All articles published by MDPI are made immediately available worldwide under an open access license. No special
permission is required to reuse all or part of the article published by MDPI, including figures and tables. For
articles published under an open access Creative Common CC BY license, any part of the article may be reused without
permission provided that the original article is clearly cited. For more information, please refer to
https://www.mdpi.com/openaccess.
Feature papers represent the most advanced research with significant potential for high impact in the field. A Feature
Paper should be a substantial original Article that involves several techniques or approaches, provides an outlook for
future research directions and describes possible research applications.
Feature papers are submitted upon individual invitation or recommendation by the scientific editors and must receive
positive feedback from the reviewers.
Editor’s Choice articles are based on recommendations by the scientific editors of MDPI journals from around the world.
Editors select a small number of articles recently published in the journal that they believe will be particularly
interesting to readers, or important in the respective research area. The aim is to provide a snapshot of some of the
most exciting work published in the various research areas of the journal.
Background/Objectives: CDK4/6i and ET improve outcomes in HR-positive, HER2-negative breast cancer, but their benefits differ between early-stage (EBC) and metastatic disease (MBC). We aimed to compare the efficacy and toxicity of CDK4/6i plus ET versus ET alone across these disease settings. Methods [...] Read more.
Background/Objectives: CDK4/6i and ET improve outcomes in HR-positive, HER2-negative breast cancer, but their benefits differ between early-stage (EBC) and metastatic disease (MBC). We aimed to compare the efficacy and toxicity of CDK4/6i plus ET versus ET alone across these disease settings. Methods: We conducted a meta-analysis of phase III randomized trials identified through MEDLINE, EMBASE, and Web of Science up to 1 October 2025. Twenty-two trials (18 MBC, n = 6364; 4 EBC, n = 17,741) met the inclusion criteria. Two reviewers extracted data and assessed risk of bias. The study followed PRISMA 2020 guidelines (PROSPERO: CRD420251132302). Outcomes included overall survival (OS), progression-free survival (PFS), invasive disease-free survival (iDFS), distant relapse-free survival (DRFS), response rates, treatment discontinuation (TDR), dose reductions (DRR), and grade 3–4 adverse events. Results: In MBC, CDK4/6i improved OS (HR: 0.78, 95% CI: 0.72–0.85) and PFS (HR: 0.53, 95% CI: 0.50–0.56) and increased objective response, clinical benefit, and disease control rates along with TDR, DRR, and grade 3–4 adverse events. In EBC, iDFS improved, whereas OS (HR: 0.92, 95% CI: 0.75–1.12; p = 0.40) and DRFS did not. TDR, DRR, and grade 3–4 adverse events were increased. Conclusions: CDK4/6i confer significant OS and PFS benefits in MBC, supporting first-line use. In EBC, no OS benefit was observed, and toxicity was increased, underscoring the need for individualized risk–benefit assessment. Longer follow-up is warranted to clarify survival outcomes.
Full article
by
Sina Makouie, Jolanta Małajowicz, Agata Gόrska, Iga Piasecka-Lenartowicz, Barbara Strojny-Cieślak, Michał Pruchniewski, Bartłomiej Zieniuk and Joanna Bryś
Milk thistle (Silybum marianum) oil production generates substantial quantities of seed cake, an underutilized by-product with potential as a source of nutrients and bioactive compounds. This study aimed to characterize milk thistle cakes from two industrial sources (MTC1 and MTC2) and
[...] Read more.
Milk thistle (Silybum marianum) oil production generates substantial quantities of seed cake, an underutilized by-product with potential as a source of nutrients and bioactive compounds. This study aimed to characterize milk thistle cakes from two industrial sources (MTC1 and MTC2) and their corresponding seeds (MTS1 and MTS2), focusing on compositional properties, fatty acid profile, and antioxidant activity assessed using the DPPH scavenging assay. Proximate analysis showed that the cakes retained significant residual oil (9.26–14.51 g 100 g−1) and protein (16–19 g 100 g−1), with low water activity (<0.33), indicating good storage stability. Fatty acid analysis revealed a predominance of polyunsaturated fatty acids (49–52%), mainly linoleic acid (C18:2 n-6), confirming their nutritional value. Differences between industrial sources indicated variability associated with raw material and processing conditions. Extraction solvent significantly affected bioactive compound recovery from the oil fraction. Dichloromethane extracts exhibited higher total phenolic content (up to 8.87 mg GAE g−1) and stronger DPPH radical scavenging activity (up to 28.07%) compared to hexane extracts, which may be attributed to a greater extraction of moderately polar phenolic compounds, including flavonolignan-type constituents potentially associated with silymarin complex. Overall, milk thistle cake represents a promising raw material for the recovery of natural antioxidants and valuable lipids, supporting its application in functional food or feed products and sustainable biorefinery processes.
Full article
The giant Dulong Sn-Zn polymetallic deposit, located in the eastern part of the southeastern Yunnan metallogenic belt, is a world-class ore system. Despite extensive research on the source of tin and its mineralization processes, the specific ore-related intrusion and the source of copper
[...] Read more.
The giant Dulong Sn-Zn polymetallic deposit, located in the eastern part of the southeastern Yunnan metallogenic belt, is a world-class ore system. Despite extensive research on the source of tin and its mineralization processes, the specific ore-related intrusion and the source of copper remain highly debated. Recent deep exploration has revealed a deep-seated granite porphyry, yet its geochronological and geochemical characteristics, along with its genetic link to mineralization, are poorly constrained. This study presents new zircon U-Pb age, whole-rock geochemistry, and Sr-Nd-Hf isotopic compositions of this granite porphyry, integrated with a regional comparison to multi-phase Laojunshan granites. LA-ICP-MS zircon U-Pb dating yields a Late Cretaceous age of 85.1 ± 1.2 Ma. The Dulong granite porphyry is strongly peraluminous and high-K calc-alkaline to shoshonitic, exhibiting typical S-type granite affinities with enrichment in Rb, U, and Ta, as well as depletions in Ba, Sr, Nb, and Eu. Isotopic signatures (εNd(t) = −12.5 to −12.0, tDM2(Nd) = 1.87 to 1.91 Ga; zircon εHf(t) = −10.24 to −1.44, tDM2(Hf) = 1.24 to 1.79 Ga) suggest that the parental magma was derived from the partial melting of ancient crust, with possible minor input of mantle-derived components in an extensional tectonic setting. The Dulong granite porphyry represents a moderate-to-high temperature, reduced, and highly evolved magmatic system. Notably, its high concentrations of Sn, W, Zn, and Cu indicate that the parental melt was metal-rich, possessing potential for Sn and Cu mineralization. Accordingly, future exploration should prioritize areas characterized by well-developed granite porphyry dykes, skarn–wallrock contact zones, and deep-seated structural intersections.
