] [PubMed]
- Hughes, G. A review of recent perspectives on biomechanical risk factors associated with anterior cruciate ligament injury. Res. Sports Med. 2014, 22, 193–212. [Google Scholar] [CrossRef] [PubMed]
- Bates, N.A.; Schilaty, N.D.; Nagelli, C.V.; Krych, A.J.; Hewett, T.E. Validation of Noncontact Anterior Cruciate Ligament Tears Produced by a Mechanical Impact Simulator Against the Clinical Presentation of Injury. Am. J. Sports Med. 2018, 46, 2113–2121. [Google Scholar] [CrossRef] [PubMed]
- Kaeding, C.C.; Leger-St-Jean, B.; Magnussen, R.A. Epidemiology and Diagnosis of Anterior Cruciate Ligament Injuries. Clin. Sports Med. 2017, 36, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.K.; Gupta, T.P.; Singh, V.B.; Kale, A.; Vij, V.; Shaki, O. Retrospective analysis and risk of progression of partial anterior cruciate ligament injuries in a young population. Arch. Orthop. Trauma Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Fooken, J.; Lalonde, K.M.; Mann, G.K.; Spering, M. Eye movement training is most effective when it involves a task-relevant sensorimotor decision. J. Vis. 2018, 18, 18. [Google Scholar] [CrossRef]
- Caldani, S.; Delorme, R.; Moscoso, A.; Septier, M.; Acquaviva, E.; Bucci, M.P. Improvement of Pursuit Eye Movement Alterations after Short Visuo-Attentional Training in ADHD. Brain Sci. 2020, 10, 816. [Google Scholar] [CrossRef]
- Sahraie, A.; Cederblad, A.M.H.; Kenkel, S.; Romano, J.G. Efficacy and predictors of recovery of function after eye movement training in 296 hemianopic patients. Cortex 2020, 125, 149–160. [Google Scholar] [CrossRef]

{kind=link}
| ACL-I | ACL-D | T (χ2) | p-Value | |
|---|---|---|---|---|
| Total | 133 (46.34%) | 154 (53.66%) | ||
| Sex | 0.095 | |||
| Male | 95 (71.43%) | 123 (79.87%) | 2.785 | |
| Female | 38 (28.57%) | 31 (20.13%) | ||
| Age (year) | 30.10 ± 10.24 | 28.31 ± 9.49 | 1.538 | 0.288 |
| Weight (kg) | 66.13 ± 13.21 | 69.39 ± 12.14 | −2.173 | 0.464 |
| Body Mass Index (kg/m2) | 22.76 ± 3.24 | 23.46 ± 2.89 | −1.936 | 0.222 |
| Injury Side | 0.001 | 0.976 | ||
| Dominant | 84 (63.16%) | 97 (62.99%) | ||
| Non-Dominant | 49 (36.84%) | 57 (37.01%) | ||
| Injury Action | 0.010 * | |||
| Sprint | 22 (16.54%) | 17 (11.04%) | 15.147 | |
| Quick Turn | 39 (29.32%) | 55 (35.71%) | ||
| Sudden Stop | 5 (3.76%) | 17 (11.04%) | ||
| Jump | 32 (24.06%) | 45 (29.22%) | ||
| Retrogress | 19 (14.29%) | 9 (5.84%) | ||
| Others # | 16 (12.03%) | 11 (7.14%) | ||
| Contact Confrontation | 0.146 | 0.702 | ||
| Yes | 37 (27.82%) | 46 (29.87%) | ||
| No | 96 (72.18%) | 108 (70.13%) | ||
| Site Condition | 8.615 | |||