Full article
Comprehensive mechanized solid backfilling technology exhibits significant advantages in solid waste disposal, “three-under” coal mining, and dynamic disaster control. However, its large-scale application is constrained by low production efficiency, high unit production cost, and high labor intensity. Therefore, industrial upgrading through intelligent technologies
[...] Read more.
Comprehensive mechanized solid backfilling technology exhibits significant advantages in solid waste disposal, “three-under” coal mining, and dynamic disaster control. However, its large-scale application is constrained by low production efficiency, high unit production cost, and high labor intensity. Therefore, industrial upgrading through intelligent technologies is urgently required. In this study, methods including literature review, theoretical analysis, and field measurements are employed to propose three backfilling modes. The configurations of the six core subsystems under each mode are systematically summarized, and the core definition of an intelligent backfilling mine is established. Furthermore, a key technology framework for intelligent backfill mining is developed, based on PLC control and PID algorithms, with a closed-loop architecture centered on “perception–decision–execution.” Engineering applications demonstrate that the surface gangue intelligent pretreatment system achieves functions including automatic vehicle washing, intelligent dust suppression spraying at discharge points, dynamic metering during conveying, and adaptive adjustment of feeding systems. The intelligent surface-to-underground coal gangue vertical feeding system enables full silo alarm and level regulation. The underground jigging intelligent separation system realizes intelligent jigging ratio adjustment, intelligent bed layer measurement and control, and intelligent air volume regulation, with the coal content in gangue discharge maintained below 4%. At the working face, the intelligent solid backfilling system doubles monthly coal output, boosts backfilling efficiency by 50%, and cuts the workforce by 8–10 workers. The intelligent backfilling effectiveness monitoring system operates stably, with a working face weighting factor of 1.12 and precise ground deformation control within Grade I limits.
Full article
The article presents the synthesis and characterization of double halide perovskites (DHPs) with the nominal composition Cs2Ag0.2Na0.4In0.6M0.4Cl6 (M = Si, Ti, Zr), including photoluminescence (PL), photoluminescence excitation (PLE) spectra measured over a
[...] Read more.
The article presents the synthesis and characterization of double halide perovskites (DHPs) with the nominal composition Cs2Ag0.2Na0.4In0.6M0.4Cl6 (M = Si, Ti, Zr), including photoluminescence (PL), photoluminescence excitation (PLE) spectra measured over a range of temperatures and kinetics of luminescence. The materials were synthesized via a hydrothermal method. The phase purity and elemental composition of the synthesized perovskites were confirmed by X-ray diffraction (XRD), Rietveld refinement, scanning electron microscopy (SEM) equipped with energy-dispersive X-ray spectroscopy (EDS) and elemental analysis, which demonstrated that the samples showed a close match to the target stoichiometry. The PL spectra exhibit a systematic shift toward the lower-energy region with substitution from Si to Zr, correlating with the progressive increase in the ionic radii of the substituting cations. All samples display broad, asymmetric emission bands, characteristic of self-trapped excitonic (STE) states. Temperature-dependent PL measurements reveal a gradual decrease in emission intensity with increasing temperature for all samples. The maximum emission intensity is observed in the range of ~160–200 K, corresponding to optimal conditions for radiative recombination, whereas the lowest intensity is recorded at ~80–100 K, where thermal activation of radiative centers is minimal. An increase in temperature is accompanied by a red shift in the PL bands across all compositions. In the Ti-doped DHP, a pronounced blue shift at low temperatures is observed, which can be attributed to the involvement of Ti3+-related electronic states. An analysis of the activation energy of thermal luminescence quenching and the results of time-resolved spectroscopy revealed the activation of thermal processes in the titanium-containing sample and their rapid decay, whereas replacing titanium with silicon leads to more stable luminescence in the crystal under study. Thus, the enhanced luminescence characteristics of double halide perovskites doped with Ti, Si, and Zr highlight their potential for advanced photonic and optoelectronic applications.
Full article
Objective: Skeletal mandibular asymmetry (MA) is a pathological condition characterised by asymmetric mandibular growth, resulting in chin deviation and, in some cases, non-coincident dental midlines. Because it is a skeletal condition, some clinicians choose to treat it with functional appliances. The present study
[...] Read more.
Objective: Skeletal mandibular asymmetry (MA) is a pathological condition characterised by asymmetric mandibular growth, resulting in chin deviation and, in some cases, non-coincident dental midlines. Because it is a skeletal condition, some clinicians choose to treat it with functional appliances. The present study therefore evaluated whether functional appliances with asymmetric activation can promote more symmetrical growth of the mandibular condyles and rami. Methods: Eighty-five patients with MA were retrospectively selected based on cervical skeletal maturation stage 2 or 3, the presence of skeletal and dental Class II malocclusion, and the availability of good-quality orthopantomograms taken before and after treatment. Among the enrolled patients, 40 were treated with functional appliances to protrude and re-centre the mandible (study group), while 45 were treated only with a rapid maxillary expander (positive and treated control group). This control group was chosen because it has no direct effects on the mandible and avoided the ethical concerns associated with postponing time-sensitive treatment to recruit a negative control group. Ramus and condyle asymmetry were evaluated pre- and post-treatment using Habets’ method. The Mann–Whitney U-test was used to compare pre- and post-treatment asymmetry indices between the two groups. Results: Although both groups showed a post-treatment symmetry improvement, no statistically significant between-group differences were observed (p = 0.712, effect size r = 0.14 for ramal symmetry; p = 0.663, effect size r = −0.01 for condylar symmetry). Conclusions: Within the limitations of this study, functional appliances did not demonstrate greater skeletal effects than the positive control treatment.
Full article
Freezing effectively extends the shelf life of food and maintains product quality by inhibiting microorganisms, enzyme activity, and chemical reactions. However, issues such as ice crystal formation, protein denaturation, lipid oxidation, and the low-temperature adaptability of psychrophilic microorganisms during the freezing process can
[...] Read more.
Freezing effectively extends the shelf life of food and maintains product quality by inhibiting microorganisms, enzyme activity, and chemical reactions. However, issues such as ice crystal formation, protein denaturation, lipid oxidation, and the low-temperature adaptability of psychrophilic microorganisms during the freezing process can directly affect the final quality of frozen foods. Among these, the size and distribution of ice crystals are key factors determining the extent of tissue damage. Therefore, this review aims to identify innovative and optimized freezing and frozen storage strategies. In order to save energy and improve product quality, various new technologies have emerged in recent years, such as ultrasonic-assisted freezing, high-pressure freezing, and magnetic-field-assisted freezing. This study systematically discusses the principles, applications, and impact mechanisms of these technologies on frozen foods. Furthermore, this study proposes the future development trends of frozen foods, filling the gap in the current food industry where there is a lack of systematic discussion and evaluation of frozen foods. It provides technical support and research directions for continuous development and innovation in the field of frozen foods.
Full article
Unmanned aerial vehicles (UAVs) are increasingly expected to support both wireless communication and logistics missions, creating a need for integrated operation strategies that jointly manage data collection and physical item handling. This paper investigates a UAV system that simultaneously performs uplink communication with
[...] Read more.
Unmanned aerial vehicles (UAVs) are increasingly expected to support both wireless communication and logistics missions, creating a need for integrated operation strategies that jointly manage data collection and physical item handling. This paper investigates a UAV system that simultaneously performs uplink communication with multiple ground nodes (GNs) while completing time-constrained item-pickup tasks. To enhance both throughput and fairness across GNs, we maximize the proportional fair spectral efficiency of GNs while ensuring that all items are collected within the required mission duration under payload and geographical constraints. The resulting formulation constitutes a mixed-integer nonconvex optimization problem involving binary pickup assignments, binary communication scheduling, and trajectory-dependent channel coupling, making direct global optimization intractable. To address this challenge, we develop an iterative convexification framework that integrates the successive convex approximation and the penalty convex–concave procedure within a block coordinate descent structure, enabling efficient joint optimization of trajectory, pickup timing/sequence, and GN scheduling. Simulation results validate that the proposed scheme dynamically shapes the UAV trajectory to improve channel conditions without violating the pickup deadline and compensates disadvantaged GNs through proportional fair scheduling. As a result, it consistently outperforms the baseline strategies under various system parameters.
Full article
by
Alishah Ahmadi, Anthony J. Kaywood, Areeb Ansari, Alejandra Chavarria, Oserekpamen Favour Omobhude, Adam Kiss, Mateusz Faltyn and Jason S. Hoellwarth
J. Pers. Med.2026, 16(6), 280; https://doi.org/10.3390/jpm16060280 (registering DOI) - 24 May 2026
Background/Objective: Osteoarthritis (OA) is the most common indication for total hip arthroplasty (THA), yet postoperative utilization and discharge outcomes vary substantially due to heterogeneous comorbidity burdens. This study applied unsupervised machine learning clustering to identify distinct comorbidity profiles among OA patients undergoing
[...] Read more.
Background/Objective: Osteoarthritis (OA) is the most common indication for total hip arthroplasty (THA), yet postoperative utilization and discharge outcomes vary substantially due to heterogeneous comorbidity burdens. This study applied unsupervised machine learning clustering to identify distinct comorbidity profiles among OA patients undergoing THA and to evaluate their association with non-routine discharge (NRD) and length of stay (LOS). Methods: The 2015–2021 National Inpatient Sample was queried using ICD-10 CM/PCS codes to identify patients with OA undergoing THA. Forty-nine comorbidities, complications, and in-hospital clinical covariates were incorporated into a k-modes clustering analysis. The Davies–Bouldin and Calinski–Harabasz indices were used to determine the optimal number of clusters. Multivariable logistic regression assessed adjusted odds of NRD across clusters, and Kruskal–Wallis H testing evaluated differences in LOS. Results: A total of 401,846 patients were included, and five distinct clusters were identified, ranging from 777 to 331,755 patients. Clusters with higher prevalence of renal dysfunction, cardiovascular disease, anemia, and heart failure demonstrated significantly increased risk of NRD (adjusted odds ratios up to 3.01, p < 0.001) and prolonged hospitalization, with median LOS up to 4 days. Lower-risk clusters exhibited shorter hospitalizations with median LOS of 2 days and higher rates of routine discharge. Kruskal–Wallis testing confirmed significant LOS differences across all clusters (p < 0.001). Conclusions: Machine learning clustering of OA patients undergoing THA identified clinically distinct subgroups with graded differences in postoperative hospital utilization. Patients with greater comorbidity burden experienced disproportionately higher risk of NRD and prolonged LOS. This data-driven framework highlights heterogeneity within the OA population and may inform future strategies for perioperative risk stratification and resource planning.
Full article
Two-stage anaerobic digestion systems are extensively researched for enhancing process stability and phase separation when processing complex organic materials. Scaling from laboratory setups to pilot plants necessitates engineering modifications to ensure operational feasibility. In this study, a laboratory-scale system comprising a 100 L
[...] Read more.
Two-stage anaerobic digestion systems are extensively researched for enhancing process stability and phase separation when processing complex organic materials. Scaling from laboratory setups to pilot plants necessitates engineering modifications to ensure operational feasibility. In this study, a laboratory-scale system comprising a 100 L horizontal CSTR and a packed-bed reactor was scaled up 100-fold. The design separates solid and liquid retention times, with fibers retained in the first stage while liquids and volatile fatty acids flow into the second. Fiber retention in the lab was achieved using a 100 µm sieve dividing the CSTR into two chambers, allowing prolonged lignocellulosic degradation. During scale-up, a filtration and recirculation system was introduced, able to return the fibers to the first reactor through a 1000 µm edge-gap filter, which separates liquids for the second reactor and recycles undegraded fibers. An economic analysis indicated a scale-up exponent of 0.396, indicating that unit costs decrease with plant size and demonstrating economies of scale. Laboratory-based mass balance estimates biogas production at approximately 16.3 m3 daily at the pilot scale, equivalent to 90 kWh. The modular system aims to be transferred to small farms, promoting cost-effective biogas from manure and local residues to support decentralized renewable energy in agriculture.