| Cement Floor | 50 (38.59%) | 63 (40.91%) | ||
| Artificial Turf | 21 (15.79%) | 25 (16.23%) | 0.125 | |
| Wooden Floor | 10 (7.52%) | 15 (9.74%) | ||
| Plastic Floor | 20 (15.04%) | 33 (21.43%) | ||
| Real Turf | 4 (3.01%) | 3 (1.95%) | ||
| Others ## | 28 (21.05%) | 15 (9.74%) | ||
| Weather | 0.965 | 0.915 | ||
| Shine | 109 (81.95%) | 129 (83.77%) | ||
| Cloud | 10 (7.52%) | 13 (8.44%) | ||
| Rain | 6 (4.51%) | 5 (3.25%) | ||
| Snow | 6 (4.51%) | 6 (3.90%) | ||
| Others ### | 2 (1.50%) | 1 (0.65%) | ||
| Vision Right | 4.130 | 0.389 | ||
| Normal | 42 (31.58%) | 57 (37.01%) | ||
| Low Ametropia | 35 (26.32%) | 43 (27.92%) | ||
| Moderate Ametropia | 43 (32.33%) | 46 (29.87%) | ||
| High Ametropia | 11 (8.27%) | 5 (3.25%) | ||
| Unclear | 2 (1.5%) | 3 (1.95%) | ||
| Vision Left | 5.208 | 0.391 | ||
| Normal | 42 (32.58%) | 61 (39.61%) | ||
| Low Ametropia | 38 (28.57%) | 42 (27.27%) | ||
| Moderate Ametropia | 42 (31.58%) | 43 (27.92%) | ||
| High Ametropia | 8 (6.02%) | 4 (2.60%) | ||
| Unclear | 3 (2.26%) | 4 (2.60%) | ||
| Eye Diseases | 8.703 | 0.069 | ||
| Normal | 84 (63.16%) | 79 (51.30%) | ||
| Astigmatism | 40 (30.08%) | 58 (37.66%) | ||
| Amblyopia | 1 (0.75%) | 3 (1.95%) | ||
| Strabismus | 2 (1.50%) | 10 (6.49%) | ||
| Multiple Diseases | 6 (4.51%) | 4 (2.60%) | ||
| Repeated Injuries | 1.022 | 0.312 | ||
| Yes | 45 (33.83%) | 61 (39.61%) | ||
| No | 88 (66.17%) | 93 (60.39%) |
| Chi-Square Statistic | p-Value | |
|---|---|---|
| Age | 2.310 | 0.129 ǂ |
| Sex | 2.763 | 0.096 ǂ |
| Weight | 4.558 | 0.033 * |
| BMI | 3.670 | 0.055 ǂ |
| Injury Side | 0.001 | 0.976 |
| Vision Right | 3.901 | 0.420 |
| Vision Left | 3.916 | 0.562 |
| Eye Diseases | 7.912 | 0.095 ǂ |
| Combat | 0.146 | 0.702 |
| Injury Action | 14.292 | 0.014 * |
| Site Condition | 8.296 | 0.141 ǂ |
| Weather | 0.934 | 0.920 |
| Repeated Injuries | 1.021 | 0.312 |
| Estimate | SE | OR | 95% CI | p-Value | ||
|---|---|---|---|---|---|---|
| Intercept | −0.542 | 0.352 | 0.581 | 0.286 | 1.149 | 0.123 |
| Eye Diseases (Astigmatism) | 0.477 | 0.270 | 1.611 | 0.951 | 2.751 | 0.078 |
| Eye Diseases (Amblyopia) | 1.344 | 1.189 | 3.832 | 0.458 | 80.582 | 0.258 |
| Eye Diseases (Strabismus) | 1.699 | 0.806 | 5.468 | 1.340 | 37.066 | 0.035 * |
| Eye Diseases (Multiple Diseases) | −0.438 | 0.714 | 0.646 | 0.146 | 2.589 | 0.540 |
| Injured Action (Quick Turn) | 0.687 | 0.396 | 1.989 | 0.922 | 4.377 | 0.082 |
| Injured Action (Sudden Stop) | 1.645 | 0.620 | 5.183 | 1.623 | 19.021 | 0.008 * |
| Injured Action (Jump) | 0.608 | 0.408 | 1.837 | 0.830 | 4.139 | 0.136 |