Full article
Controlling pollutant dispersion in high-rise buildings is crucial for public health. Vertical pollutant diffusion in stairwells occurs under thermal and wind effects. However, most existing studies rely on idealized boundary conditions. To address this, this study uses field-measured wall temperatures and a window
[...] Read more.
Controlling pollutant dispersion in high-rise buildings is crucial for public health. Vertical pollutant diffusion in stairwells occurs under thermal and wind effects. However, most existing studies rely on idealized boundary conditions. To address this, this study uses field-measured wall temperatures and a window wind velocity as boundary conditions for transient CFD simulations. We investigate the vertical diffusion characteristics of buoyant (CH4) and dense (CO2) pollutants under thermal pressure, window velocity, and wind–thermal coupling in a high-rise residential building in Taiyuan. Results show an asymmetric “fast-up, slow-down” diffusion under thermal pressure, a relatively symmetric profile under window velocity, and a hybrid pattern under coupling where the upper region is wind-dominated and the lower region resembles thermal-driven diffusion. Wind–thermal coupling most significantly enhances upward diffusion. Using the arrival time of CH4 at the 28th floor (about 15 m above the source floor) as the benchmark, the diffusion rate under coupling is about 200% faster than under thermal pressure alone, and about 50% faster than under the window-velocity condition alone. Differences in density lead to variations in dispersion, with CH4 exhibiting higher rates, concentrations (2–4 orders greater), and a broader influence range than CO2. This work interprets the synergistic regulatory mechanism between driving forces and pollutant density, providing a theoretical basis for ventilation optimization and pollution control in high-rise buildings.
Full article
by
Nan Shen, Wenwen Wang, Jipan Zhang, Huawei Rong, Xinghao Qu, Muhammad Javid, Muhammad Farooq Saleem, Xiang Li, Muhammad Irfan, Sateesh Bandaru, Xuefeng Zhang and Gulmira Mustafayeva
Nanomaterials2026, 16(11), 663; https://doi.org/10.3390/nano16110663 (registering DOI) - 24 May 2026
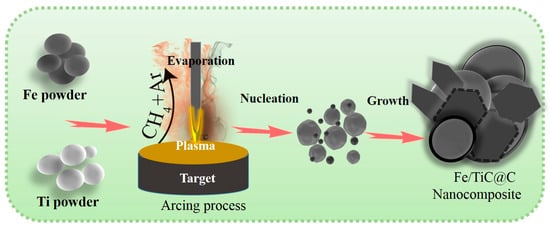
The development of cost-effective and resource-rich materials is crucial for the practical application of microwave absorbers. This study demonstrates the successful fabrication of core-shell Fe and TiC nanoparticles encapsulated within carbon shells using the arc discharge method. The samples are designated as Fe3Ti1
[...] Read more.
The development of cost-effective and resource-rich materials is crucial for the practical application of microwave absorbers. This study demonstrates the successful fabrication of core-shell Fe and TiC nanoparticles encapsulated within carbon shells using the arc discharge method. The samples are designated as Fe3Ti1 and Fe1Ti3, where the numbers indicate the Fe-to-Ti mass ratio in the precursor (e.g., Fe1Ti3 = 1:3 by mass). In the arc discharge synthesis mechanism, the mass ratio of Fe to Ti in the raw material was adjusted from 3:1 to 1:3 to optimize the Fe/TiC/C interfaces under a CH4 forming gas atmosphere. TEM analysis reveals spherical and polyhedral nanoparticles with diameters of 30–50 nm and a uniform carbon shell thickness of 3–4 nm. Raman spectroscopy shows that the Fe1Ti3 sample has a higher defect density (ID/IG = 1.13) compared to Fe3Ti1 (0.87), indicating a more disordered carbon structure. Magnetic measurements yield saturation magnetization values of 87 emu/g for Fe3Ti1 and 50 emu/g for Fe1Ti3, with coercivities of 190.72 Oe and 203.65 Oe, respectively. When composited with paraffin at 50 wt% loading, the Fe1Ti3 sample exhibits superior microwave absorption performance, achieving a minimum reflection loss (RL) of −25.22 dB at 8.23 GHz and an effective absorption bandwidth (RL ≤ −10 dB) of 4 GHz (6.5–10.5 GHz) at a thickness of 2.5 mm. This enhanced performance is attributed to the synergistic effect of multiple loss mechanisms, including conduction loss within the three-dimensional core-shell architecture, interfacial polarization at the heterojunctions between the core and the carbon shell, and magnetic loss induced by ferromagnetic behavior associated with defects in both the shell and carbon atomic layers. The magnetic loss in the (Fe/TiC)@C nanocomposites primarily arises from the natural resonance (at ~6.5 GHz) and exchange resonance (at ~12 GHz) of the Fe cores. The dielectric loss is primarily attributed to dipole, interfacial, and space charge polarization from TiC and the carbon shell, as well as multiple scattering effects between nanoparticles. Furthermore, far-field radar cross-section simulations substantiate that the Fe/TiC@C nanocomposite demonstrates excellent radar wave attenuation capability. Further, first principles simulations reveal that introducing Fe at the C/TiC interface induces strong charge redistribution and orbital hybridization, transforming a localized dielectric interface into a highly conductive and electronically coupled C/Fe/TiC system. This interfacial modulation enhances both dielectric loss (via charge transport and polarization) and magnetic loss (via Fe-induced magnetic interactions), thereby enabling optimized dielectric-magnetic synergy for broadband microwave absorption in (Fe/TiC)@C nanocomposites.
Full article
In padel, an emerging racket sport, evidence regarding competition demands in adolescent players remains limited. Therefore, this study aimed to analyze absolute external load during official competition in male and female U18 padel players. A total of 18 official matches from the Spanish
[...] Read more.
In padel, an emerging racket sport, evidence regarding competition demands in adolescent players remains limited. Therefore, this study aimed to analyze absolute external load during official competition in male and female U18 padel players. A total of 18 official matches from the Spanish Championship of Regional Teams were analyzed. Eighteen U18 players (9 females: age 15.1 ± 1.5 years, height 162.9 ± 8.2 cm, body mass 54.6 ± 9.1 kg; 9 males: age 15.4 ± 1.8 years, height 175.1 ± 9.4 cm, body mass 67.2 ± 11.0 kg), competing at the regional and national levels, were monitored using OLIVER™ inertial devices. External load variables included playing time, total distance, high-intensity accelerations and decelerations, changes of direction, time spent at high metabolic power, session volume, session intensity, and maximum speed. Statistical analysis was performed using linear mixed models to compare differences between sexes. Male players showed significantly higher values than female players in playing time (82.34 ± 23.95 vs. 51.03 ± 12.39 min; p < 0.001) and total distance (3958.50 ± 242.57 vs. 2225.54 ± 257.29 m; p < 0.001). They also presented significantly greater values in high-intensity external load variables, including accelerations, decelerations, changes of direction, time spent at high metabolic power, session volume, and session intensity (all p ≤ 0.009). No significant differences were found for maximum speed (p = 0.074). These findings suggest that official competition demands differ according to sex in U18 padel and may help inform more specific training prescriptions and load-monitoring strategies.
Full article
In vitro cultured plant calli, induced through dedifferentiation, are colonized by diverse endophytes. Most of these endophytes, being substantially inherited from the mother plant and highly dependent on the host’s internal ecological niche, are termed host-dependent endophytes (HDEs). Due to their close association
[...] Read more.
In vitro cultured plant calli, induced through dedifferentiation, are colonized by diverse endophytes. Most of these endophytes, being substantially inherited from the mother plant and highly dependent on the host’s internal ecological niche, are termed host-dependent endophytes (HDEs). Due to their close association with their hosts, HDEs exhibit heritable characteristics. However, our current understanding of plant HDEs and their effects on the host plant is limited. In this study, we characterized the composition and potential functions of the endophytic microbiota in grapevine calli derived from different varieties and organs corresponding to Cabernet Sauvignon berry flesh (CF), Rose Honey berry flesh (RF), and Rose Honey shoot tip (RS) using high-throughput sequencing and bioinformatics. Our results showed that the genotype and organotype of the explant did not affect the alpha diversity of endophytes in callus, but were associated with differences in beta diversity and community structure of the endophytic microbiota. Different types of grapevines calli inherited distinct endophytes from their mother plants, whereas sharing a conservative core endophytic microbiota consisting of a small number of amplicon sequence variants (ASVs) with high relative abundances (bacteria: 38 ASVs ranging from 79 to 92%; fungi: 9 ASVs ranging from 32 to 58 prediction analyses using revealed conserved functional traits of the endophytic microbiota across callus types, including a core suite of bacterial adaptive phenotypes, stable central metabolism dominated by oxidative phosphorylation, and uniformly structured fungal communities dominated by saprotrophs and pathotrophs, while consistently containing yeast-form fungi. Although minor variations such as elevated trait abundance in the CF group were noted, no statistically significant functional divergence was observed, demonstrating that the endophytic microbiota of grapevine callus maintains a conserved functional profile across different types. Collectively, this study provides a methodological framework for investigating plant HDEs and offers new insights into host-endophyte interactions at the cellular level.
Full article
Fused Filament Fabrication (FFF) is a widely used additive manufacturing technology due to its versatility, low cost, and broad material compatibility. However, achieving high dimensional accuracy in FFF parts remains challenging because dimensional deviations are affected by material shrinkage, process parameters, and part
[...] Read more.
Fused Filament Fabrication (FFF) is a widely used additive manufacturing technology due to its versatility, low cost, and broad material compatibility. However, achieving high dimensional accuracy in FFF parts remains challenging because dimensional deviations are affected by material shrinkage, process parameters, and part geometry. This study analyses the dimensional deviations of PLA hollow cylindrical specimens manufactured by FFF, with particular attention to the different behaviour of outer and inner diameters. The methodology combines an iterative design-adjustment procedure with a neural-network-based compensation approach. First, specimens with different geometries were printed and measured to evaluate the evolution of dimensional error after successive design corrections. Then, the influence of print speed and layer thickness was analysed through the volumetric material flow rate, and the resulting data were used to train separate feedforward neural networks for the outer and inner diameters. The results showed that outer and inner diameters followed different deviation trends, confirming that they should be analysed independently. Print speed, layer thickness, and material flow affected dimensional accuracy in different ways depending on the measured diameter. The proposed neural network approach provided a practical means of estimating compensated design diameters within the experimental domain analysed, reducing the need for repeated trial and error adjustments. However, the results should be interpreted within the experimental limits of the study, particularly regarding the use of a single material, a single printer, and a limited validation dataset. Overall, the study provides a practical workflow for improving dimensional accuracy in FFF parts and highlights the importance of diameter-specific compensation strategies.
Full article
We develop an operational, measurement-first framework for the geometry of locally finite cell complexes, in which length is defined as a count of face crossings, and curvature is read off from the discrepancy between a measured radius and a radius reconstructed from boundary,
[...] Read more.
We develop an operational, measurement-first framework for the geometry of locally finite cell complexes, in which length is defined as a count of face crossings, and curvature is read off from the discrepancy between a measured radius and a radius reconstructed from boundary, area, or volume counts using the same yardstick. We prove that the count metric is geodesic on every locally finite complex, and we introduce a unified small-ball/small-sphere curvature estimator that is valid in dimensions two through four with a single closed-form expression. By comparison with the standard small-ball volume expansion of a smooth conformal metric , we establish a quantitative identification theorem with explicit rate , which optimizes to at . We extend the construction to directional (sectional) estimators via Fermi tubes around geodesic two-slices, assemble the curvature operator, Ricci tensor, and scalar curvature in three dimensions, and prove a measured Gromov–Hausdorff convergence theorem for the rescaled count metric. All hypotheses are verified explicitly on Voronoi complexes of conformal metrics. Throughout, we are explicit that the discrete construction is interpreted via, and its asymptotic validity is established by comparison with, the smooth Riemannian theory; the contribution is the unified counts-only protocol with rigorous convergence rates, not a reformulation of curvature itself.