| Injured Action (Retrogress) | −0.447 | 0.535 | 0.640 | 0.218 | 1.805 | 0.404 |
| Injured Action (Others) | 0.034 | 0.523 | 1.035 | 0.367 | 2.886 | 0.948 |
| ACL-I | ACL-D | Control | F (χ2) | p-Value | |
|---|---|---|---|---|---|
| Total (n, %) | 127 (33.69%) | 145 (38.46%) | 105 (27.85%) | 1.412 | 0.494 |
| Male | 92 (72.44%) | 114 (78.62%) | 79 (75.24%) | ||
| Female | 35 (27.56%) | 31 (21.38%) | 26 (24.76%) | ||
| Age (year) | 28.72 ± 8.81 | 27.71 ± 8.23 | 27.61 ± 7.99 | 0.617 | 0.512 |
| Dominant eye | 0.248 | 0.883 | |||
| Right | 106 (83.46%) | 124 (85.52%) | 88 (83.81%) | ||
| Left | 21 (16.54%) | 21 (14.48%) | 17 (16.19%) | ||
| Pupillary Distance | 62.06 ± 2.71 | 62.31 ± 2.76 | 63.23 ± 10.02 | 1.278 | 0.280 |
| Vision Right | 0.74 ± 0.45 | 0.73 ± 0.50 | 0.75 ± 0.39 | 0.035 | 0.966 |
| ≥1.0 | 60 (47.24%) | 63 (43.45%) | 47 (44.76%) | ||
| 0.1~1.0 | 57 (44.88%) | 69 (47.59%) | 49 (46.67%) | ||
| ≤0.01 | 10 (7.87%) | 13 (8.97%) | 9 (8.57%) | ||
| Vision Left | 0.75 ± 0.46 | 0.77 ± 0.50 | 0.75 ± 0.36 | 0.082 | 0.922 |
| ≥1.0 | 59 (46.46%) | 68 (46.90%) | 46 (43.81%) | ||
| 0.1~1.0 | 58 (45.67%) | 66 (45.52%) | 52 (49.52%) | ||
| ≤0.01 | 10 (7.87%) | 11 (7.59%) | 7 (6.67%) | ||
| Oblique Perspective (°) | 1.97 ± 1.91 | 1.99 ± 2.19 | 1.69 ± 1.88 | 0.770 | 0.464 |
| ≥5 | 12 (9.45%) | 23 (15.86%) | 10 (9.52%) | ||
| <5 | 115 (90.55%) | 122 (84.14%) | 95 (90.48%) | ||
| Fusion Range (°) | 20.26 ± 7.27 | 17.82 ± 6.17 | 22.07 ± 5.16 | 14.103 | <0.001 ** |
| ≥25 | 38 (29.92%) | 29 (20.00%) | 30 (28.57%) | ||
| <25 | 89 (70.08%) | 116 (80.00%) | 75 (71.43%) | ||
| Stereoacuity (″) | 221.89 ± 411.15 | 273.93 ± 522.72 | 176.76 ± 361.42 | 1.464 | 0.233 |
| ≤60 | 87 (68.50%) | 97 (66.90%) | 78 (74.29%) | ||
| 60″~800 | 34 (26.77%) | 37 (25.52%) | 24 (22.86%) | ||
| >800 | 6 (4.72%) | 11 (7.59%) | 3 (2.86%) |
| Chi-Square Statistic | p-Value | |
|---|---|---|
| Sex | 1.415 | 0.493 |
| Age | 1.344 | 0.511 |
| Dominant Eye | 2.600 | 0.272 |
| Pupillary Distance | 0.250 | 0.882 |
| Vision Right | 0.070 | 0.965 |
| Vision Left | 0.165 | 0.921 |
| Oblique Perspective | 1.596 | 0.450 |
| Fusion Range | 27.377 | <0.001 ** |
| Stereoacuity | 3.026 | 0.220 |
| Estimate Value | SE | OR | 95% CI | p-Value | ||
|---|---|---|---|---|---|---|
| ACL-I to Control | 1.070 | 0.450 | 2.915 | 1.207 | 7.038 | 0.017 * |
| ACL-I to Control | 2.417 | 0.449 | 11.213 | 4.654 | 27.014 | <0.001 ** |
| ACL-I to ACL-D | −0.042 | 0.020 | 0.959 | 0.922 | 0.998 | 0.040 * |
| ACL-I to ACL-D | −0.106 | 0.021 | 0.900 | 0.863 | 0.938 | <0.001 ** |
| Estimate Value | SE | OR | 95% CI | p-Value | ||
|---|---|---|---|---|---|---|