Full article
The genus Burkholderia encompasses both plant pathogenic and beneficial species, yet the genomic determinants underlying this lifestyle divergence remain poorly understood. Using 16S rRNA sequencing of 100 rice cultivars, our companion study demonstrated that resistant varieties are enriched in beneficial Burkholderiaceae, leading
[...] Read more.
The genus Burkholderia encompasses both plant pathogenic and beneficial species, yet the genomic determinants underlying this lifestyle divergence remain poorly understood. Using 16S rRNA sequencing of 100 rice cultivars, our companion study demonstrated that resistant varieties are enriched in beneficial Burkholderiaceae, leading to the isolation of three phenotypically contrasting strains. Here, we present comparative genomic analyses of non-pathogenic biocontrol strain Burkholderia vietnamiensis J14EpLeaf2 and pathogenic strains Burkholderia gladioli A1EpSeed5 and Burkholderia cepacia J14Eple. Pathogenic strains possess significantly larger genomes (8.36–8.46 Mb) enriched in mobile genetic elements compared to the streamlined 6.95 Mb genome of B. vietnamiensis. CAZyme analysis revealed broader repertoires of glycoside hydrolases and polysaccharide lyases in pathogens, consistent with enhanced plant cell wall degradation. B. gladioli possesses a complete T3SS and expanded T6SS with 301 predicted effectors, while B. cepacia lacks structural T3SS genes but harbors 271 candidate effectors predicted to be secreted via alternative secretion pathways, compared to 180 in B. vietnamiensis. Notably, B. cepacia harbors cystic fibrosis-associated markers (cable pili, ZmpA/ZmpB), raising significant biosafety concerns that preclude its agricultural application. LC-MS validated IAA, ornibactin, and AHL production in B. vietnamiensis, supporting its plant growth-promoting and biocontrol functions. Computational PPI networks predicted distinct interaction landscapes requiring experimental validation. This study provides a genomic framework for distinguishing pathogenic from beneficial Burkholderia and supports B. vietnamiensis as a safe biocontrol agent while cautioning against B. cepacia J14Eple.
Full article
Quantitative evaluation of the interfacial contact characteristics between the cathode active material (CAM) and solid electrolyte (SE) in all-solid-state battery (ASSB) composite cathodes is essential for improving electrochemical performance. In this study, a previously proposed integrated galvanostatic method (GM)-electrochemical impedance spectroscopy (EIS) framework
[...] Read more.
Quantitative evaluation of the interfacial contact characteristics between the cathode active material (CAM) and solid electrolyte (SE) in all-solid-state battery (ASSB) composite cathodes is essential for improving electrochemical performance. In this study, a previously proposed integrated galvanostatic method (GM)-electrochemical impedance spectroscopy (EIS) framework for analyzing the electrochemically active area (EAA) was applied to particle-size-controlled composite cathodes to examine how particle-size design influences interfacial contact in practical ASSB composite cathodes. Specifically, three cathodes were examined: a small-particle Ni-rich layered oxide cathode (SP), a large-particle Ni-rich layered oxide cathode (LP), and a bimodal cathode containing an equal-weight mixture of the two particle fractions (BP). An area-independent lithium diffusion coefficient was first determined from the Warburg-blocking transition in the impedance response. The EAA of each cathode was then obtained by combining this reference value with the area-sensitive galvanostatic response in a one-step constraining procedure. Although bimodal particle-size distributions are often expected to improve interfacial contact by combining the advantages of small and large particles, the EAA increased in the order of SP < BP < LP. This result indicates that under the present electrode configuration, the LP cathode secured the most effective CAM–SE interfacial contact and the highest effective surface coverage. Consistent with this trend, the LP cathode exhibited the best rate capability under high-rate conditions. These results demonstrate that the GM–EIS-based EAA analysis framework provides a practical quantitative tool for evaluating particle-size-dependent interfacial contact and guiding microstructure optimization in ASSB composite cathodes.
Full article
Urban environments in developing countries remain affected by legacy asbestos-containing materials, yet integrated assessments of multi-pathway asbestos release and environmental mobilization integrated with demographic distribution remain limited. This study aimed to develop a spatially explicit framework to assess environmental deterioration and asbestos-related environmental
[...] Read more.
Urban environments in developing countries remain affected by legacy asbestos-containing materials, yet integrated assessments of multi-pathway asbestos release and environmental mobilization integrated with demographic distribution remain limited. This study aimed to develop a spatially explicit framework to assess environmental deterioration and asbestos-related environmental hazard where multiple asbestos release pathways converge in a post-ban urban setting, using Cartagena, Colombia, as a case study. A multi-pathway approach was implemented, combining source characterization of asbestos-cement (AC) roofs through microvacuum sampling, analysis of roof runoff and drinking water, spatial distribution of AC pipelines, and demographic data at the neighborhood scale. A total of 72 roof surface samples were collected, of which 92% showed detectable asbestos fibers, with concentrations reaching up to 326 × 106 structures/cm2. Runoff water analysis indicated 85% detection, with average concentrations of 3.5 ± 3.14 million fibers per liter (MFL). Drinking water samples showed 11% positivity, with lower concentrations (mean 1.01 ± 1.59 MFL). Spatial analysis revealed that approximately 9.5% of the urban area exhibited high airborne release potential and 3.1% exhibited high runoff-related hazard, while integrated spatial prioritization identified 5.59% of the city as high priority for intervention. Results indicated that less deteriorated roofs exhibited higher surface fiber availability, suggesting that emission potential is not directly proportional to visible degradation. The integration of environmental and demographic data supported the identification of critical hotspots where multiple asbestos release pathways converge. The proposed methodology provides a novel framework for multi-pathway asbestos spatial prioritization in urban environments and highlights the need for source-based monitoring approaches. These findings support the development of targeted mitigation strategies in cities with widespread legacy asbestos infrastructure.
Full article
Existing deep-learning-based motor imagery (MI) electroencephalogram (EEG) decoding methods face challenges in generalizing across sessions and providing channel-level physiological interpretability. These limitations hinder the practical application of MI-EEG systems. Accordingly, DO-PI-EATCNet (Dream-Optimization-Enhanced, Physics-Inspired, Efficient-Attention Temporal Channel Network) is proposed to improve generalization and
[...] Read more.
Existing deep-learning-based motor imagery (MI) electroencephalogram (EEG) decoding methods face challenges in generalizing across sessions and providing channel-level physiological interpretability. These limitations hinder the practical application of MI-EEG systems. Accordingly, DO-PI-EATCNet (Dream-Optimization-Enhanced, Physics-Inspired, Efficient-Attention Temporal Channel Network) is proposed to improve generalization and interpretability in MI-EEG classification. Unlike models that simply combine multiple components, DO-PI-EATCNet assigns distinct roles to feature representation, temporal channel modeling, temporal regularization, and channel compactness. Latent-Projected Attention (LPA) enhances spatiotemporal discriminability by aligning attention in a low-dimensional latent space, and Temporal Channel Cascaded Collaborative Attention (TCCA) refines dependencies between time and channels. Fractional-Order Difference Temporal Consistency Loss (FD-TCL) is introduced as a neurodynamics-inspired temporal regularizer to reduce high-frequency fluctuations in prediction sequences and improve within-subject cross-session prediction stability. The Multi-Population Dream Optimization Algorithm (MPDOA) is used for channel selection to obtain a compact EEG channel subset and reduce computational load, although it introduces a slight accuracy decrease compared with the uncompressed full model. Under a within-subject cross-session protocol on the BCI Competition IV-2a four-class MI dataset, the final compact model achieves an average accuracy of 84.4% and Cohen’s κ of 0.790, outperforming the reimplemented baselines. Compared with the uncompressed LPA-TCCA-FD-TCL variant, MPDOA slightly decreases accuracy from 84.9% to 84.4%, but reduces EEG channels from 22 to about 15 and decreases MACs by 27%. Scalp topographies and selected-channel visualizations provide qualitative support for channel-level anatomical plausibility, as the selected electrodes are mainly located over expected sensorimotor-related regions, while t-SNE offers a descriptive visualization of the learned feature distributions.
Full article
Building cost-effective homes that comply with stringent environmental regulations remains a significant challenge for the UK housebuilding sector, particularly for social housing providers. In the context of net zero targets and reducing embodied carbon, this study examines opportunities to minimise material waste and
[...] Read more.
Building cost-effective homes that comply with stringent environmental regulations remains a significant challenge for the UK housebuilding sector, particularly for social housing providers. In the context of net zero targets and reducing embodied carbon, this study examines opportunities to minimise material waste and associated impacts. Using an inductive mixed-methods approach, the research began with a literature review to establish baseline waste rates across key material streams. It then analysed material usage data from three completed housing developments, comparing estimated quantities with actual orders and spend to identify discrepancies between assumptions and real-world outcomes. To validate these findings, a controlled case study tracked the construction of a single four-bedroom home, enabling direct measurement of waste rates and assessment of cost and carbon implications at unit level. Results highlight a series of marginal gains achievable through improved estimating and procurement practices, which collectively offer potential for significant financial savings and reductions in embodied carbon when scaled nationally. For social housing providers, these efficiencies could lower build costs, support sustainability goals, and create opportunities to reinvest in additional housing delivery.
Full article
Waste from the fruit juice industry presents high sugar and phenolic contents, high humidity and biological activities and cumbersome disposal or low-added valorization. Orange-peel waste (OPW) represents 35–55% w/w of processed fruit, with oranges being the main citric crop. OPW saccharification
[...] Read more.
Waste from the fruit juice industry presents high sugar and phenolic contents, high humidity and biological activities and cumbersome disposal or low-added valorization. Orange-peel waste (OPW) represents 35–55% w/w of processed fruit, with oranges being the main citric crop. OPW saccharification leads to sugar-rich hydrolysates that can be further processed via fermentative and catalytic routes. In this work, OPW enzymatic hydrolysis was studied via batch and fed-batch processing using either a 50 mM citrate buffer or a 9 g/L NaCl solution with pH control by adding CaCO3 to ensure high enzyme activity across the enzymatic process. Preliminary runs showed that particle size of 3.4 mm diameter and a 300 r.p.m. stirring speed, a six-blade Rushton turbine and wall baffles were adequate to reach high sugar yields in batch. Further scale-up in batch at medium solid loading (12.5% w/w) and fed-batch operation at high-solid loading (20% w/w) led to high yields and glucose and fermentable sugars (up to 74 and 136 g/L, respectively, when using the saline solution and CaCO3 as pH-controlling agent, in only 50 h; notably shorter and higher than when using the citrate buffer). Fractal kinetic models have been shown to accurately represent the compositional change across all batch and fed-batch conditions, highlighting NaCl reaction medium and alkali-driven pH control as the most appropriate approach to achieve high yields at low process times, a promising result for further developments at demonstration and industrial scales using automatic pH control.
Full article
by
Giordano Mayer De Freitas, Guilherme Teixeira Lopes, Graziele Borges Bueno, Mariana Lentino Coelho, Julia Gomes, Caroline Leffa Venturini, Maria Eduarda Louzada, Sara Machado Peres, Barbara Regina França, Iraci L. S. Torres Pham, Felipe Fregni, Andrea Cristiane Janz Moreira and Wolnei Caumo
Eur. J. Investig. Health Psychol. Educ.2026, 16(6), 72; https://doi.org/10.3390/ejihpe16060072 (registering DOI) - 24 May 2026
Background: Work disability in fibromyalgia is only partially explained by symptom severity, suggesting a relevant contribution of cognitive–behavioral mechanisms. Objective: This study aimed to determine whether kinesiophobia is associated with fibromyalgia impact and work-related disability and to assess whether pain catastrophizing mediates these
[...] Read more.