| Fusion Range | −0.059 | 0.019 | 0.943 | 0.907 | 0.979 | 0.003 ** |
| Action (Sprint) | 0.692 | 0.486 | 2.000 | 0.768 | 5.213 | 0.155 |
| Action (Quick Turn) | 1.413 | 0.421 | 4.107 | 1.829 | 9.555 | 0.001 ** |
| Action (Sudden Stop) | 2.478 | 0.692 | 11.914 | 3.317 | 52.010 | <0.001 ** |
| Action (Jump) | 1.500 | 0.454 | 4.483 | 1.876 | 11.195 | 0.001 ** |
| Action (Retrogress) | 0.321 | 0.557 | 1.378 | 0.451 | 4.072 | 0.565 |
| Action (Others) | 0.616 | 0.581 | 1.852 | 0.583 | 5.792 | 0.289 |
| Sudden Stop | Jump | Quick Tun | ||
|---|---|---|---|---|
| Cloud | Wooden floor | 13.208 | 4.439 | 3.482 |
| Plastic floor | 11.880 | 3.993 | 3.132 | |
| Cement floor | 11.872 | 3.990 | 3.130 | |
| Snow | Wooden floor | 12.962 | 4.356 | 3.417 |
| Plastic floor | 11.659 | 3.918 | 3.073 | |
| Cement floor | 11.651 | 3.916 | 3.071 | |
| Rain | Wooden floor | 11.782 | 3.960 | 3.106 |
| Plastic floor | 10.598 | 3.562 | 2.794 | |
| Cement floor | 10.591 | 3.560 | 2.792 |
| Sudden Stop | Jump | Quick Tun | ||
|---|---|---|---|---|
| Cloud | Wooden floor | 10.583 | 3.557 | 2.790 |
| Plastic floor | 9.519 | 3.199 | 2.509 | |
| Cement floor | 9.513 | 3.197 | 2.508 | |
| Snow | Wooden floor | 10.386 | 3.491 | 2.738 |
| Plastic floor | 9.342 | 3.140 | 2.463 | |
| Cement floor | 9.336 | 3.138 | 2.461 | |
| Rain | Wooden floor | 9.441 | 3.173 | 2.489 |
| Plastic floor | 8.492 | 2.854 | 2.239 | |
| Cement floor | 8.486 | 2.852 | 2.237 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Li, Y.; Zhang, Y.; Zhang, Z.; Wang, J.; Deng, X.; Liu, C.; Chen, N.; Jiang, C.; Li, W.; et al. Analysis of Visual Risk Factors of Anterior Cruciate Ligament Injury of Knee Joint. J. Clin. Med. 2022, 11, 5602. https://doi.org/10.3390/jcm11195602
Chen Z, Li Y, Zhang Y, Zhang Z, Wang J, Deng X, Liu C, Chen N, Jiang C, Li W, et al. Analysis of Visual Risk Factors of Anterior Cruciate Ligament Injury of Knee Joint. Journal of Clinical Medicine. 2022; 11(19):5602. https://doi.org/10.3390/jcm11195602
Chicago/Turabian StyleChen, Zhong, Yuheng Li, Yichi Zhang, Zhengzheng Zhang, Jingsong Wang, Xinghao Deng, Chengxiao Liu, Na Chen, Chuan Jiang, Weiping Li, and et al. 2022. "Analysis of Visual Risk Factors of Anterior Cruciate Ligament Injury of Knee Joint" Journal of Clinical Medicine 11, no. 19: 5602. https://doi.org/10.3390/jcm11195602
APA StyleChen, Z., Li, Y., Zhang, Y., Zhang, Z., Wang, J., Deng, X., Liu, C., Chen, N., Jiang, C., Li, W., & Song, B. (2022). Analysis of Visual Risk Factors of Anterior Cruciate Ligament Injury of Knee Joint. Journal of Clinical Medicine, 11(19), 5602. https://doi.org/10.3390/jcm11195602