Background: Work disability in fibromyalgia is only partially explained by symptom severity, suggesting a relevant contribution of cognitive–behavioral mechanisms. Objective: This study aimed to determine whether kinesiophobia is associated with fibromyalgia impact and work-related disability and to assess whether pain catastrophizing mediates these relationships within a hierarchical biopsychosocial framework. Methods: This cross-sectional study included 2096 women with fibromyalgia recruited through a nationwide online survey. Participants completed validated instruments assessing fibromyalgia impact (FIQ), pain catastrophizing (PCS), depressive symptoms (PHQ-9), central sensitization (CSI), and kinesiophobia (Tampa Scale). Pain-related work disability was defined using the Graded Chronic Pain Scale–Revised (GCPS-R). Hierarchical logistic regression models identified factors independently associated with work disability. Mediation was tested using bootstrapped analyses (5000 resamples). Results: Kinesiophobia demonstrated a robust independent association with work disability (OR 1.03; 95% CI 1.02–1.05) after adjustment for sociodemographic factors, clinical pain phenotype, systemic burden, pain severity, psychocognitive load, and medication burden. Other relevant contributors included pain severity (OR 1.96; 95% CI 1.70–2.27), psychocognitive burden (OR 1.35; 95% CI 1.15–1.58), use of benzodiazepines (OR 1.74; 95% CI 1.33–2.28), and opioid use (OR 1.29; 95% CI 1.06–1.56). Mediation analysis indicated a significant indirect effect of kinesiophobia on work disability through pain catastrophizing (β = 0.131; 95% CI 0.078–0.188). Conclusions: Kinesiophobia is a proximal determinant of work disability in fibromyalgia, exerting direct and cognitively mediated effects through pain catastrophizing, reinforcing the fear-avoidance framework and the need for psychologically informed rehabilitation.
Full article
The digital economy has changed the way agricultural production is organized and how rural households access markets, jobs, and information. Yet it remains unclear whether these changes translate into higher income for rural residents, especially in major agricultural regions. This study examines the
[...] Read more.
The digital economy has changed the way agricultural production is organized and how rural households access markets, jobs, and information. Yet it remains unclear whether these changes translate into higher income for rural residents, especially in major agricultural regions. This study examines the income effect of digital infrastructure development by using the rollout of the Broadband China policy as a quasi-natural experiment. The analysis draws on panel data for 77 prefecture-level administrative units in the Yellow River Basin, one of China’s major agricultural regions, from 2009 to 2021. A staggered difference in differences model is used to estimate the policy effect. The results show that digital infrastructure development significantly increases rural residents’ income. Under the log income specification, the baseline coefficient indicates an average income increase of about 8.33%. The mechanism analysis shows that innovation capacity and nonfarm employment both serve as positive partial transmission channels, with innovation capacity explaining a larger share of the total effect. The heterogeneity results suggest that the income effect is stronger in regions with higher GDP and larger population size. These findings indicate that digital infrastructure can support rural income growth when it is linked with local innovation capacity, employment opportunities outside agriculture, and rural development policies suited to local conditions.
Full article
Self-assembling β-sheet-forming peptides are attractive building blocks for drug delivery nanomaterials. However, their strong intermolecular interactions often lead to high structural stability, which can hinder intracellular dissociation and limit cargo availability. Here, we propose a charge-compensated ampholytic design strategy for β-sheet peptide nanofibers
[...] Read more.
Self-assembling β-sheet-forming peptides are attractive building blocks for drug delivery nanomaterials. However, their strong intermolecular interactions often lead to high structural stability, which can hinder intracellular dissociation and limit cargo availability. Here, we propose a charge-compensated ampholytic design strategy for β-sheet peptide nanofibers that undergo destabilization and disassembly under reducing conditions. Six ampholytic peptides comprising an anionic main-chain peptide (β-sheet-forming motif, model antigenic cargo, and oligoglutamic acid segment) and a disulfide-linked cationic segment were designed and synthesized to vary the lengths and charges of the anionic and cationic segments, as well as the cationic insertion position. Four peptides formed nanofibers in 4×phosphate buffered saline (4×PBS) and the resulting nanofibers remained stable after dilution to 1×PBS, retaining β-sheet-rich secondary structures and fibrillar morphologies for at least 24 h. Under reducing conditions, the four preformed nanofibers exhibited distinct behaviors, including reduction-insensitive persistence, disassembly, and transient destabilization followed by re-stabilization, depending on peptide charge design. Redox-triggered disassembly was favored when the main-chain peptide had sufficient anionic character and the cationic segment was of moderate length and charge. This study therefore provides a molecular design strategy for controlling the destabilization of β-sheet peptide nanofibers under reducing conditions through disulfide-cleavage-induced disruption of charge compensation.
Full article
Equine infectious anemia virus (EIAV), with the simplest lentiviral genome, is a key model for studying fundamental lentiviral biology. Infectious viral particles are produced only when the Gag protein selectively encapsidates full-length genomic RNA via the packaging signal (Psi), yet the structural and
[...] Read more.
Equine infectious anemia virus (EIAV), with the simplest lentiviral genome, is a key model for studying fundamental lentiviral biology. Infectious viral particles are produced only when the Gag protein selectively encapsidates full-length genomic RNA via the packaging signal (Psi), yet the structural and functional features of EIAV Psi remain poorly characterized. Using computational prediction and dimethyl sulfate probing, we identified four stem-loops (SLs) within a ~120 nt region in the 5′ leader of the genome, spanning from downstream of the primer binding site through 20 nt into the gag coding sequence. In vitro dimerization assays demonstrated that a palindromic sequence (5′-CUGGCCAG-3′) within SL3 acts as a critical determinant of RNA dimerization. Functional screening using both an EIAV pseudovirus packaging system and the infectious clone EIAVuk revealed that deletion or mutation of the stem-loops significantly impairs viral packaging and replication, with SL2 deletion or its stem disruption causing the most severe defects. RNA-seq analysis of RNAs bound by wild-type Gag versus a zinc-finger mutant (H391K/H410K) identified two candidate Gag-associated sites: the SL2 stem and the SL2-SL3 junction. Targeting these regions with phosphorothioate-modified antisense oligonucleotides potently inhibited pseudovirus production and the replication of infectious EIAVuk. Our findings defined the secondary structure and functional organization of the EIAV core packaging region and established the SL2 stem and SL2-SL3 junction as candidate packaging determinants and promising targets for RNA-based antiviral intervention.
Full article














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